
{kind=link}
| Author | Affiliation |
|---|---|
| Mengyao Ying, MD | Changxing People’s Hospital of China, Department of Emergency Medicine, Zhejiang Province, People’s Republic of China |
| Yuetun Zuo, MD | Changxing People’s Hospital of China, Department of Emergency Medicine, Zhejiang Province, People’s Republic of China |
Introduction
Materials and methods
Results
Discussion
Limitations
Conclusion
ABSTRACT
Introduction
Ketamine can be particularly helpful in situations where the clinician is not able to administer opioids and require an alternate analgesic, such as for patients who are already on high-dose opioids, have a history of addiction, or for opioid-naïve children and adults. In this review, our goal was to obtain a comprehensive estimate of the efficacy and safety of low-dose ketamine (dose less than 0.5 milligrams per kilogram or equivalent) compared to opiates for the control of acute pain in the emergency setting.
Methods
We conducted systematic searches in PubMed Central, EMBASE, MEDLINE, the Cochrane Library, ScienceDirect, and Google Scholar from inception until November 2021. We used the Cochrane risk-of-bias tool to assess the quality of included studies.
Results
We carried out a meta-analysis with a random-effects model and reported pooled standardized mean difference (SMD) and risk ratio (RR) with 95% confidence intervals depending on the type of the outcome. We analyzed a total of 15 studies with 1,613 participants. Half of them had high risk of bias and were conducted in the United States of America. The pooled SMD for pain score was −0.12 (95% CI −0.50–0.25; I2=68.8%) within 15 minutes, −0.45 (95% CI −0.84–−0.07; I2=83.3%) within 30 minutes, −0.05 (95% CI −0.41–0.31; I2=86.9%) within 45 minutes, −0.07 (95% CI −0.41–0.26; I2=82%) within 60 minutes, and after 60 minutes the pooled SMD was 0.17 (95% CI −0.07–0.42; I2=64.8%). The pooled RR for need of rescue analgesics was 1.35 (95% CI 0.73–2.50; I2=82.2%). The pooled RRs were as follows: 1.18 (95% CI 0.76–1.84; I2=28.3%) for gastrointestinal side effects; 1.41 (95% CI 0.96–2.06; I2=29.7%) for neurological side effects; 2.83 (95% CI 0.98–8.18; I2=47%) for psychological side effects; and 0.58 (95% CI 0.23–1.48; I2=36.1%) for cardiopulmonary side effects.
Conclusion
Low-dose ketamine might have higher or equivalent efficacy and safety when compared to opioids for managing acute pain among patients presenting to the emergency setting. However, further studies are required to establish conclusive evidence, owing to the heterogeneity and poor quality of existing studies.
INTRODUCTION
Acute pain is responsible for more than half of the visits to the emergency department (ED).1,2 Therefore, management of acute pain is an essential aspect of patient satisfaction and care. Currently, opioids are the most common group of analgesics used for the management of acute pain.3 However, given the complications associated with use of opioids, many patients would benefit from an opioid alternative for an effective and safer control of pain. In addition, certain categories of patients, such as opioid-naïve children and adults, the elderly, chronic users of opioid medications, patients with a history of opioid use disorder, and those using drugs for opioid use disorders or alcohol dependence, would also benefit from an effective alternative to opioids.4,5
Ketamine is a N-methyl-D-aspartate (NMDA) receptor antagonist drug with anaesthetic and analgesic properties.6 While traditionally it was used as an anaesthetic, it was replaced by the newer class of anaesthetics with better efficacy and minimal side effects. Over the past few years, ketamine has been used in the emergency setting for induction before intubation and procedural sedations, given its dissociative properties that allow preservation of the airway reflexes and hemodynamic stability properties.7
At the lower sub-dissociative doses (less than 0.5 milligrams per kilogram [mg/kg] intravenous [IV] doses), ketamine has been shown to have better analgesic property than opiates for the acute and chronic pain.[8]. Although, the use of ketamine for managing acute pain is a relatively novel concept, it has certain unique features that could prove advantageous in improving patient outcomes, particularly for the group of people mentioned above. Several studies have examined the role of ketamine compared to opioids for the management of acute pain.9-11 Although few reviews have attempted to summarized the findings of these reports, they have included a very limited number of studies and provided inconclusive evidence on the efficacy and safety of ketamine for acute pain management.12,13 Our main goal in this comprehensive systematic review and meta-analysis was to evaluate the role of low-dose ketamine compared to opiates for the management of acute pain in the emergency setting.
