
| Author | Affiliation |
|---|---|
| Brandon M. Carius, DSc, MPAS, PA-C | Brian D. Allgood Army Community Hospital, Department of Emergency Medicine, Camp Humphreys, Republic of Korea |
| Edward J. Houston, MD | Brian D. Allgood Army Community Hospital, Department of Emergency Medicine, Camp Humphreys, Republic of Korea |
| Stephen P. Griffith, MD, JD, FAAEM | Brian D. Allgood Army Community Hospital, Department of Emergency Medicine, Camp Humphreys, Republic of Korea |
Introduction
Case report
Discussion
Conclusion
ABSTRACT
Introduction
A cornual pregnancy describes a rare ectopic location positioned within the myometrium next to the fallopian tube, which can be difficult to find on traditional ultrasound imaging. Given its location and the stretch within the uterine wall, cornual pregnancies can progress for weeks prior to diagnosis. Ruptures can, therefore, be catastrophic with disproportionally high maternal mortality rates compared to other ectopic pregnancies.
Case Report
A 34-year-old female recently treated with methotrexate for ectopic pregnancy presented to the emergency department (ED) for acute onset of lower abdominal cramping without vaginal bleeding. She arrived clinically stable and quickly decompensated with witnessed syncope in the ED, prompting point-of-care ultrasound showing free fluid in the abdomen. The patient was taken for emergent surgery by obstetrics while receiving transfusion of blood products for suspected ruptured ectopic pregnancy. A fetus estimated to be 10 weeks of age was discovered in the left cornual region. Approximately two liters of intraperitoneal blood were drained without complication.
Conclusion
Cornual pregnancy is a difficult to diagnose but potentially disastrous type of ectopic pregnancy due to massive hemorrhage. Emergency clinicians should be aware of this condition given its rare occurrence but potentially catastrophic outcomes.
INTRODUCTION
Pregnancy complications are frequently seen in the emergency department (ED) setting, where evaluation includes hemodynamic stability and pregnancy location and viability. While modern ultrasound (US) can help locate pregnancy and assess viability, some may be difficult to locate. Cornual pregnancy is a rare type of ectopic pregnancy rarely described in emergency medicine literature. Because it may go unidentified for weeks cornual pregnancy demonstrates high maternal mortality because of its delayed diagnosis and massive hemorrhage with rupture. We report a case of this rare type of ruptured ectopic pregnancy presenting as stable abdominal pain with sudden hemodynamic instability due to severe intraperitoneal hemorrhage.
