{kind=link}
| Author | Affiliation |
|---|---|
| Ryan Roten, DO | Desert Regional Medical Center, Department of Emergency Medicine, Palm Springs, California |
| Ryan Peterfy, DO | Desert Regional Medical Center, Department of Emergency Medicine, Palm Springs, California |
CASE PRESENTATION
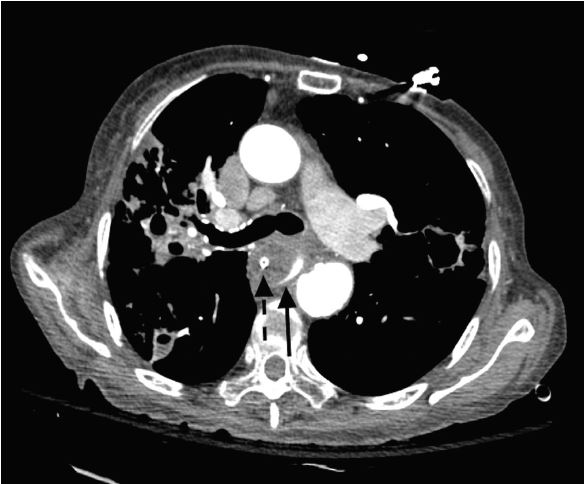
A 90-year-old female presented after sudden collapse with a Glasgow Coma Score of 3, and profound hypotension. Shortly after endotracheal intubation, the patient developed significant hematemesis, and massive transfusion protocol was subsequently instituted. Computed tomography angiogram of the chest revealed active bleeding from an aortoesophageal fistula (Image 1). During the resuscitation, over four liters of blood were collected via oral gastric tube and manual suctioning by nursing staff before the resuscitation was terminated at the family’s request.

DISCUSSION
The most common causes of aortoesophageal fistulas are thoracic aortic aneurysm, foreign body ingestion, postoperative complications, and esophageal malignancy. The classic presentation of mid-thoracic chest pain and sentinel arterial hemorrhage followed by exsanguination is known as Chiari’s triad.1 If the abnormality is identified early during the asymptomatic period using endoscopy or computed tomography angiogram of the chest, survival is possible with immediate surgical intervention or endovascular stenting.2 Medical providers must be familiar with the presentation, diagnostics, rapid interruption of diagnostics and treatment of aortoesophageal fistulas to make survival of this rare and typically fatal pathology possible.
CPC-EM Capsule
What do we already know about this clinical entity?
Aortoesophageal fistula is a rare and typically fatal pathology that presents as massive upper gastrointestinal hemorrhage.
What is the major impact of the image(s)?
This is a rarely seen image, given the degree of extremis and high mortality of patients with aortoesophageal fistula at emergency department presentation.
How might this improve emergency medicine practice?
Emergency medicine providers must be familiar with the presentation, diagnostics, rapid interruption of diagnostics and treatment of aortoesophageal fistulas.
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Address for Correspondence: Ryan Roten, DO, Desert Regional Medical Center, 1150 N. Indian Canyon Dr., Palm Springs, CA 92262. Email: ryanroten@cep.com. 1:260 – 261
Submission history: Revision received November 16, 2016; Submitted February 10, 2017; Accepted February 22, 2017
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Heckstall RL, Hollander JE. Aortoeophageal fistula: recognition and diagnosis in the emergency department. Ann Emerg Med. 1998;32(4):502-5.
2. Ayyildiz T, Nas OF, Yildirum C, et al. A rare upper gastrointestinal system case: aortaesophageal fistula. J Exp Clin Med. 2014;31:51-3.