MATERIALS AND METHODS
Design
The protocol of the study was registered in PROSPERO, registration number CRD42021289270. In this systematic review, we used the “Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement 2020” for reporting meta-analyses.14
Eligibility Criteria
Study Design
We included studies with any of the following study designs: parallel-arm individual or cluster randomized controlled trials (RCT). For cross-over trials, only the first half of the trial (before crossing over) were included. We included only published, full-text studies or abstracts, while excluding unpublished data or gray literature.
Participants
We included studies conducted in patients reporting to the emergency setting or ED with acute pain were included to form two groups (ketamine and control groups), irrespective of the cause of pain. We excluded studies conducted among postoperative patients.
Intervention and Comparison Groups
Studies using the IV low-dose ketamine (dose less than 0.5 mg/kg or equivalent) for the management of acute pain as intervention were included. The comparison group used opioids such as morphine, fentanyl, etc, or were placebo-controlled trials or standard care.
Population Health Research Capsule
What do we already know about this issue?
At the lower sub-dissociative doses (< 0.5 mg/kg IV dose), ketamine has been shown to have better analgesic property than opiates for the acute and chronic pain.
What was the research question?
What is the efficacy of low-dose ketamine for the control of acute pain in emergency setting?
What was the major finding of the study?
The pooled standard mean difference of ketamine for pain score was −0.45 (95%CI: −0.84 to −0.07; p<0.001) within 30 minutes.
How does this improve population health?
The study provides important information to clinicians and emergency physicians on the use of low-dose ketamine for management of acute pain in emergency setting.
Outcome Measures
Our outcome measures were pain score, the need for rescue analgesic medication, and adverse effects (gastrointestinal, neurological, psychological or cardiopulmonary side effects). Studies reporting either the pain score or need for rescue analgesic medication were included.
Search Strategy
We systematically searched electronic databases, including PubMed Central, EMBASE, MEDLINE, and the Cochrane Library and search engines such as ScienceDirect and Google Scholar, for eligible studies using medical subject headings and free-text words. Individual search results were combined, and the final search was performed using appropriate Boolean operators (“OR” and “AND”) and narrowed down using the available filters on time period (from inception to October 2021), language (English language only), as summarized in the Supplementary Appendix.
Study Selection
We selected the relevant studies by screening the title, abstract, and keywords of the identified manuscripts. For the studies that met the eligibility criteria, we then reviewed and screened the full-text articles were. The eligibility criteria of the reviews were assessed. We included studies that met eligibility criteria with respect to design, participants, intervention, comparisons, and outcomes. All cases of disagreement were resolved by discussion.
Data Extraction
Data was manually extracted using a predefined structured data extraction form and included authors, title of study, year of publication, study period, study design, setting, country/region, total sample size, outcome assessment details, average age, and primary and secondary outcomes in each approach. The primary investigator was responsible for entering the data, and the secondary investigator double-checked for accuracy.
Risk-of-bias (Quality) Assessment
Quality of included studies was assessed by two independent investigators using the revised Cochrane risk-of-bias tool (RoB 2) for RCTs.15 We assessed risk of bias under the following domains:
Domain 1: Bias risk arising from the process of randomization
Domain 2: Bias risk due to deviation from the intended intervention
Domain 3: Bias risk arising due to missing data on outcomes
Domain 4: Bias risk in the measurement of outcome
Domain 5: Bias risk in the selection of reported result.
Based on the rating obtained from these domains, we classified the quality of evidence of each study as having “low bias risk,” “high bias risk,” and “some concerns.”
Statistical Analysis
We performed data analysis using STATA version 14.2. (StataCorp LLC, College Station, TX). For continuous data such as pain score and total analgesic requirement, we obtained mean, standard deviation, and total sample size for both groups. The pooled effect was calculated as standardized mean difference (SMD) with 95% confidence interval, as different scales were used by each of the studies for reporting pain scores. Since all the other outcomes were dichotomous, the number of events and participants in each group were entered to obtain the pooled effect estimate as a risk ratio (RR) with 95% CI. Visual representation of these pooled estimates was done by forest plot. We used the random-effects model with inverse variance method to calculate the weight of individual studies.16
Heterogeneity was evaluated by chi square of heterogeneity and the I2 statistic. A P-value less than 0.05 in chi square testing indicated significant heterogeneity, while we used the I2 value to quantify the heterogeneity using the following criteria: less than 25% = mild heterogeneity, 25–75% = moderate heterogeneity and >75% = substantial heterogeneity.16 We performed subgroup analysis and meta-regression to explore the source of heterogeneity using possible potential covariates such as dose of ketamine and comparison group. Publication bias was evaluated and visually represented using a funnel plot. We assessed the asymmetry of plot using Egger’s test. A P-value < 0.10 was considered as statistically significant publication bias.17
Quality of Evidence
The risk of bias and quality of evidence for included studies were independently assessed by two investigators using Grading of Recommendations Assessment, Development and Evaluation (GRADE) guidelines.16 The GRADE approach consists of five components: 1) risk of bias assessment; 2) indirectness; 3) imprecision; 4) inconsistency; and 5) publication bias.
