
{kind=link}
| Author | Affiliation |
|---|---|
| William L. Fernandez, MD | University of Maryland Medical Center, Department of Emergency Medicine, Baltimore, Maryland |
| Laura J. Bontempo, MD, MEd | University of Maryland School of Medicine, Department of Emergency Medicine, Baltimore, Maryland |
| Zachary D.W. Dezman, MD, MS, MS | University of Maryland School of Medicine, Department of Emergency Medicine, Baltimore, Maryland |
Case outcome
Resident discussion
Final diagnosis
Key teaching points
ABSTRACT
A 50-year-old male presented to the emergency department with four days of intermittent chest pain and shortness of breath, which progressively worsened in severity. Testing revealed a troponin I greater than 100 times the upper limit of normal and an electrocardiogram with non-specific findings. This case takes the reader through the differential diagnosis and systematic work-up of the deadly causes of chest pain, ultimately leading to this patient’s diagnosis.
CASE OUTCOME
The diagnostic study of choice was CMR. The patient was found to have significant edema throughout the myocardium, with a focus over the anterolateral and inferior walls, seen on T2-weighted images.
While in the cardiac catheterization lab, the patient received an intra-aortic balloon pump (IABP) to support his cardiac perfusion. He was then admitted to the cardiac intensive care unit (CICU) and started empirically on broad-spectrum antibiotics. Serial echocardiograms showed an unchanging LVEF of 10–20% during his first week in the CICU. Further testing did not identify a specific infectious etiology. His LVEF improved to 20–25% on hospital day (HD) 8; the IABP was discontinued, and he was extubated successfully. CMR was then performed, demonstrating the edema described above and making the diagnosis. The remainder of his hospital course was complicated by a moderate retroperitoneal hematoma and dysphagia, both of which were managed medically and improved without further complication. His last echocardiogram before discharge on HD 19 showed an LVEF of 30–35%. He was discharged to a subacute rehabilitation center.
RESIDENT DISCUSSION
Myocarditis is an inflammatory disease involving the cardiac muscle. It affects 22 per 100,000 persons or around 1.5 million individuals worldwide, annually.12 The time course for the disease ranges from acute to chronic, with clinical severity depending on the degree of tissue damage, the underlying etiology, and patient comorbidities.
The most common infectious causes of myocarditis are viral, with over 20 different viruses implicated. Coxsackievirus was the most common up until the 1990s, but more recently parvovirus B-19 and human herpes virus 6 have become more common. Bacteria, fungi, protozoa, and even helminths have been identified as causes of myocarditis. Autoimmune disorders such as systemic lupus erythematosus, giant cell arteritis, and granulomatosis with polyangiitis can cause myocarditis as well. Less common, non-infectious etiologies include various cardiotoxins such as alcohol, cocaine, cyclophosphamide and heavy metals, and hypersensitivity reactions from antibiotics, clozapine, insect bites, and snake bites.13
Patients with acute myocarditis will often present with chest pain, dyspnea with or without exertion, unexplained sinus tachycardia, tachypnea, and signs of HF. Physicians evaluating patients with these complaints will often also consider ACS, PE, new-onset HF, or aortic dissection. Items in the patient’s history that are more supportive of myocarditis include a history of a recent mild illness, medication change, illicit drug use, or a lack of cardiovascular risk factors.13
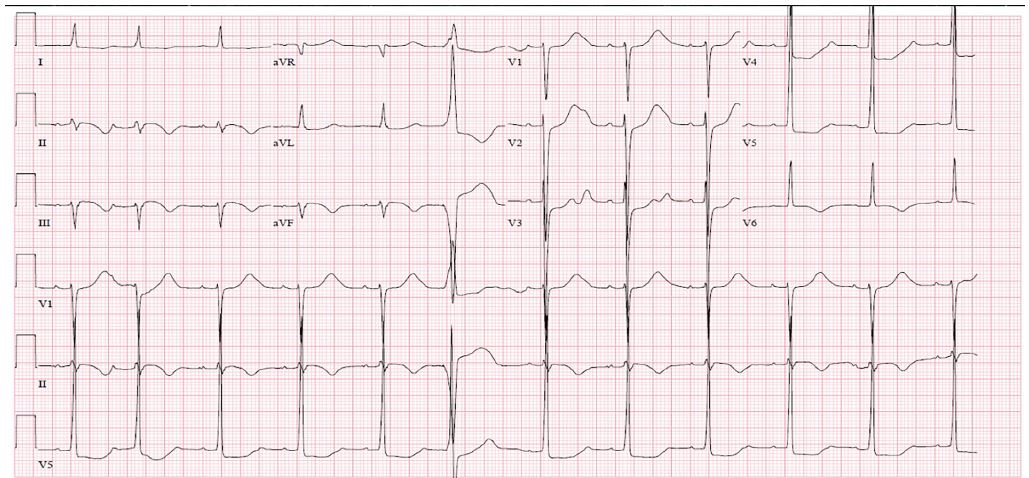
