
{kind=link}
| Author | Affiliation |
|---|---|
| Wirachin Hoonpongsimanont, MD, MS | University of California, Irvine School of Medicine, Department of Emergency Medicine, Orange, California; Eisenhower Medical Center, Department of Emergency Medicine, Rancho Mirage, California |
| Ghadi Ghanem, BS | University of California, Irvine School of Medicine, Department of Emergency Medicine, Orange, California |
| Preet Sahota, MS | University of California, Irvine School of Medicine, Department of Emergency Medicine, Orange, California |
| Abdullah Arif, BA | University of California, Irvine School of Medicine, Department of Emergency Medicine, Orange, California |
| Cristobal Barrios, MD | University of California, Irvine School of Medicine, Department of Surgery, Division of Trauma, Burns, and Critical Care & Acute Care Surgery, Orange, California |
| Soheil Saadat, MD, MPH, PhD | University of California, Irvine School of Medicine, Department of Emergency Medicine, Orange, California |
| Shahram Lotfipour, MD, MPH | University of California, Irvine School of Medicine, Department of Emergency Medicine, Orange, California; Eisenhower Medical Center, Department of Emergency Medicine, Rancho Mirage, California |
Introduction
Methods
Results
Discussion
Limitations
Conclusion
ABSTRACT
Introduction
Trauma patients who present to the emergency department (ED) intoxicated or with an alcohol use disorder (AUD) undergo more procedures and have an increased risk of developing complications. However, how AUD and blood alcohol concentration (BAC) impact a trauma patient’s disposition from the ED remains inconclusive. In this study we aimed to identify the associations between positive BAC or an AUD with admission to the hospital, including the intensive care unit (ICU).
Methods
This was a retrospective study analyzing data from 2010–2018 at a university-based, Level I trauma ED. Included in the study were 4,699 adult trauma patients who completed the Alcohol Use Disorders Identification Test (AUDIT) and had blood alcohol content test results.
Results
Positive BAC was associated with hospital admission and ICU admission after adjusting for injury severity score (ISS) (odds ratio 1.5 and 1.3, respectively). The AUDIT was only correlated with hospital and ICU admission in patients with ISS of 1 to 15. By increasing risk of AUD (low, moderate, high, and likely alcohol dependent) the proportion of ICU admissions rose from 29.3% to 37.3%, 40.0% and 42.0% (P <0.01). The results did not change significantly by adjustment for the age of patients.
Conclusion
BAC is associated with increasing ED disposition to the hospital or ICU. Furthermore, self-reported alcohol use was associated with an increased risk of hospital or ICU admission in patients with minor or moderate injuries. Further studies to determine viable options to decrease admission rates in these patients are warranted.
INTRODUCTION
Alcohol consumption can play a significant role in trauma patients’ visits to the emergency department (ED). Previous studies have found that between 33.5% and 47% of trauma patients presenting to the ED have a positive blood alcohol concentration (BAC).1, 2 Furthermore, a systematic review of trauma centers across the United States found that 26.2–62.5% of visits to trauma centers were alcohol related.3
Alcohol consumption prior to injury has been shown to lead to higher rates of infection-related complications and more diagnostic tests, which ultimately results in longer lengths of stay, extra procedures, higher hospitalization costs, and a higher probability of hospital admission.4-6 Patients with positive BACs are most likely to present to the ED between midnight and 2 am, have a higher injury severity score (ISS), and have an increased risk of head trauma.6-8 While BAC is the most commonly used tool for assessing patients’ acute alcohol consumption levels, it cannot capture and often misses habitual consumption levels.9,10 Blood alcohol concentration has also been shown to miss more than one third of trauma patients with a current alcohol use disorder (AUD).11 For that reason, many EDs have incorporated increased screening for AUDs in their patient populations.
