
{kind=link}
| Author | Affiliation |
|---|---|
| Siobhan Thomas-Smith, MD | University of Washington, Seattle Children’s Hospital, Department of Pediatrics, Division of Emergency Medicine, Seattle, Washington |
| Eileen J Klein, MD, MPH | University of Washington, Seattle Children’s Hospital, Department of Pediatrics, Division of Emergency Medicine, Seattle, Washington |
| Bonnie Strelitz, MPH | Center for Clinical and Translational Research, Seattle Children’s Research Institute, Seattle, Washington |
| Jennifer Jensen, MPH | Center for Clinical and Translational Research, Seattle Children’s Research Institute, Seattle, Washington |
| Elizabeth Parker, PhD | Center for Clinical and Translational Research, Seattle Children’s Research Institute, Seattle, Washington |
| Laura Richardson, MD, MPH | University of Washington School of Medicine, Department of Pediatrics, Division of Adolescent Medicine, Seattle, Washington |
| Carolyn A McCarty, PhD | University of Washington School of Medicine, Department of Pediatrics, Division of Adolescent Medicine, Seattle, Washington |
| Taraneh Shafii, MD, MPH | University of Washington School of Medicine, Department of Pediatrics, Division of Adolescent Medicine, Seattle, Washington |
Introduction
Materials and methods
Results
Discussion
Limitations
Conclusion
ABSTRACT
Introduction
In this study we aimed to assess the impact of an electronic health assessment with individualized feedback for risk behaviors in adolescents seeking care in a pediatric emergency department (ED).
Methods
We conducted a randomized control trial using a tablet-based screening program with a study population of adolescents in a busy pediatric ED. The intervention group received the screening program with individualized feedback. The control group received the screening program without feedback. All participants received one-day and three-month follow-up surveys to assess behaviors and attitudes toward health behaviors.
Results
A total of 296 subjects were enrolled and randomized. There was no difference in changes in risky behaviors between the control and experimental groups. A higher proportion of participants in the intervention groups reported that the screener changed the way they thought about their health at one-day follow-up (27.0%, 36/133) compared to the control group (15.5%, 20/129, P = .02).
Conclusion
This study successfully tested a multivariable electronic health screener in a real-world setting of a busy pediatric ED. The tool did not significantly change risky health behaviors in the adolescent population screened. However, our finding that the intervention changed adolescents’ perceptions of their health opens a door to the continued development of electronic interventions to screen for and target risk behaviors in adolescents in the ED setting.
INTRODUCTION
Nearly six million 15–18-year-olds are evaluated in an emergency department (ED) in the United States annually,1 and over 8% of 15–17-year-olds rely on the E D for outpatient healthcare visits.2 Adolescents who rely on the ED for healthcare have been found to have higher rates of risk behaviors and mental health needs compared to their peers2-7 and may miss health prevention screening typically completed during primary care visits.
Emergency clinicians recognize the importance and opportunity for screening health risk behaviors in adolescents such as alcohol and drug use and sexual activity. However, existing barriers in the ED setting limit the ability to screen and implement interventions.7,11 The primary barriers identified include limited time to build the rapport needed to ask sensitive health questions; lack of training in the use of screening tools; concerns that screening may detract from addressing the patient’s chief complaint; perception that screening is not the responsibility of the emergency clinician; and inadequate resources to address the problems that are identified.7-10
The development of electronic survey technology offers opportunities to efficiently screen adolescents for high-risk behaviors rather than relying on clinician time. Adolescents indicate that they prefer electronic screening over in-person interviews 9,13-16. Electronic screening also offers the opportunity to build in targeted interventions in an individualized manner using internal algorithms. Existing randomized controlled trials of risk-behavior, computer-based interventions with personalized feedback for adolescents in the ED have thus far targeted a singular specific risk behavior as opposed to screening for a range of behaviors. Several of these singular intervention studies have shown promise in reducing risk such as adolescent dating violence17,18 and alcohol abuse.18-20 While reducing any risk behavior is desirable, risk behaviors commonly co-occur;22-24 so, screening for only one risk behavior may be insufficient.