Risk of bias assessment: Determined using the Cochrane risk-of-bias tool
Indirectness: Assessed in terms of population, intervention, comparison, or outcomes
Imprecision: Determined the precision of the estimate obtained, based on sample size and CI
Inconsistency: Assessed evidence of heterogeneity using the I2 statistic and chi square test of heterogeneity
Publication bias: Assessed using Egger’s test and a funnel plot.
Finally, we classified the quality of the included studies as “very low,” “low,” “moderate,” and “high” based on certainty of evidence.
RESULTS
Study Selection
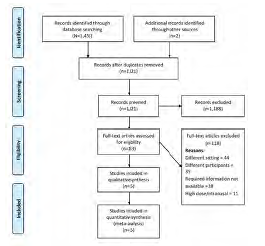
Figure 1 shows the PRISMA flowchart of the study selection process. During primary screening, 188 full-text studies were retrieved. Of them, 133 studies remained after removal of duplicates. An additional three articles were retrieved from the bibliography of the screened articles. Studies underwent secondary screening that resulted in a total of 15 studies with 1,613 participants, which satisfied the inclusion criteria and were included in the analysis.9-11,18-29
Study Characteristics
We have included only RCTs in our review. Most studies (8/15) were conducted in the United States of America (US), followed by Middle Eastern countries such as Iran and Saudi Arabia. The mean age of study participants in the intervention arm ranged from 29.1–77.3 years, while in the control arm it ranged from 29.6–77.1. The sample sizes among the included studies varied from 34–300. The IV dose of ketamine ranged from 0.1–0.5 mg/kg. Morphine was the most commonly used opioid in the comparison group (10 studies) followed by placebo (normal saline in five studies). Regarding quality assessment, at least half of the studies had higher risk of bias (seven studies), while the remaining studies evidenced some concerns as per the RoB 2 checklist (Table 1).
| Author and year | Country | Sample size | Study participants | Pain scale | Route of administration of ketamine | Dose of ketamine | Comparator group | Mean age | Risk of bias |
|---|---|---|---|---|---|---|---|---|---|
| Alshahrani 2021 | Saudi Arabia | I=138C=140 | Adults with sickle cell disease who presented with acute sickle vaso-occlusive crisis. | NRS | Intravenous | 0.3 mg/kg | Morphine | I=29.1C=29.6 | High |
| Beaudoin 2014 | USA | I=20C=20 | Patients 18–65 years old with acute moderate to severe pain and pain duration <7 days) who were deemed by their treating physician to require IV opioid | NRS | Intravenous | 0.3 mg/kg | Morphine | I=37.5C=32.5 | Some concerns |
| Carver 2019 | USA | I=45C=46 | Adult patients with three or more rib fractures admitted to a Level I trauma center | NRS | Intravenous | 2.5 μg/kg | Placebo | I=46C=50 | High |
| Esfahani 2021 | Iran | I=36C=37 | Patients referred to EDs due to isolated limb traumatic injuries | NRS | Intravenous | 0.1 mg/kg | Morphine | I=32.5C=33.4 | High |
| Etchison 2018 | USA | I=16C=18 | Adults 18–65 years of age with acute migraine at a single academic ED | NRS | Intravenous | 0.2 mg/kg | Placebo | I=38.5C=30.5 | Some concerns |
| Forouzan 2019 | Iran | I=68C=68 | Patients who had suffered kidney pain due to kidney stones referred to Ahvaz Imam Khomeini Hospital | NRS | Intravenous | 0.3 mg/kg | Morphine | NR | High |
| Galinski 2007 | France | I=33C=32 | Trauma patients with a severe acute pain defined as a VAS score of at least 60/100 were enrolled | VAS | Intravenous | 0.2 mg/kg | Placebo | I=35C=40 | Some concerns |