Alcohol use disorder has become increasingly prevalent in trauma patients. A study conducted across four major trauma centers in Los Angeles found that 24.0% of patients were characterized with AUD.12 Furthermore, on a national level, 34.3% of adult ED patients have either risky drinking, problem drinking, or alcohol-dependence behaviors.13 Researchers have also found upward trends in alcohol-related ED visits over a nine-year period, indicating an increase in problematic drinking in this population over time.14 In the trauma population, AUD and substance use disorders in general are associated with increased mortality.15 Other studies beyond emergency medicine have found that in patients who undergo surgery, having an AUD was strongly correlated with hospital readmission. The readmitted patients with an AUD also had increased length of stay, hospitalization costs, and risk of death.16
Due to the increasing prevalence of AUD in trauma patients, the American College of Surgeons Committee on Trauma has mandated that Level I trauma centers provide alcohol screening to all trauma patients and interventions for those with high risk of AUD. The current standard alcohol screening tool is the Alcohol Use Disorders Identification Test (AUDIT). The AUDIT is a self-reported, 10-item questionnaire developed by the World Health Organization; it is designed to assess patients’ alcohol consumption habits over the prior year.17 Upon completion of the questionnaire, a score is generated, which ranges from 0–40 and categorizes the patient as either low risk for alcohol dependence (0–7) or high risk for alcohol dependence (8–19), or likely alcohol dependent (20–40). Patients with AUDIT scores of 8–19 are offered a personalized brief intervention aimed at reducing their alcohol consumption, which has proven effective.18-20 Despite the self-report bias present in AUDIT, the survey has been shown to be a reliable and well-validated measure to assess habitual alcohol intake in patients.21-25 Delivering the AUDIT test through a self-administered, computerized system has also been shown to be feasible and may reduce biases associated with alcohol reporting.22,26
While many studies have found correlations between alcohol consumption and a myriad of other variables, the evidence for associations between AUDIT and disposition in trauma patients is limited. In this study, we aimed to identify the correlation between acute and chronic alcohol consumption, as defined by BAC and AUDIT, respectively, with disposition of trauma patients from the ED.
METHODS
Study Setting and Design
We conducted a retrospective, chart review study on databases that were obtained at a Level I trauma center, university-based ED between 2010–2018. Patients were included if they were over 18 years of age and met trauma activation criteria (Supplemental Document). All these patients completed the AUDIT in either Spanish or English. The study was reviewed and approved by the university’s institutional review board as an exempt category. Patient informed consent was not applicable to this study.
Population Health Research Capsule
What do we already know about this issue?
Alcohol consumption has a significant impact on trauma patients’ care in the emergency department.
What was the research question?
What is the association between alcohol consumption and disposition of trauma patients from the ED?
What was the major finding of the study?
Positive blood alcohol concentration and self-reported alcohol use were associated with hospital and intensive care unit admission in trauma patients.
How does this improve population health?
Effective alcohol screening and intervention could help reduce the admission rate in trauma patients.
Study Protocol
We obtained our data from two databases: the hospital Trauma Registry and the Computerized Alcohol Screening and Intervention (CASI) program database. The Trauma Registry database compiles patient information from all trauma patients as part of quality assurance. Data analysts obtained patient demographics; nurse abstractors obtained information on patient injuries, treatments, BAC, and diagnoses/outcomes. We obtained ED disposition (death, intensive care unit [ICU] admission, hospital admission, and discharge from the ED), BAC, and ISS27 from this database. When patients were first admitted to the ED, and trauma surgeons deemed it appropriate, the patients received venous blood draws to measure BAC as part of evaluation protocols. We included only patients who had BAC measurement results.
The CASI database was compiled by trained research associates (RA) who administered the AUDIT to trauma patients. Implementation of AUDIT screening was standard of care for trauma patients from 8 am to midnight in the ED, and 8 am to noon in the inpatient units. All trauma patients were approached to complete the AUDIT when they were clinically stable during their stay in the ED or inpatient units. Patients completed the AUDIT on a CASI tablet privately, unless a patient specifically requested assistance from an RA. Responses to individual questions were kept confidential. The AUDIT score is shared with the patient, and a printout of the score is attached to the patient’s medical record. We excluded patients who were on a psychiatric hold, incarcerated, or pregnant. For those with cognitive impairments such as acute intoxication, altered mental status, and critical illness, the RAs approached the patients once their conditions were resolved. The AUDIT results and demographic information were electronically recorded and automatically stored in a secure hospital database. We extracted patient demographic data and AUDIT scores from this database.