“Check Yourself” is an electronic screening intervention designed to identify and reduce multiple potentially co-existing risky behaviors as outlined by the Bright Futures guidelines,25 including alcohol and drug use, depression, sexual activity, and unsafe driving practices. “Check Yourself” also provides electronic feedback to adolescents about their health behaviors, peer behavioral norms, and tips to reduce risk.26 In three studies in primary care, the intervention was shown to be associated with increased delivery of risk-behavior counseling, and two of the three studies showed short-term (three-month) reductions in reported risk behaviors among adolescents, while one did not show significant reductions in risk compared to controls although both groups demonstrated risk reductions 27,28.
This randomized controlled trial evaluates the effectiveness of “Check Yourself” in reducing risk behaviors in a population of teens presenting for care in the pediatric ED. We hypothesized the intervention would decrease risky behaviors in adolescents at three-month follow-up compared to usual care.
MATERIALS AND METHODS
Study Design
This study was a randomized controlled trial conducted at a pediatric ED between March 2017–December 2018. The ED is part of an urban, tertiary, free-standing children’s hospital that serves a multi-state region with an estimated 50,000 pediatric patients overall and 8,000 adolescent patient visits per year. The study was approved by a hospital institutional review board and was registered in clinicalstrials.gov (Identifier: NCT03304574).
Population
Adolescent patients (aged 13–18 years) who presented to the ED for care, spoke and read English, and who had an email address or cell phone were eligible for study participation. Exclusion criteria were inability to complete screening due to intellectual disability; acute cognitive impairment due to injury or intoxication; administration of intravenous sedation or pain medications; mental health concern as primary reason for ED visit; or ED visit resulting in hospital admission. Individuals who were admitted to the hospital were excluded from the study due to the potential confounding factors of severity of illness, length of hospital stay, and inpatient, behavioral risk-factor screening on the potential for impacting behavioral change.
Population Health Research Capsule
What do we already know about this issue?
Computer-based interventions for adolescents in the ED can reduce risk for individual behaviors. However, risky behaviors commonly co-occur.
What was the research question?
Can a multi-behavior focused electronic health assessment with personal feedback decrease risk in adolescents seeking care in the ED?
What was the major finding of the study?
The assessment tool with personal feedback did not decrease risky behaviors, but the tool did change perspectives on health.
How does this improve population health?
Visits to the ED are an opportunity for adolescent risk-behavior screening. More work is needed to develop tools that encourage behavior change.
The Intervention
All intervention youth completed an electronic health assessment tool with integrated personalized feedback. The tool, “Check Yourself,” was originally designed for use prior to adolescent well-care visits in primary care settings. It takes about 15 minutes to complete and includes recommended screening for key health behaviors based on the Bright Futures guidelines25 (eg, alcohol and drug use, depression, sexual activity, driving safety, helmet use, physical activity, and nutrition). The tool provides integrated, individualized feedback based on motivational strategies such as normative feedback (comparison to peer behaviors and health guidelines); information regarding potential consequences of behaviors; and practical tips to change behavior.
At the completion of the feedback component of the tool, adolescents were given the option to receive additional online informational resources by email. In two of the three studies conducted in a primary care setting, the tool has been well received by adolescents and healthcare clinicians; and has shown to be associated with short-term (three-month) reductions in reported risk behaviors among adolescents.26,27 In the primary care studies, clinicians also received a one-page printed summary of adolescent-reported risk behaviors alerting the clinician to areas of high and moderate risk to encourage in-clinic counseling. Due to the fast-paced workflow in the ED, results of the risk screening were not provided to the emergency clinician. Instead, the adolescent patient only received integrated feedback with the tool.
Control Group
The control group received electronic screening only using a similar electronic screening interface. Control youth did not receive any individualized feedback.