CASE REPORT
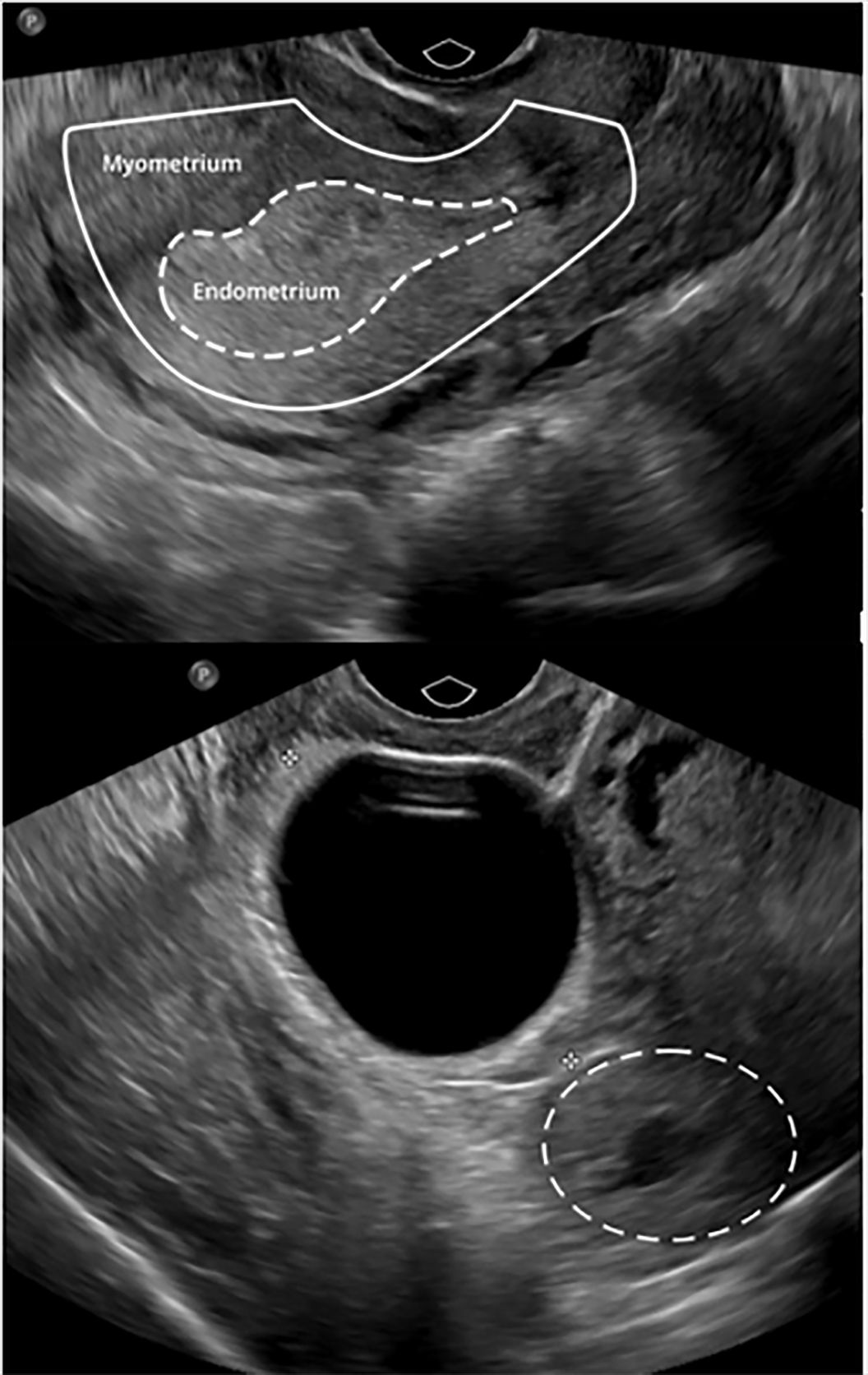
A 34-year-old gravida four, para two female with history of two ectopic pregnancies arrived at the ED complaining of 20 minutes of left-sided lower abdominal pain with four episodes of non-bloody emesis. She denied other symptoms, including vaginal bleeding. Initial medical history included two previous ectopic pregnancies; the first, approximately six months prior to arrival at the ED, resolved with intramuscular methotrexate. Her second ectopic pregnancy was suspicious for cornual pregnancy based on history and US at seven weeks estimated gestational age (Image 1) but had been officially diagnosed by obstetrics as an ectopic pregnancy of unknown location and deemed resolved after intramuscular methotrexate one month prior to arrival. After initial quantitative beta-human chorionic gonadotropin (βhCG) of over 16,000 milli-international units per milliliter (mIU/mL) (normal hCG range: <3 mIU/mL), her levels fell to 1700 mIU/mL two weeks prior to arrival.
Triage vital signs were significant for blood pressure (BP) of 86/51 millimeters mercury (mm Hg) but were otherwise within normal limits, including a heart rate (HR) of 85 beats per minutes (bpm). Physical examination revealed voluntary guarding of the abdomen and only moderate tenderness of the left lower quadrant. A one-liter saline intravenous bolus provided transient BP improvement to 108/58 mm Hg with other vital signs within normal limits. While preparing for an abdominal and pelvic computed tomography, initial complete blood count (CBC) found stable hemoglobin and hematocrit of 12.0 grams/deciliter (g/dL) (reference range: 12.0 – 16.5 g/dL) and 36.1% (reference range 36.0 – 49.5%), respectively. Approximately five minutes after last vital signs were taken, the patient stood to provide a urine sample and nursing witnessed sudden diffuse pallor immediately followed by syncope lasting less than 60 seconds. Repeat vital signs revealed BP of 68/38 mm Hg and HR of 108 bpm. After being placed in Trendelenburg position, type and cross, quantitative βhCG, and repeat CBC were drawn.
