
{kind=link}
| Author | Affiliation |
|---|---|
| Michael A. Darracq, MD | Department of Emergency Medicine, Naval Medical Center San Diego |
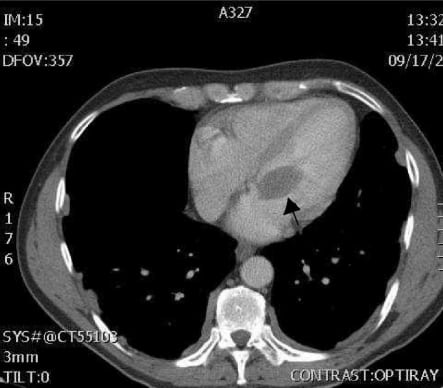
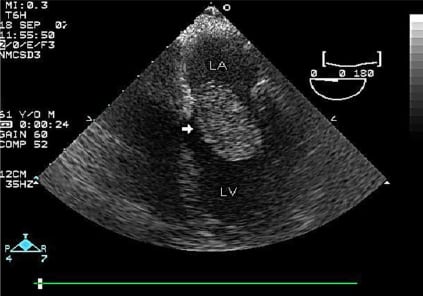
A 64-year-old white male presented to the Emergency Department with complaints of 24 hours of right lower quadrant abdominal pain. The patient was without past medical or surgical history. Review of systems was remarkable for nausea without vomiting and absence of urinary symptoms or change in bowel habits. Physical examination was significant for a blood pressure of 136/76 mm Hg, a heart rate of 95 beats per minute, respiratory rate of 16 breaths per minute, and temperature of 98.7 degrees Fahrenheit. Pulse oximetry was recorded at 100% on room air. Patient was an alert, well-appearing adult male with exquisite tenderness to palpation over the right lower quadrant without guarding, rebound, or rigidity. The rest of the physical examination and the laboratory evaluation were without significant findings or abnormalities. A CT scan of the abdomen and pelvis (Figure 1) with P.O. and I.V. contrast is shown demonstrating an intra-cardiac soft tissue mass (closed dark arrow). No intra-abdominal/pelvic radiographic findings to explain the patient’s abdominal pain were found. Subsequent bedside echocardiography demonstrated a 1.5cm × 2.5 cm left-sided atrial myxoma that extended into left ventricle during systole (Figure 2, white arrow). Atrial myxomas are rare, benign, intra-cardiac tumors with a wide spectrum of symptoms related to location, embolization, and propensity to obstruct blood flow through the heart.1,2 These are often difficult to diagnose. Most commonly, left-sided atrial myxomas present with dyspnea on exertion, dizziness, syncope, neurological signs and symptoms as a result of systemic embolization.1,2 Right-sided atrial myxomas present with easy fatigability, peripheral edema and ascites, or pulmonary embolism.3,4 Additionally, pain resulting from embolic infarction of solid and hollow organs has been reported in the literature.5,6
Subsequent to resection of the myxoma, the patient had complete resolution of the abdominal pain. No cause was ever identified.
Footnotes
Supervising Section Editor: Eric R. Snoey, MD
Submission history: Submitted November 28, 2007; Revision Received March 17, 2008; Accepted March 18, 2008.
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Michael A. Darracq MD, Department of Emergency Medicine, Naval Medical Center San Diego, 34800 Bob Wilson Drive, San Diego, CA 92134
Email: mike.darracq@gmail.com
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Pinede L, Duhaut P, Loire R. Clinical presentation of left atrial cardiac myxoma. A series of 112 consecutive cases. Medicine (Baltimore) 2001;80:159–172. [PubMed]
2. Larsson S, Lepore V, Kennergren C. Atrial myxomas: results of 25 years’ experience and review of the literature. Surgery. 1989;105:695–698. [PubMed]
3. McCoskey EH, Mehta JB, Krishnan K, Roy TM. Right atrial myxoma with extracardiac manifestations. Chest. 2000;118:547–549. [PubMed]
4. De Carli S, Sechi LA, Ciani R, Barillari G, Dolceti G, Bartoli E. Right atrial myxoma with pulmonary embolism. Cardiology. 1994;84:368–372. [PubMed]
5. Sögaard PE. Free ball thrombus of the left atrium. Eur J Cardiol. 1981;12:177–179.[PubMed]
6. Fujisaki K, Shohno Y, Yoshida T, et al. Acute renal infarction in a patient with left atrial myxoma. Clin Nephrol. 2007;67:53–57. [PubMed]