
{kind=link}
| Author | Affiliation |
|---|---|
| Cheng-Yi Wu, MD | National Taiwan University Hospital, Department of Emergency Medicine, Taipei, Taiwan |
| Tsung-Chien Lu, MD, PhD | National Taiwan University Hospital, Department of Emergency Medicine, Taipei, Taiwan; National Taiwan University, College of Medicine, Department of Emergency Medicine, Taipei, Taiwan |
| Pei-I Su, MD | National Taiwan University Hospital, Department of Emergency Medicine, Taipei, Taiwan |
| Chu-Lin Tsai, MD, ScD | National Taiwan University Hospital, Department of Emergency Medicine, Taipei, Taiwan; National Taiwan University, College of Medicine, Department of Emergency Medicine, Taipei, Taiwan |
| Joyce Tay, MD | National Taiwan University Hospital, Department of Emergency Medicine, Taipei, Taiwan |
| Meng-Che Wu, MD | National Taiwan University Hospital, Department of Emergency Medicine, Taipei, Taiwan |
| Eric H Chou, MD | Baylor Scott and White All Saints Medical Center, Department of Emergency Medicine, Fort Worth, TX; Baylor University Medical Center, Department of Emergency Medicine, Dallas, TX |
| Chih-Hung fcWang, MD, PhD | National Taiwan University Hospital, Department of Emergency Medicine, Taipei, Taiwan; National Taiwan University, College of Medicine, Department of Emergency Medicine, Taipei, Taiwan |
| Chien-Hua Huang, MD, PhD | National Taiwan University Hospital, Department of Emergency Medicine, Taipei, Taiwan; National Taiwan University, College of Medicine, Department of Emergency Medicine, Taipei, Taiwan |
| Wen-Jone Chen, MD, PhD | National Taiwan University Hospital, Department of Emergency Medicine, Taipei, Taiwan; National Taiwan University, College of Medicine, Department of Emergency Medicine, Taipei, Taiwan; National Taiwan University Hospital and National Taiwan University College of Medicine, Department of Internal Medicine, Division of Cardiology, Taipei, Taiwan; Min-Shen General Hospital, Taoyuan, Taiwan |
Introduction
Methods
Results
Discussion
Limitations
Conclusion
ABSTRACT
Introduction
The return of spontaneous circulation after cardiac arrest (RACA) score is a well-validated model for estimating the probability of return of spontaneous circulation (ROSC) in patients with out-of-hospital cardiac arrest (OHCA) by incorporating several variables, including gender, age, arrest aetiology, witness status, arrest location, initial cardiac rhythms, bystander cardiopulmonary resuscitation (CPR), and emergency medical services (EMS) arrival time. The RACA score was initially designed for comparisons between different EMS systems by standardising ROSC rates. End-tidal carbon dioxide (EtCO2) is a quality indicator of CPR. We aimed to improve the performance of the RACA score by adding minimum EtCO2 measured during CPR to develop the EtCO2 + RACA score for OHCA patients transported to an emergency department (ED).
Methods
This was a retrospective analysis using prospectively collected data for OHCA patients resuscitated at an ED during 2015–2020. Adult patients with advanced airways inserted and available EtCO2 measurements were included. We used the EtCO2 values recorded in the ED for analysis. The primary outcome was ROSC. In the derivation cohort, we used multivariable logistic regression to develop the model. In the temporally split validation cohort, we assessed the discriminative performance of the EtCO2 + RACA score by the area under the receiver operating characteristic curve (AUC) and compared it with the RACA score using the DeLong test.
Results
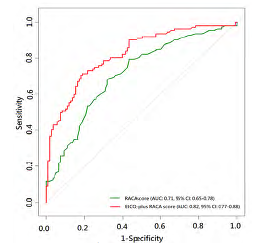
There were 530 and 228 patients in the derivation and validation cohorts, respectively. The median measurements of EtCO2 were 8.0 times (interquartile range [IQR] 3.0–12.0 times), with the median minimum EtCO2 of 15.5 millimeters of mercury (mm Hg) (IQR 8.0–26.0 mm Hg). The median RACA score was 36.4% (IQR 28.9–48.0%), and a total of 393 patients (51.8%) achieved ROSC. The EtCO2 + RACA score was validated with good discriminative performance (AUC, 0.82, 95% CI 0.77–0.88), outperforming the RACA score (AUC, 0.71, 95% CI 0.65–0.78) (DeLong test: P < 0.001).
Conclusion
The EtCO2 + RACA score may facilitate the decision-making process regarding allocations of medical resources in EDs for OHCA resuscitation.
INTRODUCTION
The global incidence of out-of-hospital cardiac arrest (OHCA) is estimated to be 28–44 people per 100,000 population annually.1 In Asia, according to the Pan-Asian Resuscitation Outcomes Study (PAROS) registry, only 5.4% of patients survived to hospital discharge and 2.7% of patients were able to recover favourable neurological function after OHCA.2
The concept of “chain of survival”3,4 has been proposed to streamline OHCA management to improve outcomes. With the advancement of resuscitation skills and equipment, most time-sensitive interventions can now be performed by emergency medical services (EMS) personnel in prehospital settings in a timely manner without being postponed until patients are transported to the emergency department (ED). To further improve outcomes, emergency physicians (EP) may initiate certain invasive interventions,5 such as extracorporeal cardiopulmonary resuscitation (CPR), for selected patients.