Initial testing should include an ECG, chest radiograph (CXR), cardiac biomarkers, and point-of-care cardiac ultrasound if available.9 ECG findings can vary dramatically, from sinus tachycardia to diffuse ST-segment elevation with PR-segment depression suggesting pericarditis. The CXR is helpful in identifying cardiomegaly, which is concerning if new, and may show evidence of pulmonary edema. Cardiac biomarkers can be markedly elevated, especially if the disease has involved all four chambers of the heart. Cardiac ultrasound can help confirm the presence of cardiomegaly as well as estimate the LVEF, identify wall motion abnormalities, and evaluate for other possible causes of the patient’s presentation.
CMR can be used to definitively identify myocardial inflammation and make the diagnosis if the patient is clinically stable and the resources are available.11 Endomyocardial biopsy is the classic method of diagnosing myocarditis, although it is rarely performed today. The affected tissue may be missed due to sampling error during the biopsy, and myocardial rupture and tamponade are rare but potentially life-threatening complications. Biopsy does have the advantage of being able to provide both a diagnosis and an etiology.
Management of acute myocarditis depends greatly on the patient’s presentation. Severe cases can present with cardiogenic shock secondary to acute HF and may require emergent intubation, ventilatory support and stabilization with the early administration of diuretics. Inotropic support with vasopressors, IABP, or extracorporeal circulatory membrane oxygenation (ECMO) can be used if the patient is hemodynamically unstable with evidence of shock.14 Targeted therapies range from appropriate antibiotics for infectious etiologies to intravenous immunoglobulin for autoimmune etiologies. The time-course of therapy depends on the patient’s clinical improvement.15 Serial echocardiograms are used both on an inpatient and outpatient basis to determine the patient’s response to therapies.
Prognosis varies with specific etiology and the severity at presentation. Otherwise healthy patients who develop acute myocarditis may return to baseline function if the initial disease process is identified and treated appropriately. Some patients develop chronic myocarditis or have severe enough disease to require cardiac transplantation.16
FINAL DIAGNOSIS
Acute myocarditis due to suspected viral or idiopathic etiology.
KEY TEACHING POINTS
A careful history and physical examination are crucial to suspecting mycarditis and initiating the appropriate diagnostics.
Myocarditis can be acute, subacute, or chronic.
Initial management is focused on controlling symptoms of HF; hypotensive patients may require inotropes and invasive support with IABP and/or ECMO.
Cardiac ultrasound is an invaluable tool to assess for the presence and severity of HF.
CMR is the diagnostic imaging study of choice.
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
Address for Correspondence: Laura J. Bontempo, MD, MEd, University of Maryland, Department of Emergency Medicine, 110 S. Paca Street, 6th Floor, Suite 200, Baltimore, MD 21201. Email: Lbontempo@som.umaryland.edu. 3:321 – 326
Submission history: Revision received September 23, 2019; Submitted October 14, 2019; Accepted October 15, 2019
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Rational Clinical Examination. 2019. Available at: https://jamanetwork.com/collections/6257/the-rational-clinical-examination. Accessed July 26, 2019.
2. Fanaroff AC, Rymer JA, Goldstein SA, et al. Does this patient with chest pain have acute coronary syndrome? The Rational Clinical Examination Systematic Review. JAMA. 2015;314(18):1955-65.
3. Castelli WP. Epidemiology of coronary heart disease: the Framingham study. Am J Med. 1984;76(2):4-12.
4. Han JH, Lindsell CJ, Storrow AB, et al. The role of cardiac risk factor burden in diagnosing acute coronary syndromes in the emergency department setting. Ann Emerg Med. 2007;49(2):145-52.