CPC-EM Capsule
What do we already know about this clinical entity?
Cornual pregnancy describes a rare, potentially disastrous implantation within the myometrium beside the fallopian tube, difficult to find on traditional ultrasound.
What makes this presentation of disease reportable?
This case illustrates a ruptured cornual pregnancy in the ED with severe hemorrhage, previously thought resolved by methotrexate via obstetrics.
What is the major learning point?
Given extended progression prior to diagnosis and disproportionate maternal mortality, cornual pregnancy should be a chief concern in suspected ectopic pregnancy.
How might this improve emergency medicine practice?
Cornual pregnancy is best diagnosed by three-dimensional ultrasound. Given high mortality from hemorrhage, all cases require emergent obstetrics consultation.
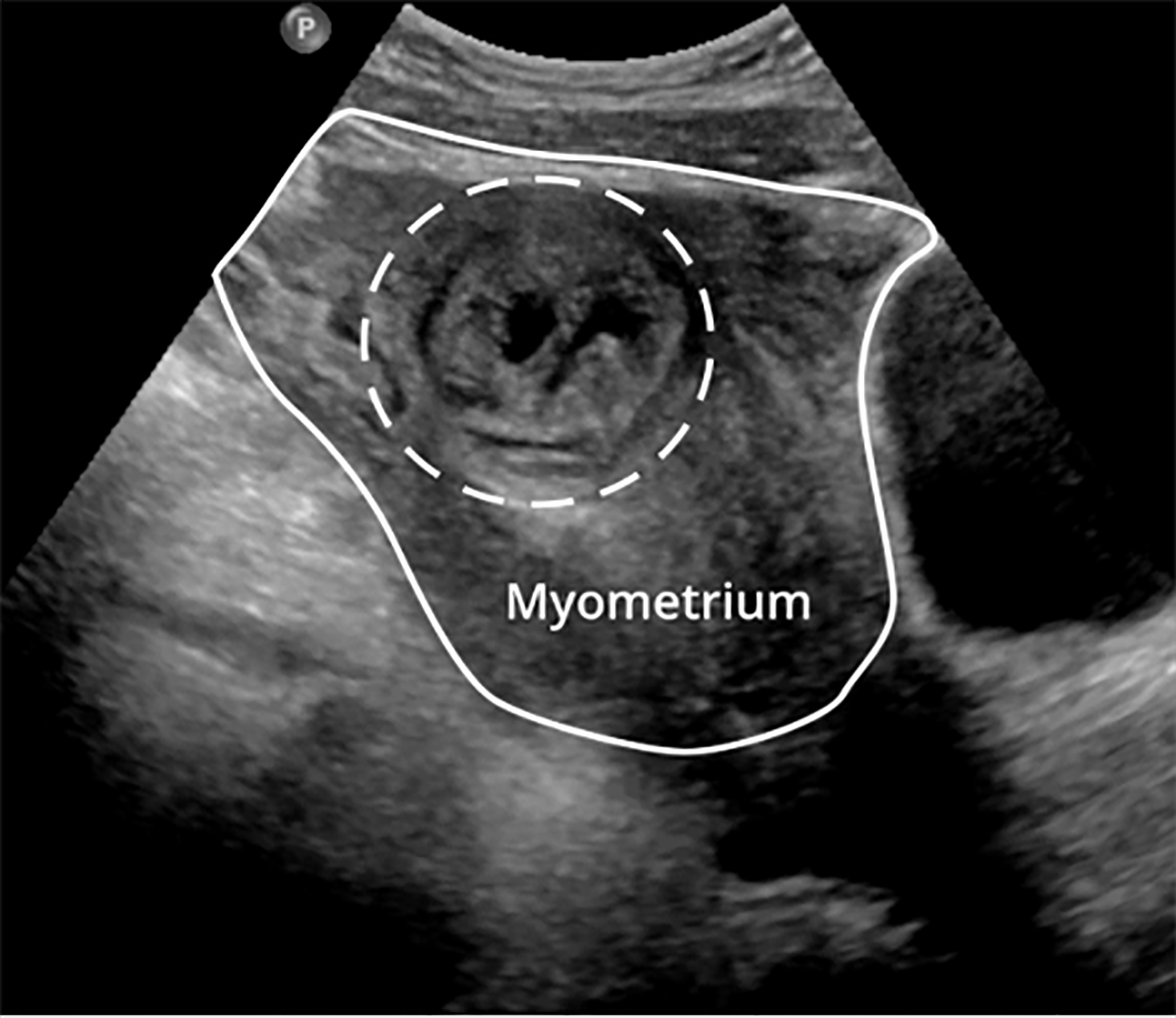
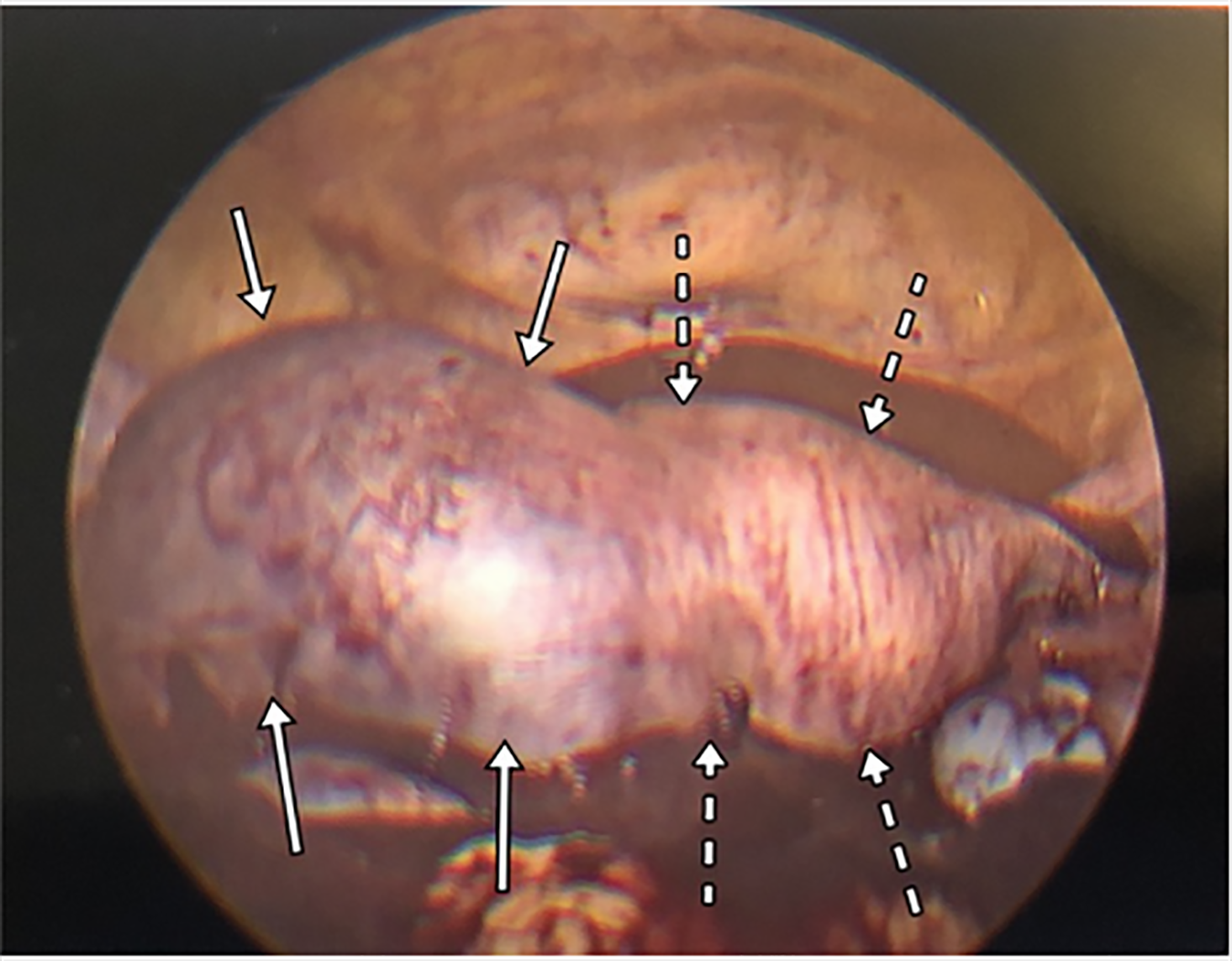
Point-of-care US revealed free fluid in the abdomen as well as a thickened endometrium with an endometrial mass (Image 2). Obstetrics was emergently consulted for suspected ectopic rupture; upon arrival to bedside, repeat hemoglobin and hematocrit revealed a dramatic decline to 6.2 g/dL and 20.1%, suspected due to hemorrhage. Two units of packed red blood cells were administered en route to the operating room. The surgeons found approximately two liters of intraperitoneal blood and diagnosed a ruptured, left cornual ectopic pregnancy (Image 3). A cornual wedge resection and a unilateral salpingectomy were performed. The patient recovered uneventfully and was discharged on postoperative day three.
{kind=link}
DISCUSSION