Procedures
Prior to study enrollment, a simple randomization sequence was prepared by a statistician with no clinical involvement in the study with 300 potential allocations per arm. Once enrollment opened, clinical research coordinators (RC) prospectively identified adolescents during their ED visit and invited the patients to participate in the study. After verifying eligibility, adolescents <18 years provided assent and their caregivers gave consent. Adolescents who were 18 years old consented for themselves. After obtaining consent, RCs then used the REDCap (Research Eectronic Data Capture) computer randomization module to allocate participants to the control or intervention arm of the study. The RCs were present in the ED to enroll subjects seven days a week from 1 pm – 11 pm.
To ensure privacy while adolescents were using the computer tablets, caregivers were instructed not to view the tablet or participate in the screening questions. The RCs instructed adolescents not to discuss or share their responses with caregivers. As a safety measure, a flagging system was enacted to promptly notify the ED clinician (at baseline) or study clinicians (at follow-up) when an adolescent endorsed suicidality on the depression screen, regardless of study arm assignment. At baseline, ED procedures for suicidal patients included an evaluation by the ED attending who determined need for further evaluation. If further evaluation was deemed necessary, a mental health professional assessed the participant while in the ED and prior to discharge. For follow-up surveys, study clinicians called participants and conducted a phone interview to assess safety and ensure appropriate follow-up care. This protocol was implemented in the same manner across study arms.
All participants (intervention and control) were asked to complete online follow-up surveys at one day and three months after their initial ED visit. Follow-up periods of one day and three months were chosen due to similar follow-up periods with previous trials of the Check Yourself tool. Online follow-up surveys were collected using REDCap. (REDCap at the University of Washington Institute of Translational Health Sciences (ITHS) is supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number UL1 TR002319.) Participants were invited and reminded to complete the survey via short text message notifications, sent by an automated text messaging service (Twilio Inc, San Francisco, CA). The one-day follow-up survey asked adolescents whether the screening and feedback tool had changed the way they thought about their health. The three-month follow-up survey included a reassessment of the same risk behaviors assessed at baseline. Participants received a $10 gift card for each completed survey (up to $30 total).
Statistical Analysis
We used data on brief intervention effects with adolescents from the existing literature (Ozer 2005; Patrick 2001; Werch 2011) to conduct power calculations with PASS 11 (NCSS Statistical Software, Kaysville, UT), assuming two-sided statistical tests and P = 0.05. Based on inequality tests for repeated measures designs across means with a within-subject correlation (rho) = 0.5, a sample size of 150 per arm achieves >0.90 power to detect a difference in mean change of one point in risk-behavior summary.
Measures
Overall Risk Score
We calculated an overall risk score based on 13 risk behaviors screened for by the electronic tool including risks ranging from sleep behaviors and exercise to driving under the influence and inconsistent condom use. Ratings for risk behaviors were determined a priori and are consistent with prior studies of this tool.27 We defined high-risk variables as those causing imminent harm such as driving under the influence and were assigned a risk score of 2. Moderate risk variables defined as those that impair health over time but not associated with risk for short-term morbidity or mortality, such as lack of exercise, were assigned a risk score of 1.
Individual Behaviors
Depression
We used the Patient Health Questionnaire 2-item to assess for depressive symptoms, using the questions: “Over the last two weeks how often have you been bothered by having little interest or pleasure in doing things?” and “Over the last two weeks how often have you felt down, depressed or hopeless?”32
Substance Use
Variables for substance use included marijuana and alcohol frequency of use over the prior 30 days. Alcohol frequency was calculated by number of days and number of drinks per day. (One drink = one can/bottle of beer, one shot of liquor, one glass of wine).
Sexual Behavior
Sexual behavior risk was a composite variable of frequency of condom and/or birth control use with sex (Table 1).
