
{kind=link}
| Author | Affiliation |
|---|---|
| Erik Wright, MD | University of Illinois College of Medicine Peoria, OSF Saint Francis Medical Center, Department of Emergency Medicine, Peoria, Illinois |
| John W. Hafner, MD, MPH | University of Illinois College of Medicine Peoria, Department of Emergency Medicine, Peoria, Illinois |
| Gregory Podolej, MD | University of Illinois College of Medicine Peoria, Department of Emergency Medicine, Peoria, Illinois |
| Douglas L. Feinstein, PhD | University of Illinois Chicago, Jesse Brown VA Medical Center, Department of Anesthesiology, Chicago, Illinois |
| Richard van Breemen, PhD | Oregon State University, Linus Pauling Institute, Department of Pharmaceutical Sciences, Corvallis, Oregon |
| Israel Rubinstein, MD | University of Illinois Chicago, Jesse Brown VA Medical Center, Division of Pulmonary, Critical Care, Sleep, and Allergy Medicine, Chicago, Illinois |
| Steven Aks, DO | Rush University, Department of Emergency Medicine, Chicago, Illinois |
| Michael Wahl, MD | John H. Stroger Hospital of Cook County, Department of Emergency Medicine, Chicago, Illinois |
Introduction
Methods
Results
Discussion
Limitations
Conclusion
ABSTRACT
Introduction
Synthetic cannabinoids are a rapidly expanding subset of designer drugs widely available in the United States since 2008. In Illinois during the spring of 2018, over 160 documented cases of bleeding and prolonged coagulopathy occurred secondary to contaminated synthetic cannabinoids.
Methods
We conducted a retrospective cohort study consisting of 38 patients to describe the initial emergency department (ED) presentation, diagnosis, and treatment.
Results
Through serum testing we found that three long-acting anticoagulant rodenticides (LAAR) were detected in patients who had inhaled these tainted products: brodifacoum, difenacoum, and bromodialone.
Discussion
This study encompasses the largest ED presentation of LAAR poisoning via the inhalational route known to date.
Conclusion
The emergency physician should be aware of the potential for tainted coingestants as the cause of undifferentiated coagulopathy.
INTRODUCTION
Synthetic cannabinoids have become a widely used type of designer drug in the global drug market.1 Synthetic cannabinoids first made their appearance in the United States in 2008 and are sold under numerous names including “K2,” “Spice,” and “Black Magic.” These drugs have long evaded law enforcement due to the drug manufacturers’ ability to quickly alter chemical formulas and generate novel products that have yet to be made illegal under the Controlled Substances Act. In addition, most of these are packaged and sold as herbal products and labeled as “not for human consumption” to further circumvent drug laws.2
After being dissolved in solvent, synthetic cannabinoids are typically formulated and sprayed onto an herbal product that is then smoked and inhaled.3 A wide array of symptoms has been associated with ingestion from these compounds. While some users report similar euphoric effects to that of marijuana, there have been other significant adverse reactions reported. Most common adverse symptoms reported include paranoid delusions, psychosis, supraventricular tachycardia, seizures, and altered sensorium.4 Additionally, there are many reports describing associations of synthetic cannabinoids with acute medical conditions including ischemic and hemorrhagic strokes, thrombotic microangiopathy, disseminated intravascular coagulation, immune thrombocytopenic purpura, rhabdomyolysis, and death.5-9
Illicit drugs are often adulterated with other products to increase profits and/or to enhance or alter the drugs’ effects on the body. Several substances including both legal and illegal compounds have been used to achieve these effects.10 Interestingly, there are numerous case reports surrounding the use of warfarin as an adulterant “lacing compound.”11-15 The addition of warfarin or long-acting anticoagulant rodenticides (LAAR) may alter CYP P450 metabolism of the psychoactive compound and act to enhance the high. We surmise drug manufacturers and distributors have exploited this pharmacological interaction in the past based on several other reported cases.