The two databases were linked by a unique identifier for each patient using Python Language Reference version 2.7 (Python Software Foundation, Wilmington, DE).
Statistical Analysis
Frequencies are reported as N (%). We studied the distribution of categorical variables using the chi-square, or chi-square for trend, statistical test. Associations of BAC and AUDIT with ICU admission and hospital admission were studied by calculating odds ratios (OR) in each level of ISS. We examined the homogeneity of estimated OR among levels of ISS using the Breslow-Day statistical test, and if the homogeneity was not rejected we reported a Mantel-Haenszel common OR. Statistical analyses were performed using SPSS Statistics 25 for Windows (IBM Corporation, Armonk, NY).
RESULTS
We identified a total of 4,699 adult trauma patients with known BAC who had completed the AUDIT questionnaire. Of these patients 3116 were male and 1583 were female (Table 1). The mean age of female patients was 51.4 years (±30.20) compared to 42.2 years (±19.86) in male patients (P <0.001). While male patients were younger, a higher percentage of them presented with an ISS score greater than 15 (P = 0.001). A total of 3551 (75.6%) patients had a BAC of zero upon arrival to the ED; 243 (5.2%) patients presented with a BAC greater than 250 milligrams per deciliter (mg/dL). A greater percentage of male patients presented with positive BAC (Table 1) as compared to female patients (P < 0.001). A similar pattern was observed with AUDIT scores.
| Gender | Total | ||
|---|---|---|---|
|
|
|||
| Male | Female | ||
| Age (Mean ± SD) | 42.2 ± 19.86 | 51.4 ± 30.20 | 45.3 ± 24.24 |
| ISS | |||
| 1–15 | 2,394 (76.8%) | 1,292 (81.6%) | 3,686 (78.4%) |
| 16–24 | 460 (17.8%) | 177 (11.2%) | 637 (13.6%) |
| =>25 | 262 (8.4%) | 114 (7.2%) | 376 (8.0%) |
| Blood Alcohol Concentration (mg/dL) | |||
| 0.0 | 2,205 (70.8%) | 1,346 (85.0%) | 3,551 (75.6%) |
| 0.1 – 100.0 | 318 (10.2%) | 78 (4.9%) | 396 (8.4%) |
| 100.1 – 250.0 | 398 (12.8%) | 111 (7.0%) | 509 (10.8%) |
| >250.0 | 195 (6.3%) | 48 (3.0%) | 243 (5.2%) |
| AUDIT score | |||
| 0–7 | 2,582 (82.9%) | 1,494 (94.4%) | 4,076 (86.7%) |
| 8–15 | 347 (11.1%) | 63 (4.0%) | 410 (8.7%) |
| 16–19 | 79 (2.5%) | 10 (0.6%) | 89 (1.9%) |
| =>20 | 108 (3.5%) | 16 (1.0%) | 124 (2.6%) |
| ED disposition | |||
| Discharged | 470 (15.1%) | 291 (18.4%) | 761 (16.2%) |
| In Hospital (non-ICU) | 1,482 (47.7%) | 816 (51.6%) | 2,298 (49.0%) |
| ICU | 1,157 (37.2%) | 474 (30.0%) | 1,631 (34.8%) |
| Dead | 1 (0.0%) | 1 (0.1%) | 2 (0.0%) |
SD, standard deviation; ISS, Injury Severity Score; mg, milligram; dL, deciliter; AUDIT, Alcohol Use Disorders Identification Test; ED, emergency department; ICU, intensive care unit.