Table 1Risk behavior change at baseline and three months for control and intervention groups.
| Control Group n (%) | Intervention Group n (%) | P-value | |||
|---|---|---|---|---|---|
|
|
|||||
| Baseline | At 3 mos follow | Baseline | At 3 mos follow | ||
| N = 147 | N = 105 | N = 149 | N = 104 | ||
| Nutrition | |||||
| Low fruit/vegetable intake 0–3/day | 113 (76.9) | 69 (65.7) | 119 (80.0) | 81 (77.9) | .12 |
| High sugary drinks >2/ day | 59 (40.1) | 46 (43.8) | 40 (26.8) | 28 (29.6) | .057 |
| Activity | |||||
| Low sleep time <8 hours/night | 81 (55.1) | 66 (62.8) | 61 (40.9) | 42 (40.4) | .0351 |
| Low physical activity 0–3 days/week | 55 (37.4) | 45 (42.8) | 41 (27.5) | 28 (26.9) | .72 |
| Safety | |||||
| Inconsistent seatbelt use | 28 (19.0) | 16 (15.2) | 21 (14.1) | 14 (13.5) | .43 |
| Inconsistent bike helmet use | 89 (60.5) | 52 (49.5) | 79 (53.0) | 38 (36.5) | .11 |
| Ever drives drunk or high | 4 (2.7) | 2 (1.9) | 2 (1.3) | 2 (1.9) | NA2 |
| Ever texts while driving | 22 (15.0) | 16 (15.2) | 19 (12.8) | 18 (17.3) | .18 |
| Drugs and Alcohol | |||||
| High alcohol use | 28 (19.0) | 14 (13.3) | 19 (12.8) | 10 (9.6) | .41 |
| High marijuana / other drug use | 33 (22.4) | 20 (19.0) | 22 (14.8) | 13 (12.5) | .87 |
| Any tobacco Use | 14 (9.5) | 12 (11.4) | 10 (6.7) | 7 (6.7) | .23 |
| Sexual behavior | |||||
| Inconsistent birth control/ condom use | 23 (15.6) | 14 (13.3) | 19 (12.8) | 6 (5.8) | .0461 |
| Depression | |||||
| High PHQ-2 score >=3 | 49 (33.3) | 35 (33.3) | 43 (28.8) | 31 (29.8) | .84 |
1Statistical significance set at P<.05.
2NA – statistical tests not performed if baseline data for intervention and control group n<10
PHQ-2, Patient Health Questionnaire 2-item.
Perception of Screener
At one-day post visit follow-up participants were asked if the screener changed the way they thought about their health. We included this variable to further assess the perceived impact of the screening and intervention tool in the ED.
Data Analysis
R version 3.6.3 (R Foundation for Statistical Computing, Vienna, Austria) was used for data analysis. We calculated means and standard deviations and conducted bivariate analyses to examine demographic differences (age, race, and gender identity) between the control and intervention groups. Chi-square tests were used for categorical variables and a t-test for continuous variables. The individual risk-behavior variables were constructed, and percentages of risk/no risk for each variable were calculated by treatment group and time period (baseline or three months). We used linear regression to assess the effects of the intervention on risk behaviors from baseline to three-month follow-up.
We conducted exploratory analyses to assess the intervention effects on specific risk behaviors included in the composite risk variable, such as substance use and inconsistent condom use. In addition to the main outcome measure, we examined the impact of the intervention on individual behaviors. These are behaviors that were deemed to be more acutely impactful on morbidity and mortality in this age group. Definitions for how risk was defined for each of these individual variables is provided below. We used binomial logistic regression for categorical variables and linear regression continuous variables. The control group was the reference group for all statistical models with age, gender identity, and baseline risk included as covariates.
RESULTS
A total of 412 of 493 participants approached were determined eligible for the study. Of those eligible, 296 joined the study, ultimately yielding an acceptance rate of 71.4%. The sample was comprised of 147 adolescents in the control arm and 149 in the intervention arm (Figure 1). The retention rate was 89.1% (262/294) at the one-day follow-up and 71.1% (209/262) at three-month follow-up. The sample consisted of 53% females with a mean age of 15.2 years. Of note, there was a difference in age between the groups (t = 2.44, P=.02) with the control group being significantly older (mean = 15.4 years) than the intervention group (mean =15.0 years) (Table 2).