In the past, a cornual pregnancy described implantation and development of a gestational sac in a bicornate or septate uterus. Today the term more broadly describes implantation in the myometrium of the horn (cornual region) of a normal uterus.1-4 Although cornual pregnancy is sometimes used interchangeably with interstitial pregnancy, the latter is distinguished by a gestational sac within the myometrium not specific to the cornual region.1-5 These constitute 2–4% of all ectopic pregnancies.5-9 Cornual pregnancy carries a 2.5% mortality rate but disproportionately accounts for 20% of maternal deaths from ectopic pregnancy.4,7,10
Compared to more common tubal pregnancies, the ability of the cornual uterine tissue to stretch allows pregnancies to progress undetected for weeks longer prior to rupture.4,9,11 Traditional ectopic pregnancy risk factors such as previous ectopic gravidity, pelvic inflammatory disease, fibroids, fallopian tube obstruction, and in vitro fertilization may be present but are largely absent in case series.3,4,7,8 Most ruptured cornual pregnancy patients complain of abdominal pain, but vaginal bleeding is less frequent than in other ectopic pregnancies, likely given the sequestered location.4,8,9 However, as pregnancy may progress as long as 12 weeks prior to rupture, women may present with hemorrhagic shock, confounding initial evaluation, differential considerations, and management.3,9,12
Cornual location within the interstitium can be confused with an uncomplicated intrauterine pregnancy on traditional two-dimensional US.4,13 A proposed, sonographic “interstitial line sign” extending from the upper region of the uterine horn to border the intramural portion of the fallopian tube has been described with