Associated Factors with Hospital and ICU Admission: All Patients
Our results showed an association between positive blood alcohol with both hospital admission and ICU admission (among those who had been admitted to the hospital) after adjusting for ISS (Mantel-Haenszel OR: 1.5 [1.2 – 1.9] and 1.3 [1.1 – 1.5], respectively) (Table 2). The association was still significant after adjusting for age groups (18–30, 31–50, 51+) and ISS (Mantel-Haenszel OR: 1.7 [1.4–2.1] and 1.4 [1.2–1.7], respectively (Appendices 1 and 2). However, we did not find a statistically significant association between AUDIT score when considered as a score of zero (ie, self-reported abstainer) vs “1 or more” scores, and hospital (P = 0.763) or ICU admission (P = 0.494) after adjustment for ISS.
| ISS levels | Hospital admission | ICU admission | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|||||||||||
| No | Yes* | Total | Odds ratio (95% CI) | No | Yes | Total | Odds ratio (95% CI) | ||||
| 1–15 | BA | Negative | Count | 614 | 2,194 | 2,808 | 1.53 (1.2 – 1.9) | 1,547 | 641 | 2,188 | 1.3 (1.1 – 1.5) |
| row % | 21.9% | 78.1% | 100.0% | 70.7% | 29.3% | 100.0% | |||||
| Positive | Count | 134 | 734 | 868 | 480 | 254 | 734 | ||||
| row % | 15.4% | 84.6% | 100.0% | 65.4% | 34.6% | 100.0% | |||||
| Total | Count | 748 | 2,928 | 3,676 | 2,027 | 895 | 2,922 | ||||
| row % | 20.3% | 79.7% | 100.0% | 69.4% | 30.6% | 100.0% | |||||
| 16–24 | BA | Negative | Count | 7 | 479 | 486 | 0.7 (0.2 – 2.8) | 169 | 309 | 478 | 1.4 (0.9 – 2.1) |
| row % | 1.4% | 98.6% | 100.0% | 35.4% | 64.6% | 100.0% | |||||
| Positive | Count | 3 | 146 | 149 | 41 | 105 | 146 | ||||
| row % | 2.0% | 98.0% | 100.0% | 28.1% | 71.9% | 100.0% | |||||
| Total | Count | 10 | 625 | 635 | 210 | 414 | 624 | ||||
| row % | 1.6% | 98.4% | 100.0% | 33.7% | 66.3% | 100.0% | |||||
| =>25 | BA | Negative | Count | 2 | 255 | 257 | 1.0(1.0 – 1.0) | 37 | 217 | 254 | 1.0 (0.6 – 2.0) |
| row % | 0.8% | 99.2% | 100.0% | 14.6% | 85.4% | 100.0% | |||||
| Positive | Count | 0 | 115 | 115 | 16 | 98 | 114 | ||||
| row % | 0.0% | 100.0% | 100.0% | 14.0% | 86.0% | 100.0% | |||||
| Total | Count | 2 | 370 | 372 | 53 | 315 | 368 | ||||
| row % | 0.5% | 99.5% | 100.0% | 14.4% | 85.6% | 100.0% | |||||
| Total | BA | Negative | Count | 623 | 2,928 | 3,551 | Mantel-Haenszel common odds ratio: | 1,753 | 1,167 | 2,920 | Mantel-Haenszel common odds ratio: |
| row % | 17.5% | 82.5% | 100.0% | 60.0% | 40.0% | 100.0% | |||||
| Positive | Count | 137 | 995 | 1,132 | 537 | 457 | 994 | ||||
| row % | 12.1% | 87.9% | 100.0% | 1.5 (1.2 – 1.9)P <0.001 | 54.0% | 46.0% | 100.0% | 1.3 (1.1 – 1.5)P = 0.002 | |||
| Total | Count | 760 | 3,923 | 4,683 | 2,290 | 1,624 | 3,914 | ||||
| row % | 16.2% | 83.8% | 100.0% | 58.5% | 41.5% | 100.0% | |||||
*Including 2 dead.
ISS, Injury Severity Score; CI, confidence interval; ICU, intensive care unit; BA, blood alcohol.
