
{kind=link}
| Author | Affiliation |
|---|---|
| Chris Merritt, MD, MPH, MHPE | Alpert Medical School of Brown University, Department of Emergency Medicine, Providence, Rhode Island |
| Sally A. Santen, MD, PhD | Virginia Commonwealth University School of Medicine, Department of Emergency Medicine, Richmond, Virginia; University of Cincinnati, Departments of Emergency Medicine and Medical Education, Cincinnati, Ohio |
| Stephen John Cico, MD, Med | Indiana University School of Medicine, Department of Emergency Medicine, Indianapolis, Indiana |
| Margaret Wolff, MD, MHPE | University of Michigan Medical School, Department of Emergency Medicine, Ann Arbor, Michigan |
| Martin Pusic, MD, MA, PhD | Harvard Medical School, Department of Emergency Medicine, Boston, Massachusetts |
Learning is critical to developing and maintaining competence. Learning is slow at the beginning, accelerates rapidly as we gain skills and knowledge, and then slows again as we achieve competence and approach expertise. Rapid periods of expansion of ability and understanding alternate with stages of relative inertia. We may at times focus on routinization, the repetitive effort by which we standardize aspects of our practice, producing a steady practice state that is efficient and systematic. At other times, however, patients and systems demand a more dynamic approach to learning.
This notion of dynamic expertise requires emergency medicine (EM) practitioners to continually adapt; the very nature of EM requires it. If a practitioner does not exert at least some adaptive effort in response to pressures, expertise erodes and, in extreme situations, a competency threshold may be breached.1 In practice, maintenance of competency looks similar to evolution – periods of static equilibrium where little adaptive energy is required punctuated by intense periods of exploration or expansion of skills. At no time has this become more evident than during the COVID-19 pandemic.
COVID-19 has disrupted our equilibrium, dictating rapid evolutionary advances in our EM knowledge and skills. The fault lines in our expertise have been laid bare and our individual and organizational adaptability tested to the point of near breaking.2-5 Systems and individuals alike have had to flex their adaptive expertise in the face of this strain. Emergency physicians rapidly developed new methods of patient assessment, intubation, ventilation, and critical care to name but a few.6-9 There has been rapid dissemination of innovation, with the worldwide medical community quickly sharing, learning, and adapting to address the crisis on the patient and system levels.10 We have developed, out of necessity, a type of expertise in which the EM expert is newly facile with innovation, flexibility, and adaptability.11-13
Emergency physicians know intuitively that one size does not fit all. Every day brings novelty and complexity. COVID-19 taught us new lessons in adaptive expertise, yet as EM educators we may not think intentionally about training our learners and ourselves in becoming adaptive experts able to maintain competence in the face of disruptive pressures.
To promote the type of adaptive expertise that allows emergency physicians to be innovators and lifelong learners, it is important to teach not just EM facts, skills, and procedures. We also need to provide our EM learners with the mindset and ability to be adaptive.14 In other words, our learners should be encouraged to develop “the ability to learn new information, make effective use of resources, and invent new procedures in order to support learning and problem solving in practice.”15 The adaptive lens emphasizes learning that occurs with awareness of the complexity of context, and encourages learners to become aware of new features as well as recognizing old features (Table 1).16
Table 1A comparison of traditional teaching methodology with teaching for adaptive expertise. Teaching for adaptive expertise may not replace more traditional teaching methods in all cases but ought to be built into emergency medicine training early and often.
| Parameter | Traditional method | Teaching for adaptive expertise |
|---|---|---|
| Emphasis | Efficient learning of well-known illness scripts and prototypic examples | Developing expertise that can match any variation or situation that is presented |
| Unit of Adaptation | Environment is adapted to the learner | Learner learns to adapt to the environment |
| Learning support | Allowing learners to gain full confidence within their comfort zones | Give learners approaches for adapting outside their comfort zones |
| Progression | Progressive withdrawal of learning supports as learners near competence | Progressive addition of adaptive behaviors |
| Endpoint | Full withdrawal of learning supports at competence. | No endpoint – coaching long-term for continued improvement, innovation, and adaptation |
A number of learning conditions or contexts facilitate a trainee’s preparation for adaptation. Many of these will be familiar to the emergency physician (Table 2). For example, learning from a wide range of examples allows for the recognition that although illness scripts may represent the typical case of a given condition, no illness or condition is without variability. “If you’ve seen one case, you’ve seen one case” often rings true. By experiencing not just repetition but varied repetition, the adaptive clinician learns how to deal with not just rare cases but also the “not-yet-encountered” variants. The learner understands to trust their instinct, but to be aware of atypical presentations or complexities of illness that require new or adapted approaches to diagnosis or treatment. As faculty we can ask the learners to identify the uniqueness of each patient case and to approach care with flexibility and inquiry.