During the spring of 2018, a large influx of patients presented to area hospitals in Illinois with unfounded coagulopathy and bleeding. The outbreak began in mid-March 2018 with over 160 reported cases in Illinois across 15 counties through June 2018.16 Through July 2018 the number of cases increased to 255 with eight reported deaths.17 By the end of July, over 55% of the documented cases had occurred in Peoria, Tazewell, and surrounding counties in Illinois. Due to symptoms of significant, prolonged bleeding and lack of known exposure to vitamin K1 antagonists there was concern that these patients had been inadvertently exposed to a long-acting anticoagulant. A large, interdisciplinary task force composed of members of the US Centers for Disease Control and Prevention, Illinois Poison Center, Illinois Department of Public Health, law enforcement agencies, and health departments was convened to elucidate the cause of this unexplained coagulopathy. It was promptly discovered that poisoned patients had been exposed to tainted synthetic cannabinoids that largely tested positive for brodifacoum, a LAAR.18
Other researchers have described a similar population at a single Illinois academic center.19,20 While those studies concentrated on the inpatient population, treatment and long-term therapy, our focus is to address the emergency department (ED) presentation, diagnosis, and treatment. While the populations are similar, we feel the difference in focus is substantive as the emergency physician is tasked with diagnosis, stabilization, and treatment initiation prior to the patient’s hospital stay. Our goal is to help readers recognize and diagnose patients suffering from bleeding diathesis in the ED as well as to identify potential resuscitative treatment strategies via descriptive data from a recent LAAR outbreak.
Population Health Research Capsule
What do we already know about this issue?
An outbreak of bleeding diathesis in Illinois in spring 2018 was linked to exposure to synthetic cannabinoids contaminated with long-acting anticoagulant rodenticides.
What was the research question?
To elucidate management therapies we investigated patients who presented to our ED with concerns for exposure to anticoagulants.
What was the major finding of the study?
Many of our patients required active reversal of anticoagulant effects with Vitamin K and/or fresh frozen plasma, and a high number were admitted to the intensive care unit.
How does this improve population health?
The emergency physician must be prepared for and aware of the possibility of future outbreak linked to tainted synthetic cannabinoids.
METHODS
Study Design
We conducted a retrospective cohort study to describe the initial ED presentation, diagnosis, and treatment of inhaled LAAR-induced coagulopathy.
Population
This study was conducted at two Illinois academic urban EDs with annual patient visits of approximately 85,000 and 120,000, respectively. We performed chart review of all patients with suspected brodifacoum-related coagulopathy from contaminated synthetic cannabinoids presenting to the ED. Patients with reported exposure who presented to either of these ED between March 29–April 23, 2018 were included in this study. Patients were identified from internal and public health registries, from patients themselves self-identifying as having an exposure, or who were identified by hospital providers as having an exposure. Using defined variables, we abstracted ED and hospital charts, and all data was deidentified prior to analysis. The institutional review boards (IRB) of the University of Illinois College of Medicine at Peoria and Oregon State University reviewed and approved this study prior to initiation. All data remained deidentified throughout.
Samples
Serum samples were obtained from 38 patients from Illinois academic urban EDs. Initial blood samples were obtained for clinical care of these patients. Leftover serum from clinical draws was then placed in vacutainers and stored at −80°C until analysis. Samples were sent to and analyzed at the Linus Pauling Institute, Corvallis, OR. Ultra performance liquid chromatography – tandem mass spectrometry (UHPLC-MS/MS) analysis was used to quantify plasma concentrations of brodifacoum, difenacoum and bromadiolone, three structurally distinct LAARs.
Statistics
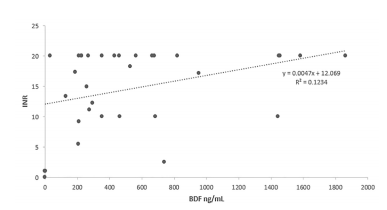
We used descriptive statistics to describe the population, define common symptomatology, and identify successful treatment regimens. Unadjusted linear regression analysis was used to describe relationships between plasma LAAR levels and international normalized ratio (INR) values. We used Pearson coefficients to investigate the correlation between variables.