Associated Factors with Hospital Admission in Patients with Injury Severity Score 1–15
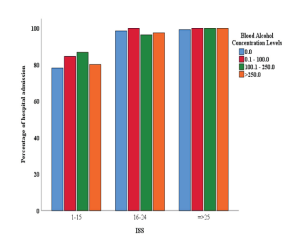
There was a statistically significant association between hospital admission and BAC among patients with ISS of 1–15 (Figure 1). By increasing BAC (from 0 mg/dL to 0.1–100 mg/dL, 100.1–250 mg/dL, and >250 mg/dL) the proportion of hospital admission rose from 78.1% to 84.5%, 86.8% and 80.1%, respectively (P = 0.001). The association remains statistically significant (P < 0.001) after adjustment for age (Appendix 3).
A similar association was observed between hospital admission and AUDIT scores in patients with an ISS of 1–15 (Figure 2). By increasing AUDIT levels (from 0–7 to 8–15, 16–19, and ≥20) the proportion of hospital admissions rose from 79.1% to 82.2%, 79.4% and 88.9%, respectively (P = 0.016). The association remained statistically significant (P < 0.001) after adjustment for age (Appendix 4).

Associated Factors with ICU Admission in Patients with ISS 1–15 Who Were Amitted to the Hospital
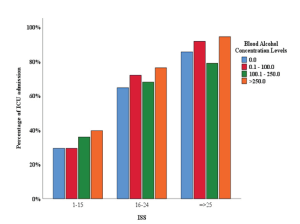
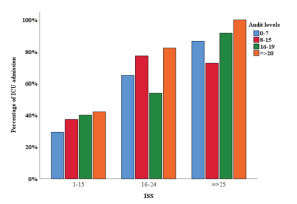
Among the patients who had been admitted into the hospital, we found a statistically significant association between ICU admission and BAC in patients with ISS of 1–15 (Figure 3). The proportion of ICU admissions in patients with BAC up to 100 mg/dL was 29.3%. The proportion of ICU admissions rose to 35.9% and 39.6% by increasing BAC to 100.1–250 mg/dL and >250 mg/dL, respectively (P = 0.001). The association remained statistically significant (P <0.001) after adjustment for age (Appendix 5). We observed a similar association between ICU admission and AUDIT scores in the same group of patients (Figure 4). By increasing AUDIT levels (from 0–7 to 8–15, 16–19, and ≥ 20) the proportion of ICU admissions rose from 29.3% to 37.3%, 40.0% and 42.0%, respectively. (P <0.001). The association remained statistically significant (P <0.001) after adjustment for age (Appendix 6).
DISCUSSION
When we considered BAC as a dichotomous variable (BAC 0 mg/dL and BAC >0 mg/dL), we found that positive blood alcohol is associated with increased risk of hospital and ICU admission. Having a positive BAC may complicate the initial patient presentation and subsequent tests, especially in patients with lower ISS, whereas the effects of chronic alcohol use may not have yet manifested. Management and differentials of patients are also complicated by alcohol use, as intoxication may mask the effects of a stroke or head injury.28 Physicians may, therefore, opt to admit these patients until they are stable and can be properly assessed. Furthermore, patients who are undomiciled are more than twice as likely to present with positive BAC after a trauma than a comparative sample of domiciled patients.29 This may complicate the discharge process for lower ISS patients who do not have reliable transportation, a shelter to return to, or a follow-up plan. This population also has a higher rate of psychiatric-related admissions.29
Intoxicated trauma patients are less likely to sustain severe injuries.30,31 However, they are more likely to present with a depressed Glasgow Coma Scale score,32 which is usually associated with intracranial trauma, hypoxia, or shock from associated injuries. This may prompt physicians to admit these patients for further investigation and work-up. Furthermore, these patients may be cognitively impaired, even as their blood alcohol levels approach zero or may go on to develop complications from alcohol withdrawal syndrome that will eventually require hospital admission.33
Trauma patients who are BAC positive are more likely to have a pre-existing condition of chronic alcohol use, cirrhosis, coagulopathy, chronic pulmonary condition, chronic obstructive pulmonary disease, or chronic drug use.34 Another study found that 66% of frequent binge drinkers and 10% of infrequent binge drinkers were found to be BAC positive upon admission.35 Binge drinking is known to dysregulate adipocyte and liver function, thereby contributing to metabolic derangement and alcoholic liver disease.36 A single binge-alcohol session can also modulate immune system functioning.37 The combination of pre-existing conditions and impaired immune function may, therefore, contribute to the increased risk of infections observed in patients with positive BAC.38 Other studies have indicated that patients with positive BAC also have a higher risk of developing pneumonia.39 These complications may encourage a physician to admit patients with positive BAC either due to incidental findings (not related to the trauma) or fear of patient deterioration.