Accurate estimation for probability of return of spontaneous circulation (ROSC) is important for EPs in their decision-making regarding mobilising medical resources for these selected patients. The RACA6 score was developed to estimate the ROSC probability after OHCA and is composed of several variables, including gender, age, arrest aetiology, witness status, arrest location, initial cardiac rhythms, bystander CPR, and EMS arrival time. Nonetheless, the RACA score was initially designed for comparisons between different EMS systems by standardising ROSC rates rather than for predicting ROSC probabilities of individual patients.
End-tidal carbon dioxide (EtCO2) refers to the concentration of carbon dioxide at the end of exhalation, which is determined by pulmonary blood flow generated during CPR,7,8 and is suggested to be maintained above at least 10 millimetres of mercury (mm Hg) to increase ROSC probability.9,10 Therefore, in the current study we attempted to develop the EtCO2 + RACA score by combining the RACA score, a baseline risk-stratifying model, and minimum EtCO2 (a CPR quality indicator) to provide EPs with an accurate estimated ROSC probability of OHCA patients sent to the ED for ongoing CPR.
METHODS
We performed this study by retrospectively analysing a registry database, which prospectively collected data of OHCA patients sent to the ED of the National Taiwan University Hospital (NTUH) for resuscitation. The results are reported according to the Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD) statement.11
Ethical Statements
This study was conducted in accordance with the Declaration of Helsinki amendments. The institutional review board approved this study (reference number: 201906082RINB) and waived the requirement for informed consent.
Population Health Research Capsule
What do we already know about this issue?
The return of spontaneous circulation after cardiac arrest (RACA) score was developed to estimate the probability of RACA.
What was the research question?
Can end-tidal carbon dioxide (EtCO2), a quality indicator of cardiopulmonary resuscitation, be used to improve the RACA score?
What was the major finding of the study?
The EtCO2 + RACA score (AUC 0.82, 95% CI 0.77–0.88) outperformed the original RACA score (AUC 0.7, 95% CI 0.65–0.78; P < 0.001).
How does this improve population health?
The EtCO2 + RACA score may help allocate medical resources in emergency departments during resuscitation of out-of-hospital cardiac arrest.
Study Setting
The NTUH Hospital has 2,600 beds, including 220 beds in intensive care units, and there are approximately 100,000 patient visits to the NTUH ED each year. For OHCA, CPR is performed according to the resuscitation guidelines.9,10 Furthermore, since 2013 ED personnel who may be involved in the resuscitation of OHCA, including clinicians and nursing staff, have received a specialised training course of the Advanced Cardiac Life Support (ACLS) teamwork model.12,13 This training model addresses both CPR techniques and non-technical skills.14,15 Any interventions performed during CPR are timestamped by nurses using a specially designed tablet app. The cardiac rhythm and EtCO2 are recorded every two minutes during pulse checking and then uploaded to the electronic health record. The EtCO2 is monitored by devices attached to the supraglottic airway (SGA) or endotracheal tube (ETT).
The decision to insert advanced airways, including SGA or ETT, during CPR is at the discretion of the treating physicians. Nonetheless, in our practice most clinicians tend to insert an ETT as soon as possible because, in the ACLS teamwork model, airway management is assigned to a dedicated squad of clinicians and nurses; thus, inserting an ETT does not influence delivery of high quality CPR. Also, for OHCA patients who never achieve ROSC, CPR would usually be performed for at least 30 minutes, except for those with a documented do-not-resuscitate (DNR) order.
Study Population
Consecutive OHCA patients resuscitated at the ED of NTUH between January 1 2015–December 31, 2020 were screened. Patients fulfilling the following criteria were eligible for inclusion in the study: 1) non-traumatic arrest; 2) absence of ROSC before ED arrival; 3) absence of documentation of DNR order before CPR; 4) transport by EMS; 5) age ≥18 years; 6) insertion of advanced airways, either SGA or ETT; and 7) availability of EtCO2 measurement at least once. If a single patient underwent CPR multiple times, we extracted only the first episode for analysis.
Data Collection, Variable Definitions, and Outcome Measures
In the NTUH ED registry, OHCA scenarios were recorded per the Utstein template.16 We used the following variables for analysis: age; gender; variables derived from the Utstein template; management by EMS and in the ED; measured EtCO2 levels; and outcomes.
We calculated the RACA score according to the original formula reported by Gräsner et al6 (Supplemental Table 1). Nonetheless, the variables of arrest aetiology and location were not explicitly defined by Gräsner et al.6 Hence, we defined these variables as follows: 1) After classifying aetiology into trauma, hypoxia, and intoxication in the RACA score, we excluded traumatic OHCA patients in our registry, while including patients with external causes of asphyxia,16 and patients with suspected drug overdose;16 and 2) we reclassified the arrest location as used in the RACA score. Nursing home designation included assisted living/nursing home; doctor’s office included primary care clinics; public place included sports/recreation event, street/highway, public building, and educational institution; and medical institution included dialysis clinics.
Finally, the initial cardiac rhythms used in the RACA score were those recorded by EMS at initial contact, which were classified into ventricular fibrillation, pulseless electrical activity (PEA), asystole, and other. Nonetheless, our EMS only categorised the initial cardiac rhythms into shockable and non-shockable rhythms. Therefore, we used the initial rhythms recorded upon ED arrival in computing the RACA score. In the NTUH ED registry, the initial 15 EtCO2 measurements were recorded. In the current analysis, we retrieved only the EtCO2 measured after insertion of advanced airways. The EtCO2 summary parameters were computed accordingly, including initial, maximum, minimum, and average EtCO2.
