
| Author | Affiliation |
|---|---|
| Jason David, MD | Nellis Air Force Base, Mike O’Callaghan Military Medical Center, Department of Emergency Medicine, Las Vegas, Nevada |
| Jerad Eldred, MD | University of Nevada, Las Vegas, University Medical Center of Southern Nevada, Department of Emergency Medicine, Las Vegas, Nevada |
| David Raper, DDS | Nellis Air Force Base, Mike O’Callaghan Military Medical Center, Department of Emergency Medicine, Las Vegas, Nevada |
ABSTRACT
Case Presentation
A four-year-old female patient presented to the emergency department with an epinephrine auto-injector that had unintentionally discharged into her mandible. There was difficulty removing the auto-injector at bedside. Images we acquired noted needle curvature not present in an off-the-shelf model. She was sedated, and the auto-injector was removed by retracing the angle of discharge, with care taken not to inject epinephrine into the patient.
Discussion
Epinephrine auto-injector accidental discharges are an unusual injury pattern, but the incidence of such events is increasing in the United States. The emergency clinician should be cognizant of complicating factors with discharges, such as bent needles. Here we discuss a case of discharge into the maxillofacial region (lower jaw), with approaches to treatment.
CASE PRESENTATION
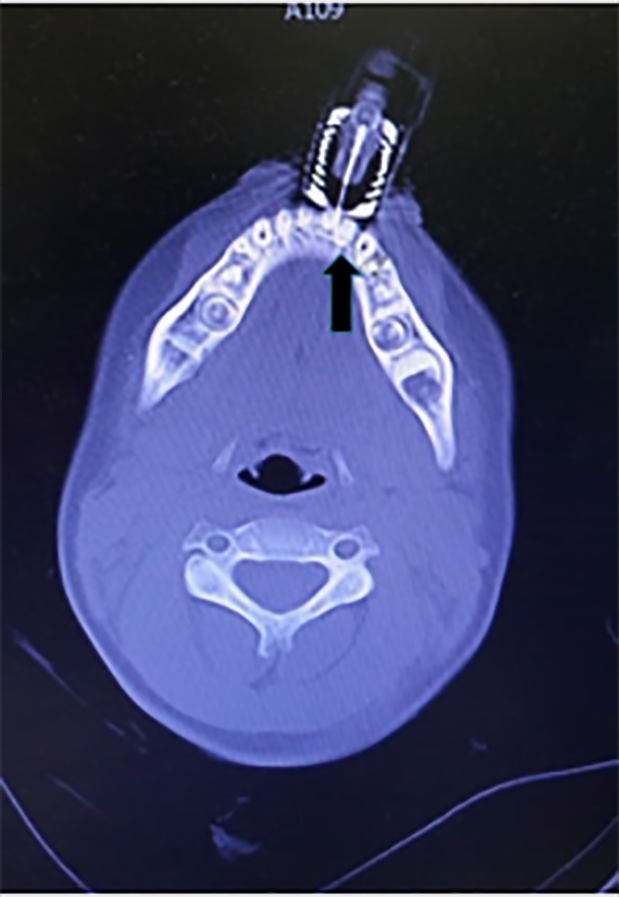
A four-year-old female presented to the emergency department (ED) with an epinephrine auto-injector unintentionally injected and lodged in her lower jaw that entered through the gingiva. Radiographs of the skull and computed tomography (CT) revealed a hooked epinephrine auto-injector embedded between the lower central incisors beneath the gingival line, bent at an approximately 140° angle (Images 1 and 2).

An initial attempt was made by the parents to remove the object at home followed by an attempt at ED bedside, which proved to be difficult due to needle angulation. We consulted oral-maxillofacial surgery; the patient was sedated with intravenous ketamine, and under sedation the hook was pulled in a retrograde manner following the noted posterior-lateral trajectory of the bent needle tip on maxillofacial imaging (Image 3). With some force, the needle was removed with care that it not accidentally discharge epinephrine into the patient. There was a very minor avulsion of gingival mucosa, which we learned did not interfere with patient’s oral intake or speech after following up with parent.

{kind=link}
DISCUSSION
Unintentional epinephrine auto-injector injuries typically occur in the digits or the legs.1 These cases are on the rise, as epinephrine auto-injectors have become more commonly prescribed.2 However, exploring the world by placing objects in their mouths is a normal stage of early childhood development.3 This case was particularly concerning due to the initial difficulty in removing the auto-injector and fear of accidentally discharging the adult-dose epinephrine into the patient. Efforts were made to stabilize the auto-injector with a bulky dressing and pillow. Due to the difficulty with initial removal, imaging was pursued. Maxillofacial CT is the optimal imaging study.4
CPC-EM Capsule
What do we already know about this clinical entity?
Epinephrine auto-injector accidental discharges are a unique and rising injury pattern in the United States and can have deceivingly simple presentations.
What is the major impact of the image(s)?
Emergency medicine physicians should be aware of complicating factors with accidental auto-injector injuries, such as bent needles, and appreciate nuances to treatment.
How might this improve emergency medicine practice?
Emergency medicine physicians will be more familiar with this particular injury pattern and be more effective at treating similar auto-injector injuries.
The mechanism behind the hooking of the needle of the auto-injector could presumably be due to hitting the subgingival areas of the incisor and curving, as well as bending, during attempted removals. Postulations from similar case studies regarding the curvature of auto-injector needles include bending when hitting a bone during injection, bending when the patient moves during injection, or if the needle fires off center and hits the cartridge carrier, hooking the needle prior to injection.5 This situation should be anticipated and investigated with imaging by the treating physician before attempting to remove the needle blindly. Stabilizing the auto-injector with a pillow and bulky dressing will also prevent further bending of the needle, which would make removal more difficult. Furthermore, care should be taken not to accidentally discharge the epinephrine dose, either by securing the pen with a bulky dressing as we did, or by removing the chamber (which we found to be extremely difficult). Prudent emergency physicians should keep these factors (object stabilization, needle curvature, and remaining epinephrine dose) in mind when treating a victim of accidental auto-injector discharge to a sensitive area such as the face.
Footnotes
Section Editor: Anna McFarlin, MD
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
The authors attest that their institution requires neither Institutional Review Board approval nor patient consent for publication of this case report. Documentation on file.
Address for Correspondence: Jason David, MD, Mike O Callaghan Military Medical Center, 4700 Las Vegas Blvd N Nellis AFB, 89191 Email: Jason.w.david.mil@mail.mil. 6:93 – 95
Submission history: Revision received August 20, 2021; Submitted October 29, 2021; Accepted November 10, 2021
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none. The views expressed here are those of the authors and do not reflect the official policy of the Department of the Army, the Department of Defense, or the U.S. Government.
REFERENCES
1. Anshien M, Rose SR, Wills BK. Unintentional epinephrine auto-injector injuries: A National Poison Center observational study. Am J Ther. 2019;26(1):e110-e4.
2. Campbell RL, Manivannan V, Hartz M, et al. Epinephrine auto-injector pandemic. Pediatric Emerg Care. 2021;28(9):938-42.
3. Koch G, Poulsen S. Paediatric dentistry—a clinical approach. Mental Development of the Child. 2001;35:41.
4. Javadrashid R, Fouladi DF, Golamian M, et al. Visibility of different foreign bodies in the maxillofacial region using plain radiography, CT, MRI and ultrasonography: an in vitro study. Dentomaxillofac Radiol. 2015;44(4):20140229.
5. Goldman RD, Long KC, Brown JC. Hooked epinephrine auto-injector devices in children: four case reports with three different proposed mechanisms. Allergy Asthma Clin Immunol. 2020;16:19.