RESULTS
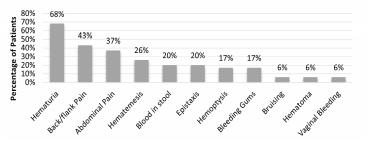
A total of 38 patients met criteria for inclusion in this study. Of the patients included, 24 males (68%) and 14 females (36%) were identified as being exposed to tainted synthetic cannabinoids. Ages ranged between 23–65 years with a mean age of 37 years at time of presentation. Of these patients, 76% (n = 24) were identified as White. This cohort experienced high admission rates to the hospital with 92% of patients (n = 35) being admitted. The three patients not admitted to the hospital left the ED against medical advice (AMA). Mean length of stay for those admitted was 4.1 days, with a range of 1–11 days. Readmission rates were also very high for this group as 30% of patients (n = 12) were readmitted within 30 days of their initial presentation. Among the wide variety of presenting symptoms the most common presenting complaint was back and or flank pain and the most common site of bleeding was from the urinary tract (
On average, patients had significantly elevated INR values at time of presentation. The INRs ranged from 1 to >20. (The maximum upper limit of on-site laboratory testing is an INR level of >20.) The mean INR at presentation was 14.5. At time of discharge from the hospital, the mean INR was 2.5.
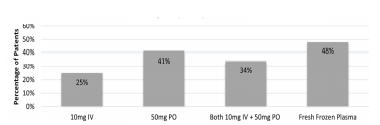
Reversal of LAAR-related coagulopathy was at the treating physician’s discretion. Several therapeutic decisions were made in consultation with Illinois Poison Control. Patients were treated with a combination of oral vitamin K1, intravenous (IV) vitamin K1, and fresh frozen plasma (FFP). Two patients left AMA before being treated. Of those treated, 25% (n = 9) received 10 milligrams (mg) IV vitamin K1; 41% (n = 16) received 50 mg oral vitamin K1 as monotherapy, and 34% (n = 13) received a combination of 50 mg oral vitamin K1 and 10 mg IV vitamin K1. In addition to vitamin K1, 48% of patients (n = 18) also received FFP with a dose range of 1–4 units while in the ED (
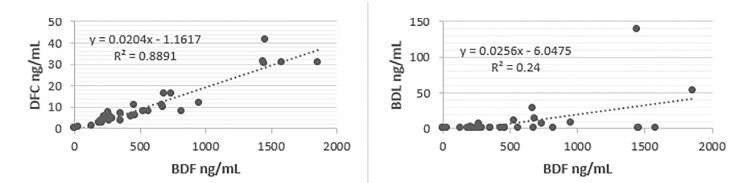
Levels of LAAR and serum INR correlated in a weakly linear fashion (
DISCUSSION
In the largest cohort of inhalational LAAR coagulopathy to date, many of the patients were quickly recognized and triaged in the ED. The initial treatments in the ED focused on recognition and stabilization as well as reversal of their coagulopathy. The most prominent presenting symptoms included complaints of back and/or flank pain and abdominal pain. Physical manifestations of coagulopathy, including hematuria, bloody stools, and epistaxis and mucosal bleeding, were also observed. Although the exact reasons for combining, or tainting, synthetic cannabis with LAAR is unknown, it is hypothesized that potentiation of cannabinoid effects may have been the desired outcome.22-25 Regardless of intent, recognizing the potential of contamination of street drugs is extremely salient to the emergency physician. Since the Illinois outbreak that occurred between March-May 2018, there have been further outbreaks of tainted synthetic cannabinoid coagulopathy throughout the East Coast.26 As this would suggest, the outbreak in Illinois does not appear to be an isolated incident, and continued vigilance and awareness of this ongoing problem by emergency care providers is necessary.