| Jahanian 2018 | Iran | I=78C=78 | Adult patients 18–65 years with upper or lower extremity long bone fractures caused by blunt trauma referring to our ED | VAS | Intravenous | 0.5 mg/kg | Morphine | I=35.8C=36.3 | High |
| Kugler 2019 | USA | I=30C=29 | Elderly patients (age, ≥65 years) with three or more rib fractures admitted to a Level I trauma center | NRS | Intravenous | 0.2 mg/kg | Placebo | I=75C=73 | High |
| Mahshidfar 2017 | Iran | I=150C=150 | Trauma patients aged 18–70 years with a musculoskeletal pain score of 5 or more on 11-point NRS who were referred to EDs | NRS | Intravenous | 0.2 mg/kg | Morphine | I=34.4C=34.1 | Some concerns |
| Majidinejad 2014 | Iran | I=63C=63 | Patients with fractures of long bones, referred to the emergency unit. | NRS | Intravenous | 0.5 mg/kg | Morphine | I=35.1C=53.6 | Some concerns |
| Miller 2015 | USA | I=24C=21 | Patients 18–59 years with acute abdominal, flank, low back, or extremity pain were enrolled | NRS | Intravenous | 0.3 mg/kg | Morphine | I=31C=29 | Some concerns |
| Motov 2015 | USA | I=45C=45 | ED patients 18–55 years and experiencing moderate to severe acute abdominal, flank, or musculoskeletal pain | NRS | Intravenous | 0.3 mg/kg | Morphine | I=35C=36 | Some concerns |
| Motov 2019 | USA | I=30C=30 | ED patients 18–55 years and experiencing moderate to severe acute abdominal, flank, or musculoskeletal pain | NRS | Intravenous | 0.3 mg/kg | Morphine | I=77.3C=77.1 | Some concerns |
| Sin 2017 | USA | I=30C=30 | Patients >18 years who presented to the ED with a chief complaint of acute pain with moderate to severe intensity | NRS | Intravenous | 0.3 mg/kg | Placebo | I=41C=48 | High |
I, Intervention (ketamine) group; C, control/comparator group; FPS, Faces Pain Scale; NR, not reported; NRS, Numerical Rating Scale; VAS, Visual Analog Scale; USA, United States of America; ED, emergency department.
Efficacy of Ketamine for Control of Acute Pain
Pain Score within 15 Minutes
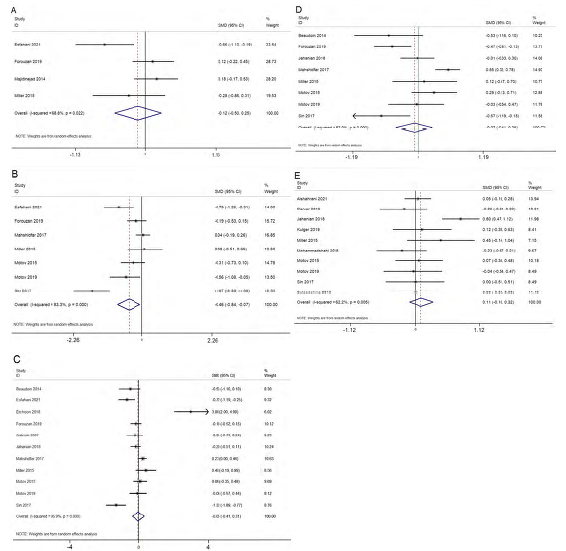
Four studies reported on the difference in pain score within 15 minutes. The pooled SMD was −0.12 (95% CI −0.50–0.25; I2=68.8%), indicating no significant difference between the ketamine and control groups in the control of pain within 15 minutes (Figure 2A). Analysis based on the dose of ketamine was not possible as each of the studies used different doses, making it difficult to provide a pooled estimate for each dose. Similarly, analysis based on the control group was not possible as all the studies used morphine in the control group. The quality of evidence was found to be low as per the GRADE approach.
Pain Score within 30 Minutes (15–29 minutes)
Seven studies reported on the difference in pain score within 30 minutes. The pooled SMD was −0.45 (95% CI −0.84–−0.07; I2=83.3%), indicating a significant decline in the pain score among the patients’ receiving ketamine when compared to the control arm within 30 minutes (Figure 2B). Sensitivity analysis did not affect the significant findings obtained in the primary analysis in terms of magnitude or direction of association because of small-study effects (Supplementary Figure 1). The most commonly used dose of ketamine (five studies) was 0.3 mg/kg and was associated with a significant difference in pain score (pooled SMD = −0.51, 95% CI −1.01–−0.01). Analysis based on the control group was not possible as all the studies (except Sin et al 2017) used morphine as control group. The quality of evidence was found to be low as per the GRADE approach.