The ROSC was specified as the primary outcome and defined as a palpable pulse > 20 seconds, as used by Gräsner et al.6 We also reported survival and favourable neurological function at the time of hospital discharge. Favourable neurological function was defined as a score of 1 or 2 on the Cerebral Performance Category scale.17
Sample Size
Because of the retrospective nature of this study, the number of eligible patients during the study period determined the final sample size. We temporally split the final cohort into a derivation cohort and a validation cohort with the ratio of patient numbers being 70% vs 30%.
Statistical Analysis
Categorical variables are presented as counts with proportions, and continuous variables are presented as medians with interquartile ranges (IQR). We examined categorical variables by chi-square test, while continuous variables were compared by the Wilcoxon rank-sum test.
In the derivation cohort, we calculated the odds ratio (OR) as the outcome measure. We only tested the two predetermined variables, RACA score and minimum EtCO2 in the multivariable logistic regression analyses to estimate their association with the primary outcome. We employed generalised additive models (GAM)18 to explore non-linear effects of the RACA score or minimum EtCO2 on the primary outcome and to identify the optimal cut-off points to transform these variables into categorical variables, if necessary. Since we did not know whether there would be confounding effects or multicollinearity between the RACA score and minimum EtCO2, we still conducted formal, stepwise, variable selection procedure with iterations to derive the final prediction model. We defined the significance levels for entry and to stay at P = 0.15. We derived the final prediction model by excluding non-significant variables sequentially until all regression coefficients were significant.
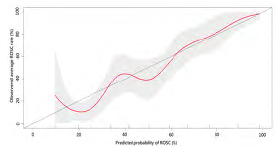
In the validation cohort, we assessed the discriminative performance of the derived model by area under the receiver operating characteristic (ROC) curve (AUC). We evaluated model calibration by the Hosmer–Lemeshow goodness-of-fit test and a calibration plot to compare predicted ROSC probabilities with the observed ROSC rates. We compared the AUCs of the EtCO2 + RACA and RACA scores by the DeLong test of correlated ROC curves.19 We used R 4.1.1 software (R Foundation for Statistical Computing, Vienna, Austria) to analyse the data. A two-tailed P-value < 0.05 was considered significant.
RESULTS
The patient selection procedure resulted in the final cohort of 758 patients (Supplemental Figure 1). We temporally split the final cohort on May 1, 2019, because the ratio of patient numbers in the derivation and validation cohorts was the closest to 70% vs 30%. The characteristics of the patients in the final cohort are presented in Table 1, and we made comparisons between the derivation and validation cohorts.
| Variables | Total cohort (N = 758) | Derivation cohort (n = 530) | Validation cohort (n = 228) | P-value |
|---|---|---|---|---|
| Age, year | 71.0 (60.0–82.0) | 73.0 (60.0–83.0) | 68.0 (59.0–79.0) | 0.005 |
| Age ≥ 80 years | 227 (29.9) | 173 (32.6) | 54 (23.7) | 0.01 |
| Male, n | 489 (64.5) | 335 (63.2) | 154 (67.5) | 0.25 |
| Arrest etiology, n | ||||
| Hypoxia | 40 (5.3) | 33 (6.2) | 7 (3.1) | 0.07 |
| Intoxication | 10 (1.3) | 7 (1.3) | 3 (1.3) | 0.99 |
| Arrest location, n | ||||
| At home | 455 (60.0) | 325 (61.3) | 130 (57.0) | 0.27 |
| Nursing home | 28 (3.7) | 25 (4.7) | 3 (1.3) | 0.02 |
| Doctor’s office | 13 (1.7) | 8 (1.5) | 5 (2.2) | 0.51 |
| Public place | 172 (22.7) | 109 (20.6) | 63 (27.6) | 0.03 |
| Medical institution | 6 (0.8) | 6 (1.1) | 0 (0) | 0.11 |
| Witness status, n | ||||
| Witness by bystander | 313 (41.3) | 214 (40.4) | 99 (43.4) | 0.44 |
| Witness by EMS | 58 (7.7) | 48 (9.1) | 10 (4.4) | 0.03 |
| Witness by bystander or EMS | 350 (46.2) | 242 (45.7) | 108 (47.4) | 0.67 |