When we categorized AUDIT into four levels (0–7, 8–15, 16–19, ≥20) we observed statistically significant associations between AUDIT levels and both ICU and hospital admission only in patients with ISS of 1–15. The AUDIT is a reflection of the patient’s perceived long-term alcohol consumption habits. Chronic alcohol use has been found to contribute to a plethora of diseases and immune dysfunctions, as well as comorbidities with other psychological disorders.40,41 In severely injured patients (ISS greater than 15), the health consequences of chronic alcohol use was likely to have been masked or superseded by the traumatic injury. But when the injuries were minor (ISS 1–15), the effects of chronic alcohol use on the patient’s health became more prominent and possibly contributed to hospital admission. Previous studies have identified that orthopedic trauma patients with a history of AUD are more likely to be admitted and have an increased length of stay.42,43 However, many of these studies were unable to discern a cause behind these statistics. Our results would indicate that the skew in data may have been primarily due to patients with minor injuries but higher risk of AUD. We therefore recommend that future studies designed to discern the effects of AUD on patient outcomes should further stratify this population by ISS.
LIMITATIONS
Patients with prolonged altered mental status due to various reasons, including intoxication and being intubated, completed the AUDIT at a later stage of their hospital stay or were excluded from our study. Although most patients completed the study within 48 hours while they were still in the ED, the accuracy of AUDIT responses might diminish if the patients completed the survey near the time of their discharge. Trauma patients with the inability to personally complete the survey due to their injuries completed the AUDIT with assistance from research personnel, which may have introduced social desirability response biases in these patients. Furthermore, ethanol tolerance may skew the symptoms of intoxication for patients with a history of AUD, thereby complicating the scale of BAC intoxication and clinical intoxication.44 Systemic biases have also been found in determining which patients are tested for BAC, which may have caused us to miss some patients on initial presentation.45
Other patient care outcomes besides hospital admission, such as alcohol withdrawal symptoms and poor surgical outcomes, may impact patient management but were not available in our databases.
CONCLUSION
Blood alcohol concentration is a reflection of acute alcohol use, often correlated with binge drinking and adverse effects on human health. The presence of BAC was found to be associated with hospital and ICU admissions after adjustment for Injury Severity Score; therefore, screening BAC might expedite disposition of trauma patients in the ED. The Alcohol Use Disorder Identification Test is a self-reported reflection of perceived alcohol consumption habits and possible chronic alcohol use. Our study found that AUDIT is associated with an increased risk of hospital or ICU admission in minor or moderately injured trauma patients only.
Footnotes
Section Editor: Eric Snoey, MD
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Wirachin Hoonpongsimanont, MD, MS, Eisenhower Medical Center, Department of Emergency Medicine, 39000 Bob Hope Dr., Rancho Mirage, CA 92270. Email: wirachin@gmail.com. 3 / 2022; 23:158 – 165
Submission history: Revision received December 29, 2020; Submitted July 23, 2021; Accepted September 9, 2021
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. No author has professional or financial relationships with any companies that are relevant to this study. There are no conflicts of interest or sources of funding to declare.
REFERENCES
1. Soderstrom CA, Trifillis AL, Shankar BS, et al. Marijuana and alcohol use among 1023 trauma patients. Arch Surg. 1988;123(6):733-7.
2. Rivara FP, Jurkovich GJ, Gurney JG, et al. The magnitude of acute and chronic alcohol abuse in trauma patients. Arch Surg. 1993;128(8):907-12.
3. MacLeod JBA, Hungerford DW. Alcohol-related injury visits: Do we know the true prevalence in U.S. trauma centres?. Injury. 2011;42(9):922-6.