high specificity but low sensitivity.7,13,14 Diagnostic criteria center on sonographic findings of an empty uterine cavity, a chorionic sac seen separately greater than one centimeter from the most lateral edge of the uterine cavity, and a thin myometrial layer surrounding the gestational sac.8,13,15 Like the interstitial line sign, these models demonstrate high specificity but low sensitivity of 40%.14 Radiologists and obstetricians advocate for three-dimensional US to improve diagnosis, as it can image the coronal plane of the uterus, although validation of increased accuracy is lacking.3,4,12,13
Suspicion of cornual pregnancy necessitates emergent obstetric consultation. Initial management focuses on stabilization and pregnancy confirmation. Unstable vital signs with free fluid on abdominal US should prompt consideration for blood product transfusion. In stable patients, early detection (βhCG < 3000 mIU/mL) of cornual pregnancy can be considered for outpatient methotrexate therapy, through oral, intramuscular, or sonographic-guided injection with obstetrics consultation.4,8,13 Most cited surgical cases are past this threshold, requiring either laparoscopic cornual resection or hysterectomy, although some are successfully treated with outpatient methotrexate.4-9,13
CONCLUSION
Given the difficulties in imaging and extended gestational age prior to diagnosis of cornual pregnancy, and high mortality rates, it is important that emergency clinicians be familiar with diagnostic pitfalls and treatment plans for management. Proper resuscitation and supportive care in the ED setting are essential, and immediate obstetric surgical consult is critical to limit catastrophic hemorrhage.