| Bystander CPR, n | 398 (52.5) | 265 (50.0) | 133 (58.3) | 0.04 |
| EMS management | ||||
| Call to EMS arrival, minutes | 4.0 (3.0–5.0) | 4.0 (3.0–5.0) | 4.0 (3.0–6.0) | 0.01 |
| Prehospital SGA use, n | 527 (69.5) | 372 (70.2) | 155 (68.0) | 0.55 |
| Prehospital ETT use, n | 54 (7.1) | 37 (7.0) | 17 (7.5) | 0.82 |
| Prehospital epinephrine use, n | 187 (24.7) | 119 (22.5) | 68 (29.8) | 0.03 |
| Prehospital defibrillation, n | 150 (19.8) | 96 (18.1) | 96 (23.7) | 0.08 |
| Prehospital CPR duration, minutes | 17.0 (13.0–21.0) | 16.0 (12.0–20.0) | 19.0 (16.0–23.0) | <0.001 |
| ED management | ||||
| Initial cardiac rhythms at ED arrival, n | ||||
| Shockable rhythms | 51 (6.7) | 36 (6.8) | 15 (6.6) | 0.91 |
| PEA | 304 (40.1) | 215 (40.6) | 89 (39.0) | 0.69 |
| Asystole | 403 (53.2) | 279 (52.6) | 124 (54.4) | 0.66 |
| ED SGA use, n | 526 (69.4) | 371 (70.0) | 155 (68.0) | 0.58 |
| ED ETT use, n | 735 (97.0) | 510 (96.2) | 225 (98.7) | 0.07 |
| Available measurements of EtCO2, times | 8.0 (3.0–12.0) | 6.0 (3.0–11.0) | 11.0 (4.0–13.0) | <0.001 |
| EtCO2 summary parameters, mm Hg | ||||
| Initial | 26.0 (16.0–41.0) | 25.0 (16.0–40.0) | 27.0 (15.5–42.5) | 0.40 |
| Maximum | 39.0 (25.0–54.0) | 37.5 (24.0–52.0) | 41.0 (25.5–56.0) | 0.19 |
| Minimum | 15.5 (8.0–26.0) | 16.0 (9.0–26.0) | 15.0 (7.0–26.0) | 0.57 |
| Average | 26.4 (16.0–38.3) | 25.7 (16.5–37.8) | 27.4 (15.3–39.1) | 0.66 |
| ED CPR duration, min | 28.5 (12.0–32.0) | 26.0 (12.0–32.0) | 30.0 (13.0–31.0) | 0.38 |
| ROSC probability predicted by RACA score, % | 36.4 (28.9–48.0) | 36.4 (28.5–48.5) | 36.8 (29.3–47.5) | 0.69 |
| Outcome, n | ||||
| ROSC | 393 (51.8) | 281 (53.0) | 112 (49.1) | 0.33 |
| Survival to hospital discharge | 78 (10.3) | 53 (10.0) | 25 (11.0) | 0.69 |
| Favorable neurological outcome at hospital discharge | 41 (5.4) | 28 (5.3) | 13 (5.7) | 0.82 |
Data are presented as median (interquartile range) or counts (proportion). Bold-typed variables represent those used in the RACA score.
EMS, emergency medical service; CPR, cardiopulmonary resuscitation; SGA, supraglottic airway; ETT, endotracheal tube; ED, emergency department; EtCO2, end-tidal carbon dioxide; mm Hg, millimeters of mercury; PEA, pulseless electrical activity.
ROSC, return of spontaneous circulation; RACA, ROSC after cardiac arrest.
Overall, the median patient age was 71.0 years (IQR 60.0–82.0 years), and 489 patients (64.5%) were male. Only a small proportion of patients suffered from hypoxia- (5.3%, 40) or intoxication-associated (1.3%, 10) OHCA. Most OHCA occurred at home (60.0%, 455 patients). Approximately 46.2% of OHCA (350 patients) was witnessed by bystanders or EMS, and 52.5% of them received bystander CPR (398 patients). The median time interval between call and EMS arrival was 4.0 minutes (min) (IQR 3.0–5.0 min). A total of 527 patients (69.5%) received SGA placement during prehospital CPR, while 735 patients (97.0%) received an ETT during CPR at the ED. Most of the initial cardiac rhythms recorded upon ED arrival were non-shockable rhythms, including PEA (40.1%, 304 patients) and asystole (53.2%, 403 patients). The median available measurements of EtCO2 were 8.0 times (IQR: 3.0–12.0 times), with the median minimum EtCO2 of 15.5 mm Hg (IQR: 8.0–26.0 mm Hg). The median RACA score was 36.4% (28.9–48.0%), and a total of 393 patients (51.8%) achieved ROSC.
The differences between patients stratified by ROSC in the derivation cohort are shown in Table 2. Significant differences between patients with and without ROSC were noted in approximately half of the variables included in the RACA score, including age ≥80 years, hypoxia, public place, witness by bystander or EMS, PEA, and asystole. Values of all EtCO2 summary parameters were significantly higher in patients with than without ROSC. The GAM plots (Supplemental Figure 2) demonstrated a near-linear association between minimum EtCO2 and ROSC. Therefore, we analysed minimum EtCO2 as a continuous variable without transformation.