Table 2Conditions that optimize learning for adaptive expertise.
| Conditions for learning adaptive expertise: | Examples: |
|---|---|
| Learning from a wide range of examples | Exposure to a variety of patient and illness presentations, varying in context and severity, repeated over time |
| Challenging learners to develop new approaches | Encouraging learners to identify gaps in their understanding and to step beyond their comfort zones, intentionally building, testing, and applying new approaches to even familiar conditions17 |
| Encourage deep mechanistic understanding | Returning to first principles when considering how and why a condition may present in varied fashion. Asking “What if…?” and “Why?” when faced with routine problems. |
| Learning through repeated opportunity for application of both routinization and innovation | Alternately seeking to improve efficiency, apply innovation, and attend to the balance between them. “Is this the wheezing patient that requires a bespoke solution?” |
Further, as we train residents we have a tendency to scaffold their learning, risking keeping them in their comfort zone. To develop adaptive expertise, it can be helpful to pull residents outside their comfort zone, challenging them to develop new approaches to situations. Through this process they develop flexibility to match whatever a situation presents.
Another method of optimizing for adaptation is to encourage a deep mechanistic understanding of illness to be able to approach new patient presentations. Through this deep understanding the learner may step beyond usual recipes to innovate new approaches. In patients with COVID-19, application of routine ventilation strategies was quickly shown to be inadequate. A mechanistic understanding of pulmonary function allows recognition of potential optimal ventilation strategies and patient positioning when confronted with the striking differences required in COVID-19 management.
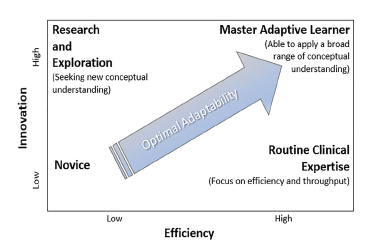
Finally, to recognize how to balance adaptation and efficiency, learning must contain opportunities for application of each. It does little good to emphasize efficiency only in routine cases or to emphasize innovation only in unusually complex scenarios. As residents focus on patient volume and flow, they may lose their deeper learning of mechanisms, variability, and clinical curiosity. Educators do well to highlight opportunities to innovate even in relatively mundane situations, and to identify opportunities to practice efficiency even in highly complex cases. In this way, EM learners can be positioned in the so-called “optimal adaptability corridor,”15 being able to appropriately balance routinization with innovation, a skill unto itself (Figure).
It should come as no surprise that these conditions – a wide range of examples informed by a deep mechanistic understanding and an opportunity to explore both innovation and efficiency – sound familiar to the emergency physician. During COVID-19, EM practice moved from routine to adaptive expertise.
If we can now remain intentional about training for adaptability, it is possible that EM training programs can be the shining examples of training for adaptive expertise. As a maturing field, EM has retained its penchant for cutting edge innovation and its deserved reputation for flexibility and adaptability. As we continue to digest the worldwide response to the individual and system stressors brought about during the ongoing pandemic, it is not too soon to begin to celebrate the adaptability that EM has demonstrated. As educators, however, we need to focus on how we will teach for adaptability to ensure our learners are prepared for whatever the next disruptions will be. There must be room in our educational models for both business as usual (and how to do business as usual better), and for exploration beyond the bounds of what is usual. We believe that emergency physicians are well equipped to set the standard for learning the personal and organizational capacity for adaptability.
As we consider the training of future adaptive experts, we must recognize that their expertise will include negotiating the balance between compiled routine expertise (efficiency) and reflective, disruptive and on-demand expertise (innovation), and the ability to identify when to toggle between them (adaptability).18 Our training mindset must continue to mirror these processes: nimble, flexible, and responsive to the changing needs of our health systems and our learners. When the system strains under stress, this adaptive expertise becomes not just admirable, but necessary.
