
{kind=link}
| Author | Affiliation |
|---|---|
| Mackensie Yore, MD, MS | VA Los Angeles and UCLA National Clinician Scholars Program, VA Greater Los Angeles Healthcare System HSR&D Center of Innovation, Los Angeles, California |
| Callan Elswick Fockele, MD, MS | University of Washington, Department of Emergency Medicine, Seattle, Washington |
| Herbert C. Duber, MD, MPH | University of Washington, Department of Emergency Medicine, Seattle, Washington |
| Kelly M. Doran, MD, MHS | NYU Grossman School of Medicine, Departments of Emergency Medicine and Population Health, New York, New York |
| Richelle J. Cooper, MD, MSHS | UCLA David Geffen School of Medicine, UCLA Department of Emergency Medicine, Los Angeles, California |
| Michelle P. Lin, MD, MPH, MS | Stanford University, Department of Emergency Medicine, Stanford, California |
| Steffani Campbell, MD, MPH | UCSF Fresno, Department of Emergency Medicine, Fresno, California |
| Vidya Eswaran, MD | Baylor College of Medicine, Department of Emergency Medicine and Section of Health Services Research, Department of Medicine, Houston, Texas |
| Betty Chang, MD, MHA | Columbia University, Department of Emergency Medicine, New York, New York |
| Haeyeon Hong, MD | Boston Medical Center, Department of Emergency Medicine, Boston, Massachusetts |
| Kessiena Gbenedio, MD | Columbia University, Department of Emergency Medicine, New York, New York |
| Kimberly A. Stanford, MD, MPH | University of Chicago, Section of Emergency Medicine, Chicago, Illinois |
| Nicholas Gavin, MD, MBA, MS | Mount Sinai Icahn School of Medicine, Department of Emergency Medicine, New York, New York |
Introduction
Methods
Results and discussion
Limitations
Conclusion
ABSTRACT
Introduction
Despite literature on a variety of social risks and needs screening interventions in emergency department (ED) settings, there is no universally accepted or evidence-based process for conducting such interventions. Many factors hamper or promote implementation of social risks and needs screening in the ED, but the relative impact of these factors and how best to mitigate/leverage them is unknown.
Methods
Drawing on an extensive literature review, expert assessment, and feedback from participants in the 2021 Society for Academic Emergency Medicine Consensus Conference through moderated discussions and follow-up surveys, we identified research gaps and rated research priorities for implementing screening for social risks and needs in the ED. We identified three main knowledge gaps: 1) screening implementation mechanics; 2) outreach and engagement with communities; and 3) addressing barriers and leveraging facilitators to screening. Within these gaps, we identified 12 high-priority research questions as well as research methods for future studies.
Results
Consensus Conference participants broadly agreed that social risks and needs screening is generally acceptable to patients and clinicians and feasible in an ED setting. Our literature review and conference discussion identified several research gaps in the specific mechanics of screening implementation, including screening and referral team composition, workflow, and use of technology. Discussions also highlighted a need for more collaboration with stakeholders in screening design and implementation. Additionally, discussions identified the need for studies using adaptive designs or hybrid effectiveness-implementation models to test multiple strategies for implementation and sustainability.
Conclusion
Through a robust consensus process we developed an actionable research agenda for implementing social risks and needs screening in EDs. Future work in this area should use implementation science frameworks and research best practices to further develop and refine ED screening for social risks and needs and to address barriers as well as leverage facilitators to such screening.
INTRODUCTION
Adverse social determinants of health, which encompass a host of socioeconomic and behavioral factors, are primary drivers of illness and injury.1 The set of adverse social factors linked to an individual’s poor health is referred to as their “social risk,” while their expressed priorities and desires for assistance addressing their social risks are collectively referred to as their “social need.”2,3
The emergency department (ED) provides a unique and important setting for social risks and needs screening and intervention to provide higher value care.4 Social risks and needs such as housing instability, food insecurity, lack of employment, substance use, and transportation barriers are prevalent in the ED patient population.5-9 Furthermore, approximately a quarter of adults in the United States lack a usual source of medical care.10 This group, particularly those uninsured or enrolled in Medicaid, often relies on the ED when health issues arise,11 highlighting a need for the ED to provide screening and resources that many patients are unable to access elsewhere. However, many factors affect the implementation of social risks and needs screening in the ED, including screening tool characteristics and deployment, stakeholder perspectives on screening, characteristics of the clinical, reimbursement, and regulatory environments, and the selected implementation strategies.12 The impact of these factors on screening implementation and uptake is inadequately characterized. A better understanding of the components and steps involved in implementing efficient and impactful ED-based social risks and needs screening programs could facilitate the uptake of this important tool for addressing the social determinants of health.