| Variables | Derivation cohort (n = 530) | ROSC (n = 281) | Absence of ROSC (n = 249) | P-value |
|---|---|---|---|---|
| Age, year | 73.0 (60.0–83.0) | 70.0 (60.0–82.3) | 75.0 (61.0–84.0) | 0.05 |
| Age ≥ 80 years | 173 (32.6) | 80 (28.5) | 93 (37.3) | 0.03 |
| Male, n | 335 (63.2) | 188 (66.9) | 147 (59.0) | 0.06 |
| Arrest etiology, n | ||||
| Hypoxia | 33 (6.2) | 25 (8.9) | 8 (3.2) | 0.007 |
| Intoxication | 7 (1.3) | 4 (2.5) | 3 (1.2) | 0.83 |
| Arrest location, n | ||||
| At home | 325 (61.3) | 148 (52.7) | 177 (71.1) | <0.001 |
| Nursing home | 25 (4.7) | 10 (3.6) | 15 (6.0) | 0.18 |
| Doctor’s office | 8 (1.5) | 6 (2.1) | 2 (0.8) | 0.21 |
| Public place | 109 (20.6) | 74 (26.3) | 35 (14.1) | <0.001 |
| Medical institution | 6 (1.1) | 5 (1.8) | 1 (0.4) | 0.13 |
| Witness status, n | ||||
| Witness by bystander | 214 (40.4) | 141 (50.2) | 73 (29.3) | <0.001 |
| Witness by EMS | 48 (9.1) | 35 (12.5) | 13 (5.2) | 0.004 |
| Witness by bystander or EMS | 242 (45.7) | 161 (57.3) | 81 (32.5) | <0.001 |
| Bystander CPR, n | 265 (50.0) | 142 (50.5) | 123 (49.4) | 0.79 |
| EMS management | ||||
| Call to EMS arrival, minutes | 4.0 (3.0–5.0) | 4.0 (3.0–5.0) | 4.0 (3.0–5.0) | 0.15 |
| Prehospital SGA use, n | 372 (70.2) | 189 (67.3) | 183 (73.5) | 0.12 |
| Prehospital ETT use, n | 37 (7.0) | 15 (5.3) | 22 (8.8) | 0.12 |
| Prehospital epinephrine use, n | 119 (22.5) | 56 (19.9) | 63 (25.3) | 0.14 |
| Prehospital defibrillation, n | 96 (18.1) | 68 (24.2) | 28 (11.2) | <0.001 |
| Prehospital CPR duration, minutes | 16.0 (12.0–20.0) | 16.0 (11.0–19.0) | 17.0 (13.0–20.0) | 0.005 |
| ED management | ||||
| Initial cardiac rhythms at ED arrival, n | ||||
| Shockable rhythms | 36 (6.8) | 30 (10.7) | 6 (2.4) | <0.001 |
| PEA | 215 (40.6) | 132 (47.0) | 83 (33.3) | 0.001 |
| Asystole | 279 (52.6) | 119 (42.3) | 160 (64.3) | <0.001 |
| ED SGA use, n | 371 (70.0) | 189 (67.3) | 182 (73.1) | 0.14 |
| ED ETT use, n | 510 (96.2) | 271 (96.4) | 239 (96.0) | 0.78 |
| Available measurements of EtCO2, times | 6.0 (3.0–11.0) | 4.0 (2.0–8.0) | 10.0 (5.0–13.0) | <0.001 |
| EtCO2 summary parameters, mm Hg | ||||
| Initial | 25.0 (16.0–40.0) | 31.0 (21.0–45.0) | 21.0 (12.0–30.3) | <0.001 |
| Maximum | 37.5 (24.0–52.0) | 43.0 (30.0–57.0) | 31.0 (18.0–48.0) | <0.001 |
| Minimum | 16.0 (9.0–26.0) | 22.0 (15.0–32.3) | 11.0 (5.0–18.0) | <0.001 |
| Average | 25.7 (16.5–37.8) | 30.5 (22.9–43.1) | 19.9 (11.2–29.1) | <0.001 |
| ED CPR duration, minutes | 26.0 (12.0–32.0) | 14.0 (9.0–28.0) | 31.0 (27.0–34.0) | <0.001 |
| ROSC probability predicted by RACA score, % | 36.4 (28.5–48.5) | 41.1 (31.4–54.5) | 31.9 (26.1–39.8) | <0.001 |
Data are presented as median (interquartile range) or counts (proportion). Bold-typed variables represent those used in the RACA score.
EMS, emergency medical service; CPR, cardiopulmonary resuscitation; SGA, supraglottic airway.
ETT, endotracheal tube; ED, emergency department; EtCO2, end-tidal carbon dioxide; mm Hg, millimeters of mercury; PEA, pulseless electrical activity.
After stepwise variable selection, the final EtCO2 + RACA score resulted in good discriminative performance in the derivation cohort (AUC 0.80, 95% CI 0.76–0.83; Table 3) (online EtCO2 + RACA score calculator: https://chou2.chou-tw.com/index.php/etco2/). In the validation cohort, the EtCO2 +RACA score also demonstrated good discriminative performance (AUC 0.82, 95% CI 0.77–0.88), significantly outperforming the RACA score (AUC 0.71, 95% CI 0.65–0.78) (DeLong test: P < 0.001) (Figure 1). Finally, the calibration plot (Figure 2) indicated that EtCO2 + RACA score was calibrated well in the validation cohort (Hosmer–Lemeshow test: P = 0.33).
| Intercept and predictors | β coefficient | Odds ratio (95% CI) | P-value |
|---|---|---|---|
| Intercept | −3.34284 | ||
| RACA score | 5.76509 | 318.97 (62.63–1624.36) | <0.001 |
| Minimum EtCO2, mm Hg | 0.06721 | 1.07 (1.05–1.09) | <0.001 |
The predicted probability of return of spontaneous circulation (ROSC) can be calculated using the following formula: probability of ROSC = 1/{1 + exp[−(−3.34284 + RACA score × 5.76509 + minimum EtCO2 × 0.06721)]}.
EtCO2, end-tidal carbon dioxide; RACA, return of spontaneous circulation after cardiac arrest.
DISCUSSION
Main Findings
Based on the RACA score, we developed and validated a logistic regression model, the EtCO2 + RACA score, to facilitate estimating ROSC probability of OHCA patients transported to EDs for continuing CPR. By adding minimum EtCO2 to the original RACA score, the discriminative performance of the EtCO2 + RACA score significantly outperformed the original RACA score. By combining a baseline risk-stratifying score and a CPR quality indicator, the EtCO2 + RACA score may assist EPs in decision-making regarding OHCA management.