5. Panju AA, Hemmelgarn BR, Guyatt GH, et al. Is this patient having a myocardial infarction?. JAMA. 1998;280(14):1256-63.
6. Jaeschke R, Guyatt G, Lijmer J. Diagnostic tests. Users’ Guides to the Medical Literature 121–40. 2002.
7. Than M, Herbert M, Flaws D, et al. What is an acceptable risk of major adverse cardiac event in chest pain patients soon after discharge from the emergency department? A clinical survey. Int J Cardiol. 2013;166(3):752-4.
8. Nienaber CA, Eagle KA. Aortic dissection: new frontiers in diagnosis and management: Part I: from etiology to diagnostic strategies. Circulation. 2003;108(5):628-35.
9. Caforio AL, Pankuweit S, Arbustini E, et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2013;34(33):2636-48.
10. Fan Y, Chen M, Liu M, et al. Myocarditis with chest pain, normal heart function and extreme increased troponin. Int J Cardiol. 2016;209:307-9.
11. Friedrich MG, Sechtem U, Schulz-Menger J, et al. Cardiovascular magnetic resonance in myocarditis: A JACC White Paper. J Am Coll Cardiol. 2009;53(17):1475-87.
12. Richardson P, McKenna W, Bristow M, et al. Report of the 1995 World Health Organization/International Society and Federation of Cardiology Task Force on the Definition and Classification of Cardiomyopathies. Circulation. 1996;93(5):841-2.
13. Cooper LT. Myocarditis. N Engl J Med. 2009;360(15):1526-38.
14. Chen JM, Spanier TB, Gonzalez JJ, et al. Improved survival in patients with acute myocarditis using external pulsatile mechanical ventricular assistance. J Heart Lung Transplant. 1999;18(4):351-7.
15. Robinson JL, Hartling L, Crumley E, et al. A systematic review of intravenous gamma globulin for therapy of acute myocarditis. BMC Cardiovasc Disord. 2005;5:12.
16. O’Connell JB, Breen TJ, Hosenpud JD. Heart transplantation in dilated heart muscle disease and myocarditis. Eur Heart J. 1995;16:137-9.
TableLaboratory values of a 50-year-old male presenting with chest pain, shortness of breath, leg pain, and pre-syncope.
| Reference values | ||
|---|---|---|
| Complete blood cell count | ||
| White blood cellsen | 20.2 K/mcL | (3.4–9.6 K/mcL) |
| Hemoglobin | 13.2 g/dL | (13.2–16.6 g/dL) |
| Hematocrit | 38.3% | (38.3–48.6%) |
| Platelets | 239 K/mcL | (135–317 K/mcL) |
| Serum chemistries | ||
| Sodium | 139 mmol/L | (136–145 mmol/L) |
| Potassium | 3.6 mmol/L | (3.5–5.0 mmol/L) |
| Chloride | 97 mmol/L | (95–105 mmol/L) |
| Bicarbonate | 29 mmol/L | (22–28 mmol/L) |
| Blood urea nitrogen | 20 mg/dL | (7–18 mg/dL) |
| Creatinine | 1.59 mg/dL | (0.6–1.2 mg/dL) |
| Magnesium | 1.5 mmol/L | (1.5–2.0 mmol/L) |
| Total protein | 7.1 g/dL | (6.0–7.8 g/dL) |
| Albumin | 3.9 g/dL | (3.5–5.5 g/dL) |
| Total bilirubin | 0.7 mg/dL | (0.1–1.0 mg/dL) |
| Aspartate aminotransferase | 1579 u/L | (8–20 u/L) |
| Alanine aminotransferase | 157 u/L | (8–20 u/L) |
| Alkaline phosphatase | 88 u/L | (20–70 u/L) |
| Additional Labs | ||
| Troponin I | 697.0 ng/mL | (<0.034 ng/mL) |
| Lactate | 3.9 mEq/L | (0.3–2.3 mEq/L) |
| C-reactive protein | 6.6 mg/L | (0.0–3.0 mg/L) |
| Erythrocyte sedimentation rate | 55 mm/hr | (0.0–22 mm/hr) |
K/mcL, thousands per microliter; mg, milligrams; dL, deciliter; g, gram; mmol, millimoles; L, liter; u, units; ng, nanogram; mL, milliliter; mEq, milliequivalents; mm, millimeter; hr, hour.