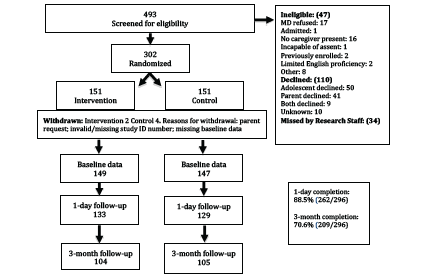
Table 2Demographic characteristics of study population.
| Control | Intervention | Total | |
|---|---|---|---|
|
|
|||
| N = 1451 | N = 149 | N = 294 | |
| Age, mean (SD) | 15.4 (1.6) | 15.0 (1.5)2 | 15.2 (1.6) |
| Gender, n (%) | |||
| Female | 75 (51.7) | 81 (54.4) | 156 (53.1) |
| Male | 70 (48.3) | 67 (44.9) | 137 (46.6) |
| Other | 0 | 1 (0.7) | 1 (0.3) |
| Race/Ethnicity, n (%) | |||
| White | 79 (54.5) | 90 (60.4) | 169 (57.6) |
| Multiracial/other | 32 (22.1) | 27 (18.1) | 59 (20.1) |
| Black | 16 (11.0) | 10 (6.7) | 26 (8.8) |
| Hispanic | 13 (9.0) | 7 (4.7) | 20 (6.8) |
| Asian | 3 (2.1) | 10 (6.7) | 13 (4.4) |
| Hawaiian / Pacific Islander | 2 (1.4) | 4 (2.7) | 6 (2.0) |
| Native American | 0 (0.0) | 1 (0.7) | 1 (0.3) |
1N = 147 with 2 participants missing demographic data.
2P<0.02.
Overall Risk Score
Prevalence of individual risk behaviors used to create the overall risk variable are presented in Table 1. The overall risk score mean at baseline was 5.87 (SD = 3.66) in the control group and 4.79 (SD = 3.66) in the intervention group. At three-month follow-up the overall mean risk score was 5.96 (SD = 3.43) for the control group and 4.42 (SD = 3.41) for the intervention group. Controlling for age, gender, and baseline risk score, we found no significant difference in reduction of risk for the intervention group compared to the control.
Individual Risk Behaviors
In an exploratory analysis of individual risk behaviors, there were no differences found between control and intervention groups at three-month follow-up for depression, marijuana use, alcohol use, or sexual behavior risk (Table 1).
Perception of Screener
A higher proportion of participants in the intervention groups reported that the screener changed the way they thought about their health at one-day follow-up (27.0%, 36/133) compared to the control group (15.5%, 20/129), controlling for age and gender (odds ratio 2.12; 95% confidence interval 1.14 – 4.03; P =.02).
DISCUSSION
This randomized clinical trial tested an electronic health assessment with individualized feedback for risk behaviors in adolescents seeking care in a pediatric ED. This study is unique as it was a large, randomized trial of a brief, multi-risk eHealth intervention with individualized feedback for adolescents in the ED. Although we found no difference in reduction of overall risk score between intervention and control groups at three months, participants reported the intervention changed the way they thought about their health.
The “Check Yourself” tool was first tested in primary care settings where primary care physicians were provided a print-out of their patient’s risk behaviors to facilitate discussion of preventive health at the visit.27 The setting for our study was a busy, fast-paced ED where clinicians focused on addressing the chief complaint and not on discussing preventive health. The emergency clinicians were not provided a print-out of risk behaviors nor were they expected to address health prevention topics; thus, this study in effect tested the brief eHealth feedback as a stand-alone intervention.
To assess for the intervention’s impact on risk behaviors that may be more commonly encountered in the ED, we performed an exploratory analysis on the outcomes of risk for marijuana use, alcohol use, depression, and risky sexual behavior. These risk behaviors were not decreased in the intervention group compared to the control group at three-month follow-up. There was a significant difference between groups at one-day follow-up with more intervention participants reporting that the “Check Yourself” tool impacted the way they thought about their health than those in control group, indicating a perceived attitudinal shift that merits further study.