This cohort of patients was largely treated with vitamin K1 in both oral and IV formulations while in the ED. Early involvement of Illinois Poison Control allowed for additional treatment recommendations and appropriate surveillance of the outbreak. Most patients were given either 50 mg oral vitamin K1 and/or 10 mg IV vitamin K1. However, in those with more significant bleeding, FFP in doses between 1 to 4 units was also used. More advanced products such as Kcentra and factor eight inhibitor bypassing activity (FEIBA) were not used. These products have been shown in several studies to rapidly reverse LAAR-induced coagulopathy and are recommended for those with life-threatening bleeding.27-28
Treatment for LAAR-induced coagulopathy outside the initial ED stay has proven to be difficult. Many of these patients have experienced repeat ED visits with 30% readmitted in the first 30 days. Many patients were sent home with high doses of oral vitamin K1, ranging from 50–150 mg daily. With 15 mg of generic vitamin K1 estimated to cost around 80 US dollars, this treatment was often cost-prohibitive for many patients. We suspect cost was the reason many patients with coagulopathy went untreated and suffered from recurrent bleeding, comorbidities, and repeat hospitalizations. Additionally, the pharmacokinetics of brodifacoum (which has a half-life up to 40 hours) can cause patients to suffer from coagulopathy for up to 12 months post ingestion. Until this time, many experts recommended using serum INR to guide vitamin K1 therapy for patients with ingestions. With data from these outbreaks, new proposals suggest that following LAAR levels may be the best way to determine when vitamin K1 therapy may be stopped.29,30
LIMITATIONS
This descriptive study of the largest inhalational LAAR poisoning to date is not without limitations. First is that we conducted a retrospective chart review of patient data. While this study is limited by the standard biases that retrospective chart reviews suffer, we have addressed some of these aspects. During this outbreak, IRB approval was obtained to allow for a prospective approach to standard documentation; this limited some of the collection discrepancies. In addition, prior to chart review we created a standardized abstraction form allowing for a systematic approach to data retrieval. Secondly, while this is the largest tainted inhalational LAAR cohort to date, inherently the patient population is limited. Although we were able to formulate some correlations given the sample size, results may be more pronounced with a larger cohort.
This is the largest cohort of inhalational LAAR toxicity known to date. Recurrences of smaller outbreaks would suggest that LAAR-contaminated synthetic cannabinoids may not be isolated to synthetic cannabinoids.
CONCLUSION
Working on the frontlines of healthcare, the emergency physician should be aware of the potential for tainted coingestants as the cause of undifferentiated coagulopathy. Long-acting anticoagulant rodenticide poisoning can usually be treated with vitamin K1, with the majority of these patients needing long-term outpatient treatment. For those with life-threatening bleeding more advanced products including fresh frozen plasma, Kcentra and FEIBA may be indicated. Additionally, the emergency physician should be aware of the high potential for return visits in these patients for recurrent bouts of coagulopathy due to the prolonged course of action of the drug.
Footnotes
Section Editor: Brandon Wills, DO, MS
Full text available through open access at
Address for Correspondence: Erik Wright, MD, University of Illinois College of Medicine Peoria/OSF Saint Francis Medical Center, Department of Emergency Medicine, 530 NE Glen Oak Avenue, Peoria, Illinois 61637. Email: erik.h.wright@osfhealthcare.org. 7 / 2021; 22:1014 – 1019
Submission history: Revision received December 29, 2019; Submitted February 17, 2021; Accepted February 24, 2021
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. No author has professional or financial relationships with any companies that are relevant to this study. There are no conflicts of interest or sources of funding to declare.
REFERENCES
1. Albertson T. Recreational drugs of abuse. Clinic Rev Allerg Immunol. 2014;46(1):1-2.
2. Davis GG. Drug abuse: Newly emerging drugs and trends. Clin Lab Med. 2012;32(3):407-14.
3. Karila L, Benyamina A, Blecha L, et al. The synthetic cannabinoids phenomenon. Curr Pharm Des. 2016;22(42):6420-5.
4. Jerry J, Collins G, Streem D. Synthetic legal intoxicating drugs: the emerging ‘incense’ and ‘bath salt’ phenomenon. Cleve Clin J Med. 2012;79(4):258-64.
5. Bernson-Leung M, Leung L, Kumar S. Synthetic cannabis and acute ischemic stroke. J Stroke Cerebrovasc Dis. 2014;23(5):1239-41.
6. Khanagavi J, Phatak P, Kolte D, Aronow WS, Lanier G. Synthetic cannabinoids-induced thrombotic microangiopathy leading to acute heart failure. Circulation. 2013;128(22).
7. Nocerino A, Ilyas N. Unusual toxicities of synthetic marijuana. J Gen Intern Med. 2016;31(2):S776.
8. Ozturk E, Oral A, Ozdemir M, et al. Synthetic marijuana “K2” induced ITP. Platelets. 2015;26(3):258-9.
9. Sherpa D, Paudel BM, Subedi BH, et al. Synthetic cannabinoids: the multi-organ failure and metabolic derangements associated with getting high. J Community Hosp Intern Med Perspect. 2015;5(4):27540.