Pain Score within 45 Minutes (30–44 minutes)
Eleven studies reported on the difference in pain score within 45 minutes. The pooled SMD was −0.05 (95% CI −0.41–0.31; I2=86.9%), indicating no significant difference in pain score between ketamine and the control group within 45 minutes (Figure 2C). Sensitivity analysis did not reveal any significant difference in the magnitude or direction of association because of small-study effects (Supplementary Figure 2). The funnel plot showed a symmetrical plot indicating the lack of publication bias (Supplementary Figure 3), and it was further confirmed by a non-significant Egger’s test (P=0.96). The quality of evidence was found to be low as per the GRADE approach.
Analysis based on the dose of ketamine did not show significant effect at any of the doses ranging from 0.1–0.5 mg/kg. Analysis based on the control group did not reveal a significant effect for ketamine when compared to morphine (pooled SMD = −0.11; 95% CI −0.3–0.13) or placebo (pooled SMD = 0.42, 95% CI −1.51–2.36). Univariable meta-regression revealed that none of these factors were responsible for the significant heterogeneity in the estimates. The quality of evidence was found to be low as per the GRADE approach.
Pain Score between 45–60 Minutes
Eight studies reported on the difference in pain score between 45–60 minutes. The pooled SMD was −0.07 (95% CI −0.41 to 0.26; I2=82%), indicating no significant difference in pain score between the ketamine and control groups between 45–60 minutes (Figure 2D). Sensitivity analysis did not reveal any significant difference in the magnitude or direction of association because of small-study effects (Supplementary Figure 4). Analysis based on the dose of ketamine did not show significant effect at any of the doses ranging from 0.1–0.5 mg/kg. Analysis based on the control group was not possible as all the studies (except Sin et al 2017) used morphine in the control group. The quality of evidence was found to be low as per the GRADE approach.
Pain Score after 60 Minutes
Eight studies reported on the difference in pain score after 60 minutes. The pooled SMD was 0.17 (95% CI −0.07–0.42; I2=64.8%), indicating no significant difference in pain score between the ketamine group and control group after 60 minutes (Figure 2E). Sensitivity analysis did not reveal any significant difference in the magnitude or direction of association because of small-study effects (Supplementary Figure 5). Analysis based on the dose of ketamine was not possible as each of the studies used a different dose, making it difficult to provide a pooled estimate for each dose. Analysis based on the control group did not reveal a significant effect for ketamine when compared to morphine (pooled SMD = 0.28, 95% CI 0.05–0.62) or placebo (pooled SMD = −0.05, 95% CI −0.32–0.22). The quality of evidence was found to be low as per the GRADE approach.
Need for Rescue Analgesic Medication
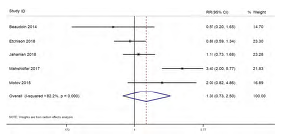
Five studies reported on the difference in need for rescue analgesic medication between the ketamine and control groups. The pooled RR was 1.35 (95% CI 0.73–2.50; I2=82.2%), indicating no significant difference in need for rescue analgesics between the ketamine and control groups (Figure 3). Sensitivity analysis did not reveal any significant difference in the magnitude or direction of association because of small-study effects (Supplementary Figure 6). Analysis based on the dose of ketamine did not show significant effect at any of the doses ranging from 0.1–0.5 mg/kg. Analysis based on the control group was not possible as all the studies (except Etchison et al 2018) used morphine in the control group. The quality of evidence was found to be low as per the GRADE approach.
Adverse Effects
Gastrointestinal Side Effects
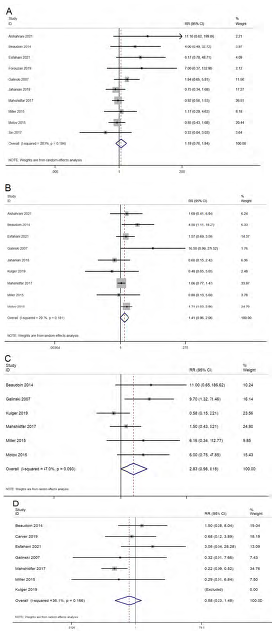
Ten studies reported on the difference in gastrointestinal side effects (nausea and vomiting) between the ketamine and control groups. The pooled RR was 1.18 (95% CI 0.76–1.84; I2=28.3%), indicating no significant difference in the gastrointestinal side effects between the ketamine and control groups (Figure 4A). Analysis based on the dose of ketamine did not show any difference in gastrointestinal side effects at any of the doses ranging from 0.1–0.5 mg/kg. Analysis based on the control group revealed no significant difference compared to any of the control group. The quality of evidence was found to be low as per the GRADE approach.