Most risk behavior intervention studies in EDs target a single risk behavior,7 whereas the intervention in this study targeted 13 health behaviors. This may have diffused the impact on any one behavior affecting health. In addition, adolescents in the ED may be preoccupied by their reason for seeking care and less invested in learning about risks that are secondary to their presenting concerns. However, the literature supports that adolescents are open to risk-behavior screening in the ED regardless of their chief complaint. Studies have found acceptability for both specific risk behaviors such as substance abuse;15 pregnancy prevention;33 sexually transmitted infection risk;34-36 depression;37 suicidality;38 and for comprehensive screening across a battery of five risk behaviors (substance use, violence, depression, human trafficking, and access to firearms).39
Risk behavior screening in the ED is an important tool for adolescent health as it can reach a population that does not frequently access preventive healthcare. Such screening has increased the identification of substance abuse, post-traumatic stress, depression, and suicidality.40-43
Similar to our intervention, several studies have included brief, targeted interventions for behavioral change specifically for adolescent dating violence17-18 and alcohol abuse.18-20 Unlike these studies, however, our intervention assessed and provided feedback on a wide variety of behavioral risk factors, rather than more streamlined singular behaviors or areas as targets. As the screening was broader, the intervention itself required brevity to fit the time constraints of an ED visit. The difference in outcomes of our electronic screening and intervention tool compared to more focused interventions suggests that the use of multi-variable screening and feedback may not be as successful of an intervention on youth behaviors as targeted screening and feedback focusing on one achievable goal.
LIMITATIONS
This study has several limitations. The intervention targeted health behaviors with both long-term implications and those with more immediate health consequences. Overall, our study population had low prevalence of risky behaviors compared to the general population screened in the national Youth Risk Behavioral Surveillance System (YRBS) with the exception of depression, which was similar to the YRBS.21 These prevalence differences may limit the generalizability of the study. Youth in the ED may have been more concerned about the reason for their acute visit rather than those behaviors addressed in the intervention. Unlike the primary care trial of the “Check Yourself” tool, this intervention did not include discussion with a healthcare clinician, and thus may not have had as much impact. While there was a significant finding of the intervention impact in how adolescents perceived their health, there were no follow-up questions to understand the specifics on how their beliefs changed.
CONCLUSION
This study successfully tested a multi-variable electronic health screener in a real-world setting of a busy pediatric ED. We were able to implement screening and feedback for health behaviors into typical ED workflow without adding to the workload of clinicians. The “Check Yourself” tool did not significantly change health behavior risks in the adolescent population screened. However, based on our one-day follow-up, our intervention did show an impact on how adolescents perceive their health, opening a door to the continued development of electronic interventions to screen for and target risk behaviors in adolescents in the ED setting. Future studies should focus interventions designed for specific risk behaviors with more depth that could result in more immediate healthy changes and health consequences.
Footnotes
Section Editor: Tony Zitek, MD
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Siobhan Thomas-Smith, MD, University of Washington, Department of Pediatrics, 4800 Sand Point Way NE, Seattle, Washington 98105. Email: siobhanthomassmith@gmail.com. 11 / 2022; 23:931 – 938
Submission history: Revision received December 21, 2021; Submitted June 30, 2022; Accepted July 19, 2022
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. No author has professional or financial relationships with any companies that are relevant to this study. There are no conflicts of interest or sources of funding to declare.
REFERENCES
1. McDermott KW, Stocks C, Freeman WJ. Overview of Pediatric Emergency Department Visits, 2015. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. 2018.
2. Schlichting LE, Rogers ML, Gjelsvik A, et al. Pediatric emergency department utilization and reliance by insurance coverage in the United States. Acad Emerg Med. 2017;24:1483-90.
3. Winkelman TNA, Genao I, Wildeman C, et al. Emergency department and hospital use among adolescents with justice system involvement. Pediatrics. 2017;140(5):1-9.