To spur research on ED-based social risks and needs screening, the 2021 Society for Academic Emergency Medicine (SAEM) Consensus Conference, “From Bedside to Policy: Advancing Social Emergency Medicine and Population Health through Research, Collaboration and Education” (“Consensus Conference”) developed a research agenda based on literature gaps, expert opinion, and stakeholder feedback comprising the following: 1) instruments for social risks and needs screening in the ED; 2) implementation of social risks and needs screening in the ED; and 3) interventions for patients with identified social risks and needs in the ED. Our goal in this article, the second of three manuscripts, was to describe consensus, process-derived research gaps and priorities related to implementation of social risks and needs screening in the ED setting.
METHODS
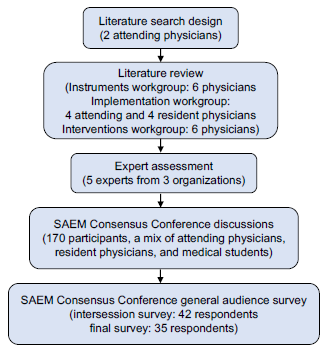
We identified research gaps and priorities for ED-based social risks and needs screening instruments, implementation, and interventions through a consensus-based approach, drawing on an extensive literature review, expert consultation, and feedback from Consensus Conference participants during moderated discussions and follow-up surveys (Figure 1).
Population Health Research Capsule
What do we already know about this issue?
The ED is an important setting for social risks/needs screening and intervention, yet factors affecting screening implementation are poorly characterized.
What was the research question?
What are the research gaps and priorities related to implementation of social risks/needs screening in the ED setting?
What was the major finding of the study? Major comparison with p-value and confidence interval
In a consensus process, we developed and ranked 12 research questions to address three social risks/ needs screening implementation knowledge gaps.
How does this improve population health?
We highlight research needed on the design, structure, and operationalization of ED social risks/needs screening to increase program sustainability and patient benefit.
Literature Review
A literature review on social risks and needs screening in the ED, adapted from methods used by Malecha et al5 and in consultation with a social sciences librarian, identified 2,085 articles covering screening tools, implementation, and/or interventions (Figure 2). Based on relevance of titles and abstract content, we selected 151 articles for detailed review. We found another 188 articles using the search term “emergency” in the Social Interventions Research & Evaluation Network (SIREN) Evidence and Resource Library13 and selected 22 for detailed review. Both searches were conducted in December 2020. Of the 173 articles identified for detailed review, 75 addressed implementation of ED screening, focusing on screening format and workflow, team structure, and barriers and facilitators to screening implementation.
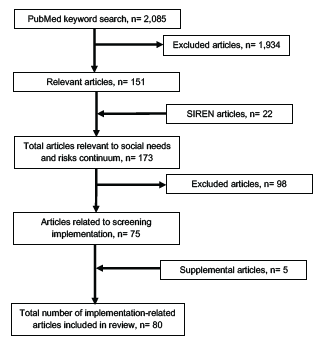
Finally, five additional articles from bibliographic references of the reviewed manuscripts were added to the literature review, based on their pertinence to ED screening implementation. A team of four attending and four resident physicians, all in Emergency Medicine, reviewed the 80 articles and extracted details into an Excel for Mac, version 16.52 (Microsoft Corp, Redmond, WA) database with information on study objective, design, outcomes, results, limitations, and quality. Our workgroup analyzed the extracted data and source manuscripts with the primary goals to identify research gaps and to subsequently draft research priorities.
Engagement and Feedback
We shared these draft research priorities with a panel of experts drawn from three organizations: the Office of the Assistant Secretary for Planning and Evaluation, a health policy-focused government agency14; Health Leads, a nonprofit organization connecting communities to social resources15; and SIREN, a program at the University of California San Francisco that researches healthcare sector strategies to address social conditions.13 We integrated feedback from these experts into a pre-reading document shared with Consensus Conference participants.