Footnotes
Section Editor: Jeffrey Love, MD
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Chris Merritt, MD, MPH, MHPE, Alpert Medical School of Brown University, Department of Emergency Medicine, 593 Eddy St., Claverick 264, Providence, RI 02903. Email: cmerritt@brown.edu. 1 / 2022; 23:56 – 58
Submission history: Revision received November 1, 2021; Submitted November 1, 2021; Accepted November 26, 2021
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. No author has professional or financial relationships with any companies that are relevant to this study. There are no conflicts of interest or sources of funding to declare.
REFERENCES
1. Santen SA, Hemphill RR, Pusic M. The responsibility of physicians to maintain competency. JAMA. 2020;323(2):117-8.
2. Smith C. The structural vulnerability of healthcare workers during COVID-19: observations on the social context of risk and the equitable distribution of resources. Soc Sci Med. 2020;258:113119.
3. Miller IF, Becker AD, Grenfell BT, et al. Disease and healthcare burden of COVID-19 in the United States. Nat Med. 2020;26(8):1212-7.
4. Zaka A, Shamloo SE, Fiorente P, et al. COVID-19 pandemic as a watershed moment: a call for systematic psychological health care for frontline medical staff. J Health Psychol. 2020;25(7):883-7.
5. Colenda CC, Applegate WB, Reifler B V, et al. COVID-19: Financial stress test for academic medical centers. Acad Med. 2020;95(8):1143-5.
6. Arabi YM, Azoulay E, Al-Dorzi HM, et al. How the COVID-19 pandemic will change the future of critical care. Intensive Care Med. 2021;47(3):282-91.
7. Ruangsomboon O, Boonmee P, Nimmannit A. The COVID-19 pandemic: the effect on airway management in non-COVID emergency patients. BMC Emerg Med. 2021;21(1):97.
8. Russi CS, Heaton HA, Demaerschalk BM. Emergency medicine telehealth for COVID-19: minimize front-line provider exposure and conserve personal protective equipment. Mayo Clin Proc. 2020;95(10):2065-8.
9. Sweeney DA, Malhotra A. Coronavirus disease 2019 respiratory failure: What is the best supportive care for patients who require ICU admission?. Curr Opin Crit Care. 2021;27(5):462-7.
10. Blutinger EJ, Shahid S, Jarou ZJ, et al. Translating COVID-19 knowledge to practice: enhancing emergency medicine using the “wisdom of crowds.”. J Am Coll Emerg Physicians Open. 2021;2(1):e12356.
11. Walton H, Navaratnam AV, Ormond M, et al. Emergency medicine response to the COVID-19 pandemic in England: a phenomenological study. Emerg Med J. 2020;37(12):768-72.
12. Chaplin T, McColl T, Petrosoniak A, et al. “Building the plane as you fly”: simulation during the COVID-19 pandemic. CJEM. 2020;22(5):576-8.
13. Yaffee AQ, Peacock E, Seitz R, et al. Preparedness, adaptation, and innovation: approach to the COVID-19 pandemic at a decentralized, quaternary care department of emergency medicine. West J Emerg Med. 2020;21(6):63-70.
14. Bohle Carbonell K, Stalmeijer RE, Könings KD, et al. How experts deal with novel situations: a review of adaptive expertise. Educ Res Rev. 2014;12:14-29.
15. Bransford JD, Schwartz DL. Rethinking transfer: a simple proposal with multiple implications. Rev Res Educ. 1999;24:61-100.
16. Mylopoulos M, Brydges R, Woods NN, et al. Preparation for future learning: a missing competency in health professions education?. Med Educ. 2016;50(1):115-23.
17. Regan L, Hopson LR, Gisondi MA, et al. Learning to learn: a qualitative study to uncover strategies used by master adaptive learners in the planning of learning. Med Teach. 2019;41(11):1252-62.
18. Pusic MV, Santen SA, Dekhtyar M, et al. Learning to balance efficiency and innovation for optimal adaptive expertise. Med Teach. 2018;40(8):820-7.