Footnotes
Section Editor: Austin Smith, MD
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
The authors wish to acknowledge the contributions of Peter Max Dodge in helping with reviewing the manuscript and refining the images for submission.
The authors attest that their institution requires neither Institutional Review Board approval nor patient consent for publication of this case report. Documentation on file.
Address for Correspondence: Brandon M. Carius, DSc, MPAS, PA-C, Brian D. Allgood Army Community Hospital, Department of Emergency Medicine, 3030 Gimlet Drive, Camp Humphreys, Republic of Korea, APO, AP 96273. Email: brian.m.carius.mil@mail.mil. 6:41 – 44
Submission history: Revision received August 10, 2021; Submitted October 18, 2021; Accepted October 22, 2021
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none. The views expressed here are those of the authors and do not reflect the official policy of the Department of the Army, the Department of Defense, or the U.S. Government.
REFERENCES
1. Arleo EK, DeFilippis EM. Cornual, interstitial, and angular pregnancies: clarifying the terms and a review of the literature. Clin Imaging. 2014;38(6):763-70.
2. Malinowski A, Bates SK. Semantics and pitfalls in the diagnosis of cornual/interstitial pregnancy. Fertil Steril. 2006;86(6):1764.e1711-64.
3. Valsky DV, Yagel S. Ectopic pregnancies of unusual location: management dilemmas. Ultrasound Obstet Gynecol. 2008;31(3):245-51.
4. Brincat M, Bryant-Smith A, Holland TK. The diagnosis and management of interstitial ectopic pregnancies: a review. Gynecological Surgery. 2019;16(1):2.
5. Marchand G, Taher Masoud A, Sainz K, et al. A systematic review and meta-analysis of laparotomy compared with laparoscopic management of interstitial pregnancy. Facts Views Vis Obgyn. 2021;12(4):299-308.
6. Ma K, Kaur N, Winters U. Cornuostomy and cornuectomy: laparoscopic management of interstitial ectopic pregnancies. J Minim Invasive Gynecol. 2020;27(7):1480-1.
7. Molinaro TA, Barnhart KT. Ectopic pregnancies in unusual locations. Semin Reprod Med. 2007;25(2):123-30.
8. MacRae R, Olowu O, Rizzuto MI, et al. Diagnosis and laparoscopic management of 11 consecutive cases of cornual ectopic pregnancy. Arch Gynecol Obstet. 2009;280(1):59-64.
9. Chan LY, Fok WY, Yuen PM. Pitfalls in diagnosis of interstitial pregnancy. Acta Obstet Gynecol Scand. 2003;82(9):867-70.
10. Tang A, Baartz D, Khoo SK. A medical management of interstitial ectopic pregnancy: a 5-year clinical study. Aust N Z J Obstet Gynaecol. 2006;46(2):107-11.
11. Surekha SM, Chamaraja T, Nabakishore SN, et al. A ruptured left cornual pregnancy: a case report. J Clin Diagn Res. 2013;7(7):1455-6.
12. Sargin MA, Tug N, Ayas S, et al. Is interstitial pregnancy clinically different from cornual pregnancy? A case report. J Clin Diagn Res. 2015;9(4):Qd05-06.
13. Dagar M, Srivastava M, Ganguli I, et al. Interstitial and cornual ectopic pregnancy: conservative surgical and medical management. J Obstet Gynaecol India. 2018;68(6):471-6.
14. Ackerman TE, Levi CS, Dashefsky SM, et al. Interstitial line: sonographic finding in interstitial (cornual) ectopic pregnancy. Radiology. 1993;189(1):83-7.
15. Timor-Tritsch IE, Monteagudo A, Matera C, et al. Sonographic evolution of cornual pregnancies treated without surgery. Obstet Gynecol. 1992;79(6):1044-9.