4. Aalsma MC, Anderson VR, Schwartz JD, et al. Preventive care utilization among justice-involved and non-justice involved youth. Pediatrics. 2017;140(5):1-15.
5. Bonar EE, Walthon MA, Caldwell MT, et al. Sexually transmitted infection history among adolescents presenting to the emergency department. J Emerg Med. 2015;49(5):613-22.
6. Chandler I, Rosenthal L, Carroll-Scott A, et al. Adolescents who visit the emergency department are more likely to make unhealthy dietary choices: an opportunity for behavioral intervention. J Health Care Poor Underserved. 2015;26(3):701-11.
7. Chun TH, Duffy SJ, Linakis JG. Emergency department screening for adolescent mental health disorders: the who, what, when, where, why and how it could and should be done. Clin Pediatr Emerg Med. 2013;14(1):3-11.
8. Habis A, Tall L, Smith J, et al. Pediatric emergency medicine physicians’ current practices and beliefs regarding mental health screening. Pediatr Emerg Care. 2007;23(6):387-93.
9. Miller MK, Mollen C, Behr K, et al. Development of a novel computerized clinical decision support system to improve adolescent sexual health care provision. Acad Emerg Med. 2019;26(4):420-33.
10. Shafii T, Rivara FP, Wang P, et al. Screening adolescent patients admitted to the trauma service for high-risk behaviors: who is responsible?. J Trauma. 2009;67(6):1288-92.
11. Irwin CE, Adams SH, Park MJ, et al. Preventive care for adolescents: few get visits and fewer get services. Pediatrics. 2009;123(4):e565-72.
12. Miller MK, Champassak S, Goggin K, et al. Brief behavioral intervention to improved adolescent sexual health: a feasibility study in the emergency department. Pediatr Emerg Care. 2016;32(1):1-7.
13. Jasik CB, Berna M, Martin M, et al. Teen preferences for clinic-based behavior screens: who, where, when, how?. J Adolesc Health. 2016;59(6):722-4.
14. Ranney ML, Choo EK, Wang Y, et al. Emergency department patient’s preferences for technology-based behavioral interventions. Ann Emerg Med. 2012;60(2):218-27.
15. Vaca F, Winn D, Anderson C, et al. Feasibility of emergency department bilingual computerized alcohol screening, brief intervention, and referral to treatment. Subst Abus. 2010;31:264-9.
16. Stevens J, Kelleher KJ, Gardner W, et al. Trial of computerized screening for adolescent behavioral concerns. Pediatrics. 2008;121(6):1099-105.
17. Cunningham RM, Whiteside LK, Chermack ST, et al. Dating violence: outcomes following a brief motivational interviewing intervention among at-risk adolescents in an urban emergency department. Acad Emerg Med. 2013;20(6):562-9.
18. Walton MA, Chermack ST, Shope JT, et al. Effects of a brief intervention for reducing violence and alcohol misuse among adolescents: a randomized controlled trial. JAMA. 2010;304(5):527-35.
19. Walton MA, Chermack ST, Blow FC, et al. Components of brief alcohol interventions for youth in the emergency department. Subst Abus. 2015;36(3):339-49.
20. Suffoletto B, Callaway C, Kristan J, et al. Text-message-based drinking assessments and brief interventions for young adults discharged from the emergency department. Alcohol Clin Exp Res. 2012;36(3):552-60.
21. Kann L, McManus T, Harris WA, et al. Youth Risk Behavior Surveillance – United States, 2017. MMWR Surveill Summ. 2018;67(8):1-114.
22. Riskind RG, Tornello SL, Younger BC, et al. Sexual identity, partner gender, and sexual health among adolescent girls in the United States. Am J Public Health. 2014;104(10):1957-63.
23. Sterrett EM, Dymnicki AB, Henry D, et al. Predictors of co-occurring risk behavior trajectories among economically disadvantaged African-American youth: contextual and individual factors. J Adolesc Health. 2014;55(3):380-7.