The SAEM Consensus Conference was held virtually using Zoom sessions (Zoom Video Communications, San Jose, CA) on April 13 and 27, 2021. The first session included a moderated discussion of methods, research gaps, and preliminary research priorities that incorporated expert feedback regarding the implementation of social risks and needs screening in the ED. After the first session, an intersession survey gathered feedback from the Consensus Conference participants, and this feedback was integrated into a revised set of research priorities. In the second session, moderated discussion further refined the priorities and ratings and resulted in a revised list of research priorities. In a final survey after the second session, participants ranked research priorities based on their perceived importance for future research and the SMART (specific, measurable, attainable, relevant, and time-based) criteria. Priorities were ranked using the following formula:
3
x
(
#
o
f
1
s
t
c
h
o
i
c
e
v
o
t
e
s
)
+
2
x
(
#
o
f
2
n
d
c
h
o
i
c
e
v
o
t
e
s
)
+
1
x
(
#
3
r
d
c
h
o
i
c
e
v
o
t
e
s
)
=
T
o
t
a
l
S
c
o
r
e
We categorized research priorities as high, medium, or low priority based on relative score (top ⅓, middle ⅓, lowest ⅓, respectively). Below, we present the research priorities pertaining to implementation of social risks and needs screening, grouped by thematic gaps identified during the literature review.
RESULTS AND DISCUSSION
Of the 80 articles reviewed, 10 were controlled clinical trials, including eight randomized controlled clinical trials, and five were prospective observational studies. Following the first moderated discussion, 31/32 survey respondents (96.8%) found that no additional priorities should be added to the research question list, and 28/32 (87.5%) recommended that no priorities be removed. Following the second Consensus Conference moderated discussion, 35 respondents completed the second survey, generating the final ranked list of research gaps and priorities, summarized in the Table and discussed in detail below.
| Question | Priority | Total points | Priority category | Gap addressed* | ||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | ||||
| How can EDs work effectively with and leverage existing expertise and resources of community organizations to optimize ED screening for social risk/needs? | 10 | 3 | 4 | 40 | High | OCE |
| What combination of interpersonal engagement and technology (eg, chatbots, kiosks, and EHR alerts and algorithms) in the screening process optimizes patient comfort disclosing their needs, maximizes efficiency, and facilitates successful referrals to community resources? | 3 | 11 | 1 | 32 | High | SIM |
| When should the screening be completed during the ED course? Where/how should it be done (eg, triage desk, registration, or alone in a treatment room; technology-assisted)? Where and with whom are results of screening discussed? | 7 | 3 | 4 | 31 | High | SIM |
| What are patient-, clinician-, and systems-level barriers to social risk/need screening in the ED? What strategies can be used to address the barriers to screening for social risk/needs in the ED? Do patient and clinician acceptability and accurate completion of screening improve when these barriers are addressed? | 3 | 7 | 2 | 25 | High | BFS |
| What is the ideal team structure and skill-mix of personnel for supporting screening in the ED? How might community health workers, trained peers, and/or health system navigators be incorporated into the screening process? | 2 | 2 | 4 | 14 | Medium | SIM |
| What is the comparative effectiveness of conducting a brief screening (eg, 1–2 items) for social risk/needs and then more detailed questions for those with potential risks/needs identified in the general screener versus starting with a more comprehensive screening for multiple discrete social risk/needs? | 3 | 1 | 2 | 13 | Medium | SIM |
| What is the “return on investment” for social risk/need screening in the ED, considering broadly defined “returns” as well as costs (including time and resources) in the ED? | 0 | 3 | 7 | 13 | Medium | BFS |
| How does the effectiveness of a given ED-based, social risk/need screening intervention vary across settings (ie, urban vs rural, academic vs community, and across multiple sites in general)? How can implementation of screening for social risk/needs be tailored based on setting to maximize effectiveness? | 4 | 0 | 0 | 12 | Medium | OCE |
| What strategies should be used to screen for social risk/needs among patients with psychiatric or high acuity presentations? Non-English-speaking patients? Undocumented patients? | 0 | 3 | 5 | 11 | Low | BFS |
| What is the comparative effectiveness and feasibility of strategies where interventions are triggered by positive social risk/need screening versus universal offers of social needs assistance to ED patients? | 2 | 0 | 2 | 8 | Low | SIM |
| What is the role of universal screening vs targeting certain patient groups (eg, patients with frequent ED visits)? | 1 | 1 | 1 | 6 | Low | SIM |
| What factors of the payment and policy landscape (eg, mandates and funding) encourage/incentivize or discourage EDs from implementing social risk/need screening? | 0 | 1 | 2 | 4 | Low | BFS |
*SIM, screening implementation mechanics (Gap 1); OCE, outreach and community engagement (Gap 2); BFS, barriers and facilitators to screening (Gap 3); ED, emergency department; EHR, electronic health record.