Comparisons with Previous Studies
For OHCA patients, most prediction models were designed for those who had achieved ROSC,20 with only a few models available for patients who were still undergoing CPR. By using registry data, Baldi et al21 used Utstein-based (UB) variables to develop the UB-ROSC score for predicting the probability of survival to hospital admission of an OHCA victim with AUCs above 0.77. Also, according to the Utstein-based variables recorded in the PAROS registry, Liu et al22 employed machine-learning to derive the prehospital (P-ROSC) score to predict the individualized probability of P-ROSC23 with an AUC of 0.806. The RACA score6 was originally developed for predicting ROSC after OHCA, using readily available factors when EMS personnel arrive at the scene. With slight differences in definitions, these RACA score-related variables were similar to the Utstein-based ones used by UB-ROSC21 and P-ROSC, 22 suggesting that these variables might be employed to make individualized predictions. In the validation cohort of the original study by Gräsner et al,6 the RACA score achieved a fair discriminative performance (AUC 0.73).
The RACA score has been validated in many regions, including Finland (AUC 0.71),24 Asia (AUC 0.74),25 Italy, and Switzerland (AUC 0.76),26 as well as in our validation cohort (AUC 0.71), suggesting that the RACA score is generalisable and applicable to a wide range of diverse populations. Our validation cohort had a higher proportion of non-shockable rhythms above 90% (PEA: 39.0%, asystole: 54.4%), compared with the validation cohort of the Gräsner et al6 study (PEA: 15.0%, asystole: 46.6%). Despite the substantial difference in the presenting rhythms, the discriminative performance of the RACA score in our validation cohort was similar to that in previous studies (AUC 0.71, Figure 1). Therefore, we adopted the RACA score in our study to calculate the baseline probability of ROSC.
The ROSC rate (51.8%) of our total cohort was slightly higher than the ROSC rate (43.3%) reported by Gräsner et al,6 despite the fact that the proportions of non-shockable rhythms were higher in our study. When using the EMS registry of our city, the Chiang et al study27 reported the proportion of survival or favourable neurological outcome at hospital discharge among OHCA patients receiving ETT or SGA was 7.2% and 3.1%, respectively, similar to our results (survival: 10.3%, favourable neurological outcome: 5.4%). Chiang et al27 also noted high proportions of non-shockable rhythms (89.2%) and sustained ROSC of ≥2 hours (26.6%) among these patients. Since ROSC was defined as a palpable pulse lasting longer than 20 seconds6 in our study, the seemingly high ROSC rate may be reasonable.
The RACA score tended to underestimate the ROSC probability in our cohort, with predicted vs observed ROSC rate being 36.4% vs 51.8% (Table 1). This miscalibration may have occurred because in the original study in which the RACA score was developed,6 the arrest aetiology and location were not classified according to the Utstein template16 and needed to be reclassified in our study retrospectively. Furthermore, the component variables of the RACA score, such as age or arrest location, were all baseline variables and unmodifiable during CPR. These baseline variables may not reflect the highly dynamic nature of CPR. That is, if the ROSC probability predicted by the RACA score was low, the outcomes could still be improved by high quality CPR; in contrast, even if the RACA score predicted a high ROSC probability, the outcomes may still be compromised if CPR quality was poor. Hence, to make individualised prognostication during CPR, variables specific to the patient and resuscitation process such as EtCO2 may be more helpful.
Interpretation of Current Studies
The systematic review by Paiva et al28 indicated that EtCO2 was associated with ROSC probability, likely because EtCO2 could reflect CPR quality. Nonetheless, the optimal parameter for EtCO2 being a prognostic factor is still under debate.28 For example, the so-called “initial” EtCO2 may not be truly measured at the initial stage of CPR since an ETT may be inserted at a later stage of CPR. Also, the maximum EtCO2 may be confusing since it did not account for the influence of measurement timing, ie, whether the predictive value of a maximum EtCO2 measured at the early stage of CPR was the same as that measured at the late stage of CPR. Average EtCO2 was also a frequently reported parameter. Despite its convenience in summarising the overall measured EtCO2, average EtCO2 could not differentiate between different EtCO2 trends. While ascending and descending EtCO2 trends may have similar average EtCO2, their prognoses may be very different.29 Furthermore, average EtCO2 is not very practical in clinical application since clinicians may not be able to compute the average EtCO2 in real time. Lastly, the most promising parameter in predicting ROSC may be the minimum EtCO2 since this parameter may reflect the minimum CPR quality achieved by rescuers.
