
{kind=link}
| Author | Affiliation |
|---|---|
| Shane Daugherty, MS | Lake Erie College of Osteopathic Medicine, Erie, Pennsylvania |
| Briana King, DO | Saint Vincent Hospital, Department of Emergency Medicine, Allegheny Health Network, Erie, Pennsylvania |
| Melody Milliron, DO | Saint Vincent Hospital, Department of Emergency Medicine, Allegheny Health Network, Erie, Pennsylvania |
| Jestin N. Carlson, MD, MS | Saint Vincent Hospital, Department of Emergency Medicine, Allegheny Health Network, Erie, Pennsylvania |
ABSTRACT
Case Presentation
A 50-year-old male with a history of multiple sclerosis with dizziness and nystagmus presented to the emergency department. On physical exam, nystagmus was noted. Computed tomography of the head without contrast was obtained showing a low density in the left frontal lobe. During admission, magnetic resonance imaging (MRI) findings were consistent with Balò’s concentric sclerosis.
Discussion
Balò’s concentric sclerosis is a rare, inflammatory demyelinating disease, often considered to be an infrequent variant of multiple sclerosis with alternating rings of healthy myelin and demyelination leading to pathognomonic findings of concentric lamella on T2 or contrast-enhanced T1 MRI imaging.
CASE PRESENTATION
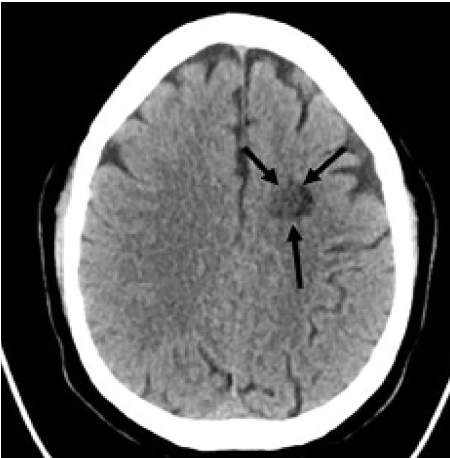
A 50-year-old White male with a history of multiple sclerosis presented to the emergency department with fatigue, lightheadedness, and dizziness, exacerbated with sitting upright and worsening over the prior one to two days. He stated his last flare was approximately two years prior, and presented with aphasia as his primary symptom. On physical exam, the patient had non-fatigable horizontal bidirectional nystagmus with no other abnormalities noted. Non-contrast computed tomography of the head showed an indeterminate 13- millimeter low density in the left frontal lobe (Image 1).
DISCUSSION
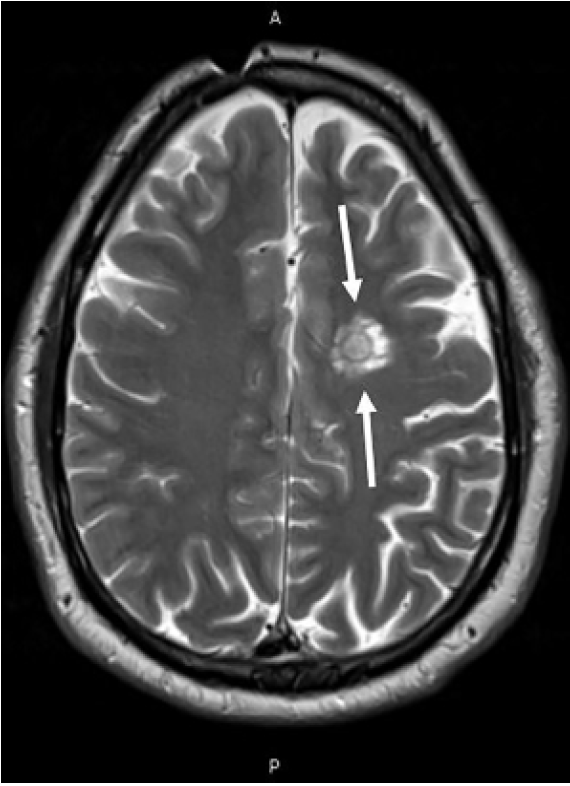
Balò’s concentric sclerosis (BCS) is a rare inflammatory demyelinating disease, often considered to be an infrequent variant of multiple sclerosis. Initially termed leuko-encephalitis periaxialis concentrica due to its pathognomonic MRI findings, BCS was originally considered a rapidly progressive encephalopathy that was universally fatal1,3; however, it has recently been associated with spontaneous remission.1 Balò’s concentric sclerosis typically affects young adults with a mean age of 37 at diagnosis,1 and is most commonly noted in Asian and Filipino populations.3 Lesions are most commonly found in the cerebrum and cerebellum.2 Alternating rings of healthy myelin and demyelination lead to the unique and pathognomonic MRI findings of a whorled appearance of concentric lamella on T2 or contrast-enhanced T1 imaging (Image 2).4 The clinical presentation of BCS is heterogenous, with symptoms often indicative of a mass-like lesion depending on lesion location. Treatment options range from high-dose intravenous steroids to immunosuppressive agents.5 Our patient was admitted and treated conservatively with intravenous fluids, meclizine, and promethazine. He was discharged on hospital day two without complications, and was referred for outpatient vestibular rehabilitation evaluation.
CPC-EM Capsule
What do we already know about this clinical entity?
Dizziness is a common presenting complaint in the emergency department. Balò’s concentric sclerosis (BCS) is unlikely to be included in the differential for dizziness with nystagmus.
What is the major impact of the image(s)?
The presented images will broaden the differential diagnosis in patients with intracerebral lesions on computed tomography.
How might this improve emergency medicine practice?
Consideration of BCS in the differential could lead to a neurology rather than neurosurgical referral, allowing earlier diagnosis and treatment.
Footnotes
Section Editor: Shadi Lahham, MD
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
The authors attest that their institution requires neither Institutional Review Board approval, nor patient consent for publication of this case report. Documentation on file.
Address for Correspondence: Melody Milliron, DO, Saint Vincent Hospital, Department of Emergency Medicine, 232 West 25th St, Erie, PA 16502. Email: melody.milliron@ahn.org. 5:123 – 124
Submission history: Revision received May 27, 2020; Submitted October 10, 2020; Accepted October 16, 2020
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Karaarslan E, Altintas A, Senol U, et al. Balò’s concentric sclerosis: clinical and radiologic features of five cases. AJNR Am J Neuroradiol. 2001;22(7):1362-7.
2. Kreft KL, Mellema SJ, Hintzen RQ. Spinal cord involvement in Balo’s concentric sclerosis. J Neurol Sci. 2009;279(1–2):114-7.
3. Amini Harandi A, Esfandani A, Pakdaman H, et al. Balò’s concentric sclerosis: an update and comprehensive literature review. Rev Neurosci. 2018;29(8):873-82.
4. Kastrup O, Stude P, Limmroth V. Balò’s concentric sclerosis. Evolution of active demyelination demonstrated by serial contrast-enhanced MRI. J Neurol. 2002;249(7):811-4.
5. Pietroboni AM, Arighi A, De Riz MA, et al. Balò’s concentric sclerosis: still to be considered as a variant of multiple sclerosis?. Neurol Sci. 2015;36(12):2277-80.