24. De Winter AF, Visser L, Verhulst FC, et al. Longitudinal patterns and predictors of multiple health risk behaviors among adolescents: The TRAILS study. Prev Med. 2016;84:76-82.
25. 2017 Recommendations for Preventive Pediatric Health Care. Pediatrics. 2017;139(4):e20170254.
26. Zieve GG, Richardson LP, Katzman K, et al. Adolescents’ perspectives on personalized e-feedback in the context of health risk behavior screening for primary care: qualitative study. J Med Internet Res. 2017;19(7):1-11.
27. Richardson LP, Zhou C, Gersh E, et al. Effect of electronic screening with personalized feedback on adolescent health risk behaviors in a primary care setting; a randomized clinical trial. JAMA Netw Open. 2019;2(5):e193581.
28. McCarty CA, Parker E, Zhou C, et al. Electronic screening, feedback, and clinician training in adolescent primary care: a stepped-wedge cluster randomized trial. J Adolesc Health. 2022;70(2):234-40.
29. Ozer EM, Adams SH, Lustig JL, et al. Increasing the screening and counseling of adolescents for risky health behaviors: a primary care intervention. Pediatrics. 2005;115(4):960-8.
30. Patrick K, Sallis JF, Prochaska JJ, et al. A multicomponent program for nutrition and physical activity change in primary care: PACE+ for adolescents. Arch Pediatr Adolesc Med. 2001;155(8):940-6.
31. Werch CE, Bian H, Carlson JM, et al. Brief integrative multiple behavior intervention effects and mediators for adolescents. J Behav Med. 2011;34(1):3-12.
32. Richardson LP, Rockhill C, Russo JE, et al. Evaluation of the PHQ-2 as a brief screen for detecting major depression among adolescents. Pediatrics. 2010;125(5):e1097-e1103.
33. Solomon M, Badolato GM, Chernick LS, et al. Examining the role of the pediatric emergency department in reducing unintended adolescent pregnancy. J Pediatr. 2017;189:196-200.
34. Ahmad FA, Jeffe DB, Plax K, et al. Characteristics of youth agreeing to electronic sexually transmitted infection risk assessment in the emergency department. Emerg Med J. 2018;35(1):46-51.
35. Goyal MK, Shea JA, Hayes K, et al. Development of a sexual health screening tool for adolescent emergency department patients. Acad Emerg Med. 2016;23(7):809-15.
36. Goyal MK, Teach SJ, Badolato GM, et al. Universal screening for sexually transmitted infections among asymptomatic adolescents in an urban emergency department: high acceptance but low prevalence. J Pediatr. 2016;171:128-32.
37. Ranney ML, Freeman JR, Connell G, et al. A depression prevention intervention for adolescents in the emergency department. J Adolesc Health. 2016;59(4):401-10.
38. Ballard ED, Bosk A, Snyder D, et al. Patients’ opinions about suicide screening in a pediatric emergency department. Pediatr Emerg Care. 2012;28(1):34-8.
39. Langerman SD, Badolato GM, Rucker A, et al. Acceptability of adolescent social and behavioral health screening in the emergency department. J Adolesc Health. 2019;65:543-8.
40. Boudreaux ED, Camargo CA, Arias SA, et al. Improving suicide risk screening and detection in the emergency department. Am J Preven Med. 2016;50(4):445-53.
41. Ballard ED, Cwik M, Van Eck K, et al. Identification of at-risk youth by suicide screening in a pediatric emergency department. Prev Sci. 2017;18:174-82.
42. Fein AJ, Pailler ME, Barg FK, et al. Feasibility and effects of a web-based adolescent psychiatric assessment administered by clinical staff in the pediatric emergency department. Arch Pediatr Adolesc Med. 2010;164(12):1112-7.
43. Spirito A, Bromberg JR, Casper C, et al. Reliability and validity of a two-question alcohol screen in the pediatric emergency department. Pediatrics. 2016;138(6):1-10.