The higher the minimum EtCO2, the higher the ROSC probability would be (Supplemental Figure 2). Similarly, the systematic review of Paiva et al28 indicated that EtCO2 ≥ 20 mm Hg was a stronger predictor for ROSC than EtCO2 ≥10 mm Hg. An abrupt rise of EtCO2 over 40 mm Hg was suggested to be the first sign of ROSC.28 For minimum EtCO2 ≤40 mm Hg, the higher EtCO2 may indicate higher CPR-generated cardiac output and better CPR quality. In contrast, for minimum EtCO2 >40 mm Hg, the high EtCO2 may simply suggest that the cardiac arrest was caused by asphyxia or hypercapnic respiratory failure prior to collapse rather than augmented cardiac output.30
Our research has several advantages over previous studies28 in investigating EtCO2 as an outcome predictor. First, as one part of the ACLS teamwork model,12,13 the EtCO2 is routinely recorded in our ED. Second, the clinical practice is consistent across different clinicians who treat OHCA in our ED’s resuscitation bay. As shown in Table 1, the proportions of ETT use in the ED were similarly high in the derivation and validation cohorts. Finally, CPR is usually performed for approximately 30 min in patients who never achieve ROSC (median duration of CPR performed in the ED was 28.5 min, Table 1), which would not be shortened simply because of clinicians’ perception of poor prognosis for the patient. This practice may help circumvent the “bias of self-fulfilling prophecy”31 since EtCO2 has been proposed as a variable in the termination of resuscitation rule.9
Future Applications
In most Asian countries, EMS personnel are usually not legally allowed to pronounce death2 and must transfer OHCA patients to EDs despite most interventions of Advanced Life Support being able to be performed in prehospital resuscitation. The EPs resuscitating EMS-transported patients are faced with the problem of whether resuscitation should be continued as set up by EMS personnel or further invasive interventions should be implemented. Advanced therapeutics, such as extracorporeal CPR5 or resuscitative endovascular balloon occlusion of the aorta,32 are being tested and may be applicable in the near future for OHCA. Nonetheless, these interventions may only be beneficial in a certain group of patients. A prediction model like the EtCO2 + RACA score may assist EPs in determining whether the interventions should be upgraded for an individual patient. It should be emphasized that like other scoring systems predicting ROSC for OHCA patients,21,22 the EtCO2 + RACA score is not intended to terminate CPR for OHCA patients. With the assistance of advanced technology, the EtCO2 + RACA score may be computed instantaneously along with the real-time updated minimum EtCO2 during CPR. Further studies are needed to validate the EtCO2 + RACA score and explore the possibility of integrating the prediction model, internet-based devices, and the resuscitation process.
LIMITATIONS
First, the analysed EtCO2 dataset was derived from a prospectively collected database of a single centre with a specialised training model for CPR. The median of the minimum EtCO2 was higher than 10 mm Hg (Table 1), revealing the high CPR quality achieved by the ACLS teamwork model. Further studies are needed to investigate the generalisability of our results. Second, as suggested by the TRIPOD statement,11 the temporally split derivation and validation cohorts allowed non-random variation between the two cohorts, and this kind of validation could be considered an intermediary between internal and external validation.
Even the number of measurements of EtCO2 was significantly higher in the validation than the derivation cohort (Table 1), suggesting that the ACLS teamwork model matured with time. Despite this advantage in the validation procedure, further external validation of the EtCO2 + RACA score in other communities is needed because this model was developed from a single medical centre. Finally, we only used EtCO2 recorded in the ED to develop the EtCO2 + RACA score. Because of the limitations in the facility and human resources, the EtCO2 values were not recorded at regular time intervals in the field and during transport. Future studies are needed to test whether the EtCO2 values measured by EMT during CPR could further improve the performance of the EtCO2 + RACA score.
CONCLUSION
The derived EtCO2 +RACA score may be used to assist emergency physicians in estimating the probability of return of spontaneous circulation for EMS-transported patients with out-of-hospital cardiac arrest. By adding a CPR quality indicator, minimum EtCO2, to the well-validated RACA score, the EtCO2 + RACA score achieved good discriminative performance. The EtCO2 + RACA score may facilitate the decision-making process regarding allocations of medical resources in EDs for OHCA resuscitation. Nonetheless, it should be emphasized that the EtCO2 + RACA score is not intended to terminate CPR. Further validation by external datasets is warranted to ensure the generalizability of the EtCO2 + RACA score.
Footnotes
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Chih-Hung Wang, MD, PhD, National Taiwan University Hospital, Department of Emergency Medicine, No.7, Zhongshan S. Rd., Zhongzheng Dist., Taipei City 100, Taiwan. Email: chwang1981@ntu.edu.tw. 5 / 2023; 24:605 – 614
Submission history: Revision received September 25, 2023; Submitted February 2, 2023; Accepted January 24, 2023
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. No author has professional or financial relationships with any companies that are relevant to this study. There are no conflicts of interest or sources of funding to declare.
REFERENCES
1. Berdowski J, Berg RA, Tijssen JG, et al. Global incidences of out-of-hospital cardiac arrest and survival rates: systematic review of 67 prospective studies. Resuscitation. 2010;81(11):1479-87.
2. Ong ME, Shin SD, De Souza NN, et al. Outcomes for out-of-hospital cardiac arrests across 7 countries in Asia: the Pan Asian Resuscitation Outcomes Study (PAROS). Resuscitation. 2015;96:100-8.
3. Merchant RM, Topjian AA, Panchal AR, et al. Part 1: Executive Summary: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020;142(16_suppl_2):S337-57.
4. Semeraro F, Greif R, Böttiger BW, et al. European Resuscitation Council Guidelines 2021: systems saving lives. Resuscitation. 2021;161:80-97.
5. Yannopoulos D, Bartos J, Raveendran G, et al. Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST): a phase 2, single centre, open-label, randomised controlled trial. Lancet. 2020;396(10265):1807-16.
6. Gräsner J-T, Meybohm P, Lefering R, et al. ROSC after cardiac arrest—the RACA score to predict outcome after out-of-hospital cardiac arrest. Eur Heart J. 2011;32(13):1649-56.