4. Cowperthwaite MC, Burnett MG. Treatment course and outcomes following drug and alcohol-related traumatic injuries. J Trauma Manag Outcomes. 2011;5:3.
5. O’Keeffe T, Rhee P, Shafi S, et al. Alcohol use increases diagnostic testing, procedures, charges, and the risk of hospital admission: a population-based study of injured patients in the emergency department. Am J Surg. 2013;206(1):16-22.
6. Cittadini F, De Giovanni N, Caradonna L, et al. Prevalence of alcohol and other drugs in injured drivers and their association with clinical outcomes. Eur Rev Med Pharmacol Sci. 2017;21(9):2008-14.
7. Comelli I, Lippi G, Sanchis-Gomar F, et al. Visits for alcohol-related problems in a large urban emergency department. Results of a 15-year survey. Acta Biomed. 2018;88(4):514-8.
8. Savola O, Niemelä O, Hillbom M. Alcohol intake and the pattern of trauma in young adults and working aged people admitted after trauma. Alcohol Alcohol. 2005;40(4):269-73.
9. Paton A. Alcohol in the body. BMJ. 2005;330(7842):85-7.
10. Ewing T, Barrios C, Lau C, et al. Predictors of hazardous drinking behavior in 1,340 adult trauma patients: a computerized alcohol screening and intervention study. J Am Coll Surg. 2012;215(4):489-95.
11. Soderstrom CA, Smith GS, Dischinger PC, et al. Psychoactive substance use disorders among seriously injured trauma center patients. JAMA. 1997;277(22):1769-74.
12. Ramchand R, Marshall GN, Schell TL, et al. Alcohol abuse and illegal drug use among Los Angeles County trauma patients: prevalence and evaluation of single item screener. J Trauma. 2009;66(5):1461-7.
13. Cherpitel CJ, Ye Y. Drug use and problem drinking associated with primary care and emergency room utilization in the US general population: data from the 2005 National Alcohol Survey. Drug Alcohol Depend. 2008;97(3):226-30.
14. McDonald AJ, Wang N, Camargo CA. US emergency department visits for alcohol-related diseases and injuries between 1992 and 2000. Arch Intern Med. 2004;164(5):531-7.
15. Dezman ZDW, Gorelick DA, Buchanan L, et al. 20-year mortality after discharge in a cohort of 1,099 former trauma inpatients with and without substance use disorders. Injury. 2020;51(12):2930-7.
16. Gili-Miner M, Béjar-Prado L, Gili-Ortiz E, et al. Alcohol use disorders among surgical patients: unplanned 30-days readmissions, length of hospital stay, excessive costs and mortality. Drug Alcohol Depend. 2014;137:55-61.
17. Saunders JB, Aasland OG, Babor TF, et al. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption–II. Addiction. 1993;88(6):791-804.
18. Lotfipour S, Mortazavi R, Chakravarthy B. Commentary: Alcohol and motor vehicle-related crashes–driver attitudes need further intervention. Ann Emerg Med. 2011;57(4):406-8.
19. Harrison C, Hoonpongsimanont W, Anderson CL, et al. Readiness to change and reasons for intended reduction of alcohol consumption in emergency department versus trauma population. West J Emerg Med. 2014;15(3):337-44.
20. Neumann T, Neuner B, Weiss-Gerlach E, et al. The effect of computerized tailored brief advice on at-risk drinking in subcritically injured trauma patients. J Trauma. 2006;61(4):805-14.
21. Imani G, Barrios C, Anderson CL, et al. Computerized alcohol screening identified more at-risk drinkers in a Level 2 than a Level 1 trauma center. BMC Public Health. 2017;17(1):32.
22. Lotfipour S, Howard J, Roumani S, et al. Increased detection of alcohol consumption and at-risk drinking with computerized alcohol screening. J Emerg Med. 2013;44(4):861-6.
23. Vaca F, Winn D, Anderson C, et al. Feasibility of emergency department bilingual computerized alcohol screening, brief intervention, and referral to treatment. Subst Abus. 2010;31(4):264-9.
24. Albright JM, Kovacs EJ, Gamelli RL, et al. Implications of formal alcohol screening in burn patients. J Burn Care Res. 2009;30(1):62-9.