Neurological Side Effects
Ten studies reported on the difference in neurological side effects (dizziness, drowsiness, emergence phenomena, dysphoria/dissociation) between the ketamine and control groups. The pooled RR was 1.41 (95% CI 0.96–2.06; I2=29.7%), indicating no significant difference in the neurological side effects between the ketamine and control groups (Figure 4B). Analysis based on the dose of ketamine showed significantly higher risk of neurological side effects at a dose of 0.3 mg/kg (pooled RR=1.82, 95% CI 1.17–2.83), while it was not significant at a dose less than 0.3 mg/kg. Analysis based on the control group revealed no significant difference compared to any of the control group. The quality of evidence was found to be low as per the GRADE approach.
Psychological Side Effects
Six studies reported on the difference in psychological side effects (delirium, hallucinations, and mood changes) between the ketamine and control groups. The pooled RR was 2.83 (95% CI 0.98–8.18; I2=47%), indicating no significant difference in psychological side effects between the ketamine and control groups (Figure 4C). Subgroup analysis based on the route of administration, dose, or control group did not reveal any difference in terms of magnitude or direction of association. The quality of evidence was found to be low as per the GRADE approach.
Cardiopulmonary Side Effects
Seven studies reported on the difference in cardiopulmonary side effects (hypoxia, hypotension, and respiratory failure) between the ketamine and control groups. The pooled RR was 0.58 (95% CI 0.23–1.48; I2=36.1%), indicating no significant difference in cardiopulmonary side effects between the ketamine and control groups (Figure 4D). Subgroup analysis based on the route of administration, dose, or control group did not reveal any difference in terms of magnitude or direction of association. The quality of evidence was found to be low as per the GRADE approach.
DISCUSSION
Our aim in this systematic review was to obtain a comprehensive estimate of the efficacy and safety of low-dose ketamine for the control of acute pain among patients presenting to the ED. We found that ketamine causes a significant decline in the pain score within 30 minutes of infusion when compared to any control group. We also found that ketamine had maximum efficacy at a dosage of 0.3 mg/kg when administered through the IV route. However, primary evidence is limited on the dose-related analysis and conclusive evidence on dosage cannot be provided. Ketamine had better efficacy when compared to morphine and placebo. However, its effect was similar to morphine and placebo at other time intervals (>30 minutes). Previous reviews have also reported that ketamine had equivalent or higher efficacy in the pain score at short-term and long-term time intervals compared to opioids such as morphine or fentanyl.12,13,30 In addition, a review has also reported 0.3 mg/kg as the optimal dose of ketamine.13
Mechanism of action of ketamine involves binding to the spinal μ receptors and increasing the efficacy of the opioid-induced signalling.31 In addition, ketamine also functions as a NMDA receptor antagonist and acts preferentially post-synoptically, causing a reduction in hyperexcitability.32 Therefore, the blockage of NMDA by ketamine might further improve the opioid efficacy leading to opioid-sparing effect.
We also assessed risk of various adverse effects associated with ketamine for the management of acute pain in emergency settings. We found that ketamine was associated with a significantly higher risk of neurological side effects at a dose of 0.3 mg/kg when compared to the opioid group of drugs. Previous reviews have also warned against the neurological complications of ketamine, especially at higher doses. Ketamine prevents serious adverse effects of opioids and inhibits the chronic pain that develops due to opioid tolerance.33,34 Ketamine inhibits nociception through the high affinity and selective interaction with the NMDA receptor.33,34 At the full-anaesthetic dose, ketamine activates different types of opioid receptors, such as κ, μ, and σ opioid receptors, with various affinities.35,36 However, previous review has shown that a higher rate of neurological effects was associated with the intranasal route.37,38 Other adverse effects such as gastrointestinal, psychological, and cardiopulmonary effects were almost equivalent between the ketamine and opioid groups.
The major strength of this paper is that it provides an up-to-date, comprehensive review of the efficacy and safety of low-dose ketamine in the management of acute pain among patients presenting to the emergency setting. This review also includes a large number of studies to provide a reasonable estimate on burden. We performed additional sensitivity analysis, subgroup analysis, and meta-regression to provide a more robust estimate. We did not find significant publication bias, adding more credibility to the results.