10. Solimini R, Rotolo MC, Pellegrini M, et al. Adulteration practices of psychoactive illicit drugs: an updated review. Curr Pharm Biotechnol. 2017;18(7):524-30.
11. La Rosa FG, Clarke SH, Lefkowitz JB. Brodifacoum intoxication with marijuana smoking. Arch Pathol Lab Med. 1997;121(1):67-9.
12. Waien SA, Hayes D, Leonardo JM. Severe coagulopathy as a consequence of smoking crack cocaine laced with rodenticide. N Engl J Med. 2001;345(9):700-1.
13. Tecimer C, Yam LT. Surreptitious superwarfarin poisoning with brodifacoum. South Med J. 1997;90(10):1053-5.
14. Damkier P, Lassen D, Christensen MMH, Madsen KG, Hellfritzsch M, Pottegard A. Interaction between warfarin and cannabis. Basic Clin Pharmacol Toxicol. 2019;124(1):28-31.
15. Kim JH, Kim HS, Kong TY, et al. In vitro metabolism of a novel synthetic cannabinoid, EAM-2201, in human liver microsomes and human recombinant cytochrome P450s. J Pharm Biomed Anal. 2016;119:50-8.
16. More synthetic cannabinoids cases. 2018. Available at: http://dph.illinois.gov/news/more-synthetic-cannabinoids-cases. Accessed September 28, 2018.
17. Connors JM. Hemorrhagic highs from synthetic cannabinoids— a new epidemic. N Engl J Med. 2018;379(13):1275-7.
18. Moritz E, Austin C, Wahl M, et al. Notes from the field: outbreak of severe illness linked to the vitamin K antagonist brodifacoum and use of synthetic cannabinoids — Illinois, March–April 2018. MMWR Morb Mortal Wkly Rep. 2018;67(21):607-8.
19. Kelkar AH, Smith NA, Martial A, et al. An outbreak of synthetic cannabinoid-associated coagulopathy in Illinois. N Engl J Med. 2018;379(13):1216-23.
20. Devgun JM, Rasin A, Kim T, et al. An outbreak of severe coagulopathy from synthetic cannabinoids tainted with long-acting anticoagulant rodenticides. Clin Toxicol (Phila). 2019:1-8.
21. Bruno GR, Howland MA, McMeeking A, et al. Long-acting anticoagulant overdose: brodifacoum kinetics and optimal vitamin K dosing. Ann Emerg Med. 2000;36(3):262-7.
22. Damkier P, Lassen D, Christensen MMH, et al. Interaction between warfarin and cannabis. Basic Clin Pharmacol Toxicol. 2019;124(1):28-31.
23. Yamreudeewong W, Wong HK, Brausch LM, et al. Probable interaction between warfarin and marijuana smoking. Ann Pharmacother. 2009;43(7):1347-53.
24. Waien SA, Hayes D, Leonardo JM. Severe coagulopathy as a consequence of smoking crack cocaine laced with rodenticide. N Engl J Med. 2001;345(9):700-1.
25. La Rosa FG, Clarke SH, Lefkowitz JB. Brodifacoum intoxication with marijuana smoking. Arch Pathol Lab Med. 1997;121(1):67-9.
26. Health alert network (HAN) advisory released on May 25, 2018: Outbreak of life-threatening coagulopathy associated with synthetic cannabinoids use. ;379(13):1216-23. Available at: https://Emergency.cdc.gov/han/han00410.asp.
27. Kearon C, Akl EA, Ornelas J, et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest. 2016;149(2):315-52.
28. Doyle RJ, Elfessi Z, Kolman K. Fixed dose 4-factor prothrombin complex concentrate for bleeding caused by long acting anticoagulant rodenticides. Am J Emerg Med. 2018;36(10):1922.e3-1922.e4.
29. Feinstein DL, Nosal DG, Swetha R, et al. Effects of vitamin K1 treatment on plasma concentrations of long-acting anticoagulant rodenticide enantiomers following inhalation of contaminated synthetic cannabinoids. Clin Toxicol (Phila). 2020;58(7):716-24.
30. Rubinstein I, Weinberg G, van Breemen R, et al. Treatment for long acting anticoagulant rodenticide poisoning – beyond INR monitoring?. Toxicol Commun. 2018;2(1):59-61.