25. Sakai LM, Esposito TJ, Ton-That HH, et al. Comparison of objective screening and self-report for alcohol and drug use in traumatically injured patients. Alcohol Treat Q. 2012;30(4):433-42.
26. Lotfipour S, Cisneros V, Chakravarthy B, et al. Assessment of readiness to change and relationship to AUDIT score in a trauma population utilizing computerized alcohol screening and brief intervention. Subst Abus. 2012;33(4):378-86.
27. Baker SP, Neill B, Haddon W, et al. The Injury Severity Score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma Acute Care Surg. 1974;14(3):187-96.
28. Arokszallasi T, Balogh E, Csiba L, et al. Acute alcohol intoxication may cause delay in stroke treatment – case reports. BMC Neurol. 2019;19(1):14.
29. Miller JP, O’ Reilly GM, Mackelprang JL, et al. Trauma in adults experiencing homelessness. Injury. 2020;51(4):897-905.
30. Velmahos GC, Jindal A, Chan LS, et al. “Insignificant” mechanism of injury: not to be taken lightly. J Am Coll Surg. 2001;192(2):147-52.
31. Sarani B, Temple-Lykens B, Kim P, et al. Factors associated with mortality and brain injury after falls from the standing position. J Trauma. 2009;67(5):954-8.
32. Hadjizacharia P, O’Keeffe T, Plurad DS, et al. Alcohol exposure and outcomes in trauma patients. Eur J Trauma Emerg Surg. 2011;37(2):169-75.
33. Heffernan T, Samuels A, Hamilton C, et al. Alcohol hangover has detrimental impact upon both executive function and prospective memory. Front Psychiatry. 2019;10:282.
34. Cowperthwaite MC, Burnett MG. Treatment course and outcomes following drug and alcohol-related traumatic injuries. J Trauma Manag Outcomes. 2011;5:3.
35. Savola O, Niemelä O, Hillbom M. Blood alcohol is the best indicator of hazardous alcohol drinking in young adults and working-age patients with trauma. Alcohol. 2004;39(4):340-5.
36. Parker R, Kim S-J, Gao B. Alcohol, adipose tissue and liver disease: mechanistic links and clinical considerations. Nat Rev Gastroenterol Hepatol. 2018;15(1):50-9.
37. Afshar M, Richards S, Mann D, et al. Acute immunomodulatory effects of binge alcohol ingestion. Alcohol. 2015;49(1):57-64.
38. Cowperthwaite MC, Burnett MG. Treatment course and outcomes following drug and alcohol-related traumatic injuries. J Trauma Manag Outcomes. 2011;5:3.
39. Ahmed N, Greenberg P. Examining the influence of blood alcohol level on the incidence of pneumonia & sepsis complications following traumatic injury. Alcohol. 2019;76:111-5.
40. Cook RT. Alcohol abuse, alcoholism, and damage to the immune system–a review. Alcohol Clin Exp Res. 1998;22(9):1927-42.
41. Gauba D, Thomas P, Balhara YP, et al. Psychiatric comorbidity and physical correlates in alcohol-dependent patient. Indian J Psychol Med. 2016;38(5):414-8.
42. Gitajn IL, Reider L, Scharfstein DO, et al. Variability in discharge disposition across US trauma centers after treatment for high-energy lower extremity injuries. J Orthop Trauma. 2020;34(3):e78-e85.
43. Vincent HK, Vasilopoulos T, Zdziarski-Horodyski LA, et al. Preexisting psychiatric illness worsens acute care outcomes after orthopaedic trauma in obese patients. Injury. 2018;49(2):243-8.
44. Olson KN, Smith SW, Kloss JS, et al. Relationship between blood alcohol concentration and observable symptoms of intoxication in patients presenting to an emergency department. Alcohol Alcohol. 2013;48(4):386-9.
45. Cheever CS, Barbosa-Leiker C. Impact of alcohol screening for traumatic brain injury patients being admitted to neurosurgical intensive care unit. J Neurosci Nurs. 2018;50(2):83-7.