7. Garnett AR, Ornato JP, Gonzalez ER, et al. End-tidal carbon dioxide monitoring during cardiopulmonary resuscitation. JAMA. 1987;257(4):512-5.
8. Sandroni C, De Santis P, D’Arrigo S. Capnography during cardiac arrest. Resuscitation. 2018;132:73-7.
9. Panchal AR, Bartos JA, Cabañas JG, et al. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020;142(16_suppl_2):S366-468.
10. Soar J, Böttiger BW, Carli P, et al. European Resuscitation Council Guidelines 2021: Adult Advanced Life Support. Resuscitation. 2021;161:115-51.
11. Collins GS, Reitsma JB, Altman DG, et al. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): the TRIPOD statement. Ann Intern Med. 2015;162(1):55-63.
12. Chong KM, Wu C-H, Lin J-J, et al. Advanced cardiac life support (ACLS) is all about airway-circulation-leadership-support (A-C-L-S): a novel cardiopulmonary resuscitation (CPR) teamwork model. Resuscitation. 2016;106:e11-2.
13. Lin CH, Lin HY, Tseng WP, et al. Resuscitation teamwork during the COVID-19 pandemic in the emergency department: challenges and solutions. Resuscitation. 2021;160:18-9.
14. Soar J, Monsieurs KG, Ballance JH, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 9. Principles of Education in Resuscitation. Resuscitation. 2010;81(10):1434-44.
15. Bhanji F, Mancini ME, Sinz E, et al. Part 16: Education, Implementation, and Teams: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18 Suppl 3):S920-33.
16. Perkins GD, Jacobs IG, Nadkarni VM, et al. Cardiac Arrest and Cardiopulmonary Resuscitation Outcome Reports: Update of the Utstein Resuscitation Registry Templates for Out-of-Hospital Cardiac Arrest: A Statement for Healthcare Professionals from a Task Force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian and New Zealand Council on Resuscitation, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Southern Africa, Resuscitation Council of Asia); and the American Heart Association Emergency Cardiovascular Care Committee and the Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Resuscitation. 2015;96:328-40.
17. Becker LB, Aufderheide TP, Geocadin RG, et al. Primary outcomes for resuscitation science studies: a consensus statement from the American Heart Association. Circulation. 2011;124(19):2158-77.
18. Hastie TJ, Tibshirani RJ. Generalized Additive Models. 1990.
19. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988;44(3):837-45.
20. Gue YX, Adatia K, Kanji R, et al. Out-of-hospital cardiac arrest: a systematic review of current risk scores to predict survival. Am Heart J. 2021;234:31-41.
21. Baldi E, Caputo ML, Savastano S, et al. An Utstein-based model score to predict survival to hospital admission: the UB-ROSC score. Int J Cardiol. 2020;308:84-9.
22. Liu N, Liu M, Chen X, et al. Development and validation of an interpretable prehospital return of spontaneous circulation (P-ROSC) score for patients with out-of-hospital cardiac arrest using machine learning: a retrospective study. EClinicalMedicine. 2022;48:101422.
23. Testa A, Versaci F, Biondi-Zoccai G. Individualised prognosis in out-of-hospital cardiac arrest: the case for P-ROSC in Asian people. EClinicalMedicine. 2022;48:101446.
24. Kupari P, Skrifvars M, Kuisma M. External validation of the ROSC after cardiac arrest (RACA) score in a physician-staffed emergency medical service system. Scand J Trauma Resusc Emerg Med. 2017;25(1):34.
25. Liu N, Ong MEH, Ho AFW, et al. Validation of the ROSC after cardiac arrest (RACA) score in Pan-Asian out-of-hospital cardiac arrest patients. Resuscitation. 2020;149:53-9.
26. Caputo ML, Baldi E, Savastano S, et al. Validation of the return of spontaneous circulation after cardiac arrest (RACA) score in two different national territories. Resuscitation. 2019;134:62-8.
27. Chiang WC, Hsieh MJ, Chu HL, et al. The effect of successful intubation on patient outcomes after out-of-hospital cardiac arrest in Taipei. Ann Emerg Med. 2018;71(3):387-96.
28. Paiva EF, Paxton JH, O’Neil BJ. The use of end-tidal carbon dioxide (ETCO) measurement to guide management of cardiac arrest: a systematic review. Resuscitation. 2018;123:1-7.
29. Wang CH, Lu TC, Tay J, et al. Association between trajectories of end-tidal carbon dioxide and return of spontaneous circulation among emergency department patients with out-of-hospital cardiac arrest. Resuscitation. 2022;177:28-37.
30. Lah K, Križmarić M, Grmec S. The dynamic pattern of end-tidal carbon dioxide during cardiopulmonary resuscitation: difference between asphyxial cardiac arrest and ventricular fibrillation/pulseless ventricular tachycardia cardiac arrest. Crit Care. 2011;15(1):R13.
31. Mertens M, King OC, van Putten M, et al. Can we learn from hidden mistakes? Self-fulfilling prophecy and responsible neuroprognostic innovation. J Med Ethics. 2021.
32. Brede JR, Skulberg AK, Rehn M, et al. REBOARREST, resuscitative endovascular balloon occlusion of the aorta in non-traumatic out-of-hospital cardiac arrest: a study protocol for a randomised, parallel group, clinical multicentre trial. Trials. 2021;22(1):511.