Gap 1: Screening Implementation Mechanics
Our literature review and Consensus Conference discussion identified several research gaps in the specific mechanics of screening implementation, including screening and referral team composition, workflow, and use of technology. Literature on social risks and needs screening describes the feasibility of, and potential concerns with, several team structures and workflows, including screening questions asked by ED staff (eg, registration clerk, nurse, social worker),16-20 completed independently by patients,16,18,21-27 or asked by external personnel (eg, patient navigator).25,26,28,29
Social risks and needs screening questions may be embedded in the electronic health record (EHR) and asked by ED staff in series with more conventional questions (eg, contact information, medical history, current symptoms).30 While this approach may integrate with the existing workflow and make use of staff already interacting with the patient, there may be a tendency by staff to rush or skip some questions given time constraints and the large volume of EHR prompts.23
Screenings completed independently by the patient often use electronic platforms such as tablets, kiosks, or chatbots.16,21,23-26,31,32 Such patient-facing, technology-based platforms can improve disclosure of risks/needs compared with face-to-face screening,18,21,27,33 especially in the ED waiting room and other spaces with limited privacy.2,18,34 Because these platforms do not require continuous staff time, screening can be more comprehensive, and patients have more autonomy over which questions to answer. Electronic screening can also automate referrals.28 Patient acceptance of self-facilitated, technology-based screening depends on patient age and screening topic; use of digital technologies is near-ubiquitous among adolescents,34 and most adolescents prefer technology-based screening for most social risk and need topics.
In 2000, increasing age was associated with lower acceptability of technology-assisted screening35; further studies could determine whether this sentiment persists and identify barriers to overcoming technological barriers among older adults. Another research gap is how technology might increase or impede screening accessibility for patients with vision or hearing impairments, limited English proficiency, and/or low health literacy. Furthermore, there is an opportunity for such research to include partnerships with patients in the co-design of accessible screening tools.
Several studies describe screening programs led by non-clinical staff and volunteers who can facilitate both screening and navigation to resources for identified needs (“patient navigator” model).36-39 Programs that specifically employ peer navigators and community health workers can incorporate community perspectives to better design screening programs, increasing patient comfort with disclosing needs, and empowering members of the community with new skills and opportunities.40 As with patient-completed questionnaires, screening not embedded within the EHR may lack EHR integration, and whether and how this information might be useful to clinicians and tracked over time is unstudied.
Consensus Conference participants broadly agreed that social risks and needs screening is generally acceptable to patients and clinicians and feasible in an ED setting. They therefore advocated that future research focus more on using best practices from quality improvement and implementation science to select and customize screening models to meet the needs of a local context, maximize the value of screening to patients and clinicians, and enable long-term sustainability of screening programs. For those new to quality improvement and implementation science, these practices may include using qualitative and quantitative methods to understand contextual factors and stakeholder perspectives, constructing testable theoretic and system models, and characterizing barriers and facilitators to initiating, scaling up, and sustaining screening.41-43 Additionally, researchers could plan experiments using one of many implementation research designs to evaluate screening deployment strategies through a combination of process and outcome metrics.44-46
Reflecting on the various models for screening, Consensus Conference participants expressed concern that screenings facilitated by overextended clinicians or nursing staff would be unsustainable regardless of buy-in and recommended research evaluating the screening by non-clinical staff (eg, peer navigators or college students) and/or training existing team members with nonclinical roles (eg, registration staff). Participants suggested clinicians would appreciate access to screening results even if they are less interested in doing the screening themselves. Participants recognized that many EDs have generally relied on social workers to address social needs of high-risk patients identified by clinicians and recommended that social workers be involved in the design and implementation of screening programs. Regardless of the screening model chosen, participants said it was essential for ED staff initiating or facilitating screening to understand and convey to patients the importance and utility of screening and demonstrate empathy throughout the process – an approach that may require additional training.
Research Priorities:
When should the screening be completed during the ED course? Where/how should it be done (eg, triage desk, registration, or alone in a treatment room; technology-assisted)? Where and with whom are the results of screening discussed?
What is the ideal team structure and skill-mix of personnel for supporting screening in the ED? How might community health workers, trained peers, and/or health system navigators be incorporated into the screening process?
What combination of interpersonal engagement and technology (eg, chatbots, kiosks, and EHR alerts and algorithms) in the screening process optimizes patient comfort disclosing their needs, maximizes efficiency, and facilitates successful referrals to community resources?
What is the comparative effectiveness of conducting a brief screening (eg, 1–2 items) for social risks/needs and then more detailed questions for those with potential risks/needs identified in the general screener versus starting with a more comprehensive screening for multiple discrete social risks/needs?
What is the comparative effectiveness and feasibility of strategies where interventions are triggered by positive social risks/needs screening versus universal offers of social needs assistance to ED patients?
What is the role of universal screening versus targeting certain patient groups (eg, patients with frequent ED visits)?