LIMITATIONS
Our review did have certain limitations. Almost half of the included studies had high risk of bias. The chi square test for heterogeneity also revealed significant variability across the included studies. This could have led to biased estimates with limited generalizability. We tried to overcome this limitation by performing meta-regression. However, meta-regression could not be performed for the majority of the outcomes due to the limitation in the number of studies (<10 studies). Ketamine works fairly quickly, yet only four studies reported pain scores within 15 minutes, and only seven studies reported them within 30 minutes. This was a limitation with the primary studies, in that it was not possible to really report the full pain effect of ketamine. Finally, we could not perform subgroup analysis based on the type of pain. Future studies could specifically focus on different types of pain conditions, as the mechanism and neurochemistry behind the pain pathways for each condition is entirely different.
CONCLUSION
Low-dose ketamine may have equivalent or higher efficacy and safety when compared to opioids for managing acute pain among patients presenting to the emergency care setting. However, we could not make a conclusive recommendation based on the available evidence. Hence, further studies are required to compare the combination of ketamine with specific opioids to identify the best approach to pain control. This will help clinicians manage their patients with the least chance of complications and an optimal success rate.
Footnotes
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Yuetun Zuo, MD, Changxing People’s Hospital of China, Department of Emergency Medicine, 66 Taihu Middle Road, Huzhou, Zhejiang, China. Email: heiming7k@163.com. 5 / 2023; 24:644 – 653
Submission history: Revision received August 10, 2022; Submitted January 24, 2023; Accepted February 4, 2023
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. No author has professional or financial relationships with any companies that are relevant to this study. There are no conflicts of interest or sources of funding to declare.
REFERENCES
1. Cordell WH, Keene KK, Giles BK, et al. The high prevalence of pain in emergency medical care. Am J Emerg Med. 2002;20:165-9.
2. Todd KH, Ducharme J, Choiniere M, et al. Pain in the emergency department: results of the pain and emergency medicine initiative (PEMI) multicenter study. J Pain. 2007;8:460-6.
3. Todd KH. A Review of Current and emerging approaches to pain management in the emergency department. Pain Ther. 2017;6:193-202.
4. Hawk K, D’Onofrio G. Emergency department screening and interventions for substance use disorders. Addict Sci Clin Pract. 2018;13:18.
5. Ukkonen M, Jämsen E, Zeitlin R, et al. Emergency department visits in older patients: a population-based survey. BMC Emerg Med. 2019;19:20.
6. Ketamine. Available at: https://pubchem.ncbi.nlm.nih.gov/compound/3821. Accessed January 1, 2022.
7. Beatty L, MacQuarrie K, Zed P. Airway management pharmacology. Airway Management in Emergencies-A Free Open Access Living Textbook.
8. Kurdi MS, Theerth KA, Deva RS. Ketamine: current applications in anesthesia, pain, and critical care. Anesth Essays Res. 2014;8:283-90.
9. Majidinejad S, Esmailian M, Emadi M. Comparison of intravenous ketamine with morphine in pain relief of long bones fractures: a double blind randomized clinical trial. Emerg (Tehran). 2014;2:77-80.
10. Motov S, Rockoff B, Cohen V, et al. Intravenous subdissociative-dose ketamine versus morphine for analgesia in the emergency department: a randomized controlled trial. Ann Emerg Med. 2015;66:222-229.e1.
11. Forouzan A, Masoumi K, Motamed H, et al. Comparison of the analgesic effect of intravenous ketamine versus intravenous morphine in reducing pain of renal colic patients: double-blind clinical trial study. Rev Recent Clin Trials. 2019;14:280-5.
12. Karlow N, Schlaepfer CH, Stoll CRT, et al. A systematic review and meta-analysis of ketamine as an alternative to opioids for acute pain in the emergency department. Acad Emerg Med. 2018;25:1086-97.
13. Lee EN, Lee JH. The effects of low-dose ketamine on acute pain in an emergency setting: a systematic review and meta-analysis. PLoS One. 2016;11:e0165461.
14. Page MJ, McKenzie JE, Bossuyt PM, et al. Updating guidance for reporting systematic reviews: development of the PRISMA 2020 statement. J Clin Epidemiol. 2021:103-12.
15. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898.
16. Higgins J, PT , Green S. Cochrane Handbook for Systematic Reviews of Interventions. 2008. Available at: https://idostatistics.com/higgins-green-2008-cochrane-handbook-systematic-reviews-interventions/. Accessed December 13, 2019.
