
{kind=link}
| Author | Affiliation |
|---|---|
| Sosamma Methratta, MD | Penn State Milton S. Hershey Medical Center, Department of Radiology, Hershey, PA |
| Arabinda K. Choudhary, MD | Penn State Milton S. Hershey Medical Center, Department of Radiology, Hershey, PA |
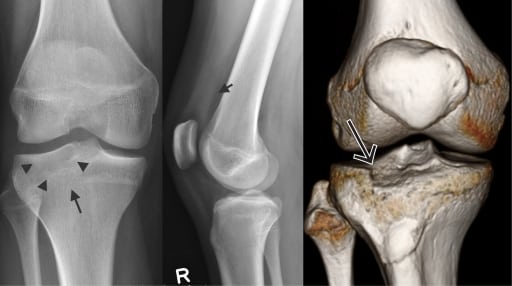
A 14-year-old boy developed immediate right knee pain and difficulty weight bearing after colliding with another baseball player. Knee radiographs and computed tomography knee confirmed type-3A Schatzker tibial plateau fracture. A depressed fracture may not be appreciated on plain radiographs and only clearly demonstrated at cross sectional imaging. Studies of tibial plateau fractures have shown that surgical plan based on radiographs are modified in 6–60% of cases after CT.1Furthermore, this fracture is more common in older age group with osteopenia rather than young patients. If left untreated, depression results in joint incongruity, valgus deformity and a sense of instability.1
We describe three signs of type 3A Schatzker fracture of lateral tibial plateau on radiographs, which include loss of visualization of the tibial plateau margin, associated increased sclerosis and effusion (Figure). In the setting of traumatic knee effusion, anterior and posterior margins of the tibial plateaus should be scrutinized. Management of the fracture centers on evaluating and repairing the articular cartilage and restoring the articular surface.1,2 The patient underwent open reduction and internal fixation with elevation of the depressed fracture fragment and supported by allograft. Optimum outcome post treatment is obtained with an anatomic reduction, adequate rigid internal fixation and bone grafting of the depressed areas.2
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted February 3, 2010; Revision Received March 14, 2010; Accepted March 22, 2010
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Arabinda K. Choudhary, MD, Department of Radiology, Penn State Hershey Medical Center, 500 University Dr., Hershey, PA 17033
Email: achoudhary@hmc.psu.edu
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Markhardt BK, Gross J, et al. Schatzker Classification of Tibial Plateau Fractures: Use of CT and MR Imaging Improves Assessment. Radiographics. 2009;29:585–597. [PubMed]
2. Lachiewicz PF, Funcik T. Factors influencing the results of open reduction and internal fixation of tibial plateau fractures. Clin Orthop Relat Res. 1990;259:210–5. [PubMed]