17. Egger M, Smith GD, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629-34.
18. Mahshidfar B, Mofidi M, Fattahi M, et al. Acute pain management in emergency department, low dose ketamine versus morphine, a randomized clinical trial. Anesth Pain Med. 2017;7:e60561.
19. Beaudoin FL, Lin C, Guan W, et al. Low-dose ketamine improves pain relief in patients receiving intravenous opioids for acute pain in the emergency department: results of a randomized, double-blind, clinical trial. Acad Emerg Med. 2014;21:1193-202.
20. Jahanian F, Hosseininejad SM, Amini Ahidashti H, et al. Efficacy and safety of morphine and low dose ketamine for pain control of patients with long bone fractures: a randomized, double-blind, clinical trial. Bull Emerg Trauma. 2018;6:31-6.
21. Esfahani H, Khazaeipour Z, Safaie A, et al. Ketamine sub-dissociative dose vs. morphine sulfate for acute pain control in patients with isolated limb injuries in the emergency department: a randomized, double-blind, clinical trial. Bull Emerg Trauma. 2021;9:73-9.
22. Motov S, Mann S, Drapkin J, et al. Intravenous subdissociative-dose ketamine versus morphine for acute geriatric pain in the emergency department: a randomized controlled trial. Am J Emerg Med. 2019;37:220-7.
23. Alshahrani MS, AlSulaibikh AH, ElTahan MR, et al. Ketamine administration for acute painful sickle cell crisis: a randomized controlled trial. Acad Emerg Med. 2022;29(2):150-8.
24. Carver TW, Kugler NW, Juul J, et al. Ketamine infusion for pain control in adult patients with multiple rib fractures: results of a randomized control trial. J Trauma Acute Care Surg. 2019;x:181-8.
25. Kugler NW, Carver TW, Juul J, et al. Ketamine infusion for pain control in elderly patients with multiple rib fractures: results of a randomized controlled trial. J Trauma Acute Care Surg. 2019;87:1181-8.
26. Etchison AR, Bos L, Ray M, et al. Low-dose ketamine does not improve migraine in the emergency department: a randomized placebo-controlled trial. West J Emerg Med. 2018;19:952-60.
27. Miller JP, Schauer SG, Ganem VJ, et al. Low-dose ketamine vs morphine for acute pain in the ED: a randomized controlled trial. Am J Emerg Med. 2015;33:402-8.
28. Galinski M, Dolveck F, Combes X, et al. Management of severe acute pain in emergency settings: ketamine reduces morphine consumption. Am J Emerg Med. 2007;134:385-90.
29. Sin B, Tatunchak T, Paryavi M, et al. The use of ketamine for acute treatment of pain: a randomized, double-blind, placebo-controlled trial. J Emerg Med. 2017;52:601-8.
30. Balzer N, McLeod SL, Walsh C, et al. Low-dose ketamine for acute pain control in the emergency department: a systematic review and meta-analysis. Acad Emerg Med. 2021;28:444-54.
31. Gupta A, Devi LA, Gomes I. Potentiation of μ-opioid receptor-mediated signaling by ketamine. J Neurochem. 2011;119:294-302.
32. Dickenson AH. NMDA receptor antagonists: interactions with opioids. Acta Anaesthesiol Scand. 1997;41:112-5.
33. Stubhaug A, Breivik H, Eide PK, et al. Mapping of punctuate hyperalgesia around a surgical incision demonstrates that ketamine is a powerful suppressor of central sensitization to pain following surgery. Acta Anaesthesiol Scand. 1997;41:1124-32.
34. Oye I, Paulsen O, Maurset A. Effects of ketamine on sensory perception: evidence for a role of N-methyl-D-aspartate receptors. J Pharmacol Exp Ther. 1992;260:1209-13.
35. Smith DJ, Bouchal RL, de Sanctis CA, et al. Properties of the interaction between ketamine and opiate binding sites in vivo and in vitro. Neuropharmacology. 1987;26:1253-60.
36. Sarton E, Teppema LJ, Olievier C, et al. The involvement of the mu-opioid receptor in ketamine-induced respiratory depression and antinociception. Anesth Analg. 2001;93:1495-500.
37. Oliveira JE, Silva L, Lee JY, Bellolio F, et al. Intranasal ketamine for acute pain management in children: a systematic review and meta-analysis. Am J Emerg Med. 2020;38(9):1860-6.
38. Seak YS, Nor J, Tuan Kamauzaman TH, et al. Efficacy and safety of intranasal ketamine for acute pain management in the emergency setting: a systematic review and meta-analysis. J Clin Med. 2021;10:3978.