Gap 2: Outreach and Community Engagement
The literature includes numerous examples of engagement between social risks and needs screening programs and external agencies, including community-based organizations (CBOs) and referral agencies, especially for linking patients with resources.23,28,36,47-50 Relationships with referral agencies and CBOs have so far been useful for refining screening tools,23 evaluating referral success,49 and sharing patients’ experiences.50 However, we found no studies that directly involved patients or CBOs in the design of ED screening processes.
During the Consensus Conference, participants discussed community outreach and engagement to 1) enhance bidirectional communication with referral agencies, and 2) make screening processes more patient-centered. Participants thought community partners could help tailor screening processes to particular settings (eg, rural areas, language minorities) and advise on the timeline and manner of screening. Furthermore, it was thought that involving referral agencies in program design could help these agencies better anticipate increased demand following screening implementation and help tailor the screening process to better match agencies’ purpose and capacity.
While some Consensus Conference participants advocated for a community-based participatory research approach to developing and implementing ED social risks and needs screening, we found no studies using this approach. Through such an approach, representatives from socially vulnerable communities could lead design of screening interventions centered on patients’ priorities; gather screening information (eg, through a community health worker approach); recommend resources that are most useful and referral agencies that are most trusted among the community; review and contextualize aggregate results (eg, trends in screening, numbers and types of referrals to various kinds of resources with community partners); and help evaluate and improve the program.51,52
Research Priorities:
How can EDs work effectively with and leverage existing expertise and resources of community organizations to optimize ED screening for social risks/needs?
How does the effectiveness of a given ED-based social risk/needs screening intervention vary across settings (ie, urban vs rural, academic vs community, and across multiple sites in general)? How can implementation of screening for social risks/needs be tailored based on setting to maximize effectiveness?
Gap 3: Barriers and Facilitators to Screening
Our working group identified patient, personnel, system, and societal barriers to implementation of ED social risks and needs screening. Our literature review identified barriers and strategies to overcome these barriers and demonstrated research gaps that were further discussed and prioritized by Consensus Conference participants.
Patient-Related Barriers to Emergency Department Social Risks and Needs Screening
A variety of patient-related barriers to ED social risks and needs screening have been reported. Patient condition (eg, high-acuity illness, impairment) during the ED visit may limit screening of certain patients.53 Among patients able to be screened, those in hallway beds or other open areas may feel uncomfortable sharing screening information aloud.54 Others may be concerned about sharing information with unknown or untrusted referral organizations54 or triggering a report to Child Protective Services by disclosing certain risks (eg, intimate partner violence [IPV]).55 Furthermore, patients may decline screening due to disinterest in receiving resources.56 Factors that may facilitate screening in the ED include caring and empathetic interactions with screening staff, ability to immediately address identified needs,55 reassurance that screening will not delay care, assistance with screening technology, and observing that other patients are also screened.16 We found no studies that attempt to show the effect of addressing these barriers and facilitators on completion of screening, willingness to disclose risks and needs, or on accessing resources.
Consensus Conference participants described the lack of an ongoing patient-clinician relationship as a unique challenge for ED social risks and needs screening, highlighting a need for research to address which screening team structure (eg, clinical staff, peer navigators) is best for building trust to enable disclosure of social risks and needs and enable linkages to desired resources.
Personnel-Related Barriers to Emergency Department Social Risks and Needs Screening
Clinicians generally understand that social risks impact health,4 and most studies show clinical staff supporting the idea of screening 2,54,57 with greater support among physicians than nurses.31 Furthermore, attitudes toward screening can improve following implementation of screening programs.58 Clinical staff have also expressed reservations about screening, including a belief that screening is beyond their scope of practice,59,60 fear of offending patients,28,55,59,61,62 perceived or real lack of resources to address needs,55,62,63 and concern about disclosure increasing risk such as with IPV.59 In the case of IPV screening, however, evidence shows patient acceptability23,53,54 and satisfaction64 along with a single study finding no risk of violence with disclosure.65 Literature suggest several factors that may increase staff support for screening, including leveraging technology during screening60; selecting nurse champions to help direct implementation16; using a team approach to screening60; and ongoing staff engagement and feedback.16 Incentives for completing screening and disciplinary action for not screening have yielded mixed success,57,66 and staff-centered educational interventions alone to improve screening completion have shown limited efficacy.21,63
Consensus Conference participants noted that preparation for screening implementation often centered on training facilitators in content (eg, domestic violence, human trafficking), while insufficiently addressing critical system aspects such as funding, time, space, community engagement, and communication with referral agencies.
Systems-Related Barriers to Emergency Department Social Risks and Needs Screening
Our literature review identified multiple systems-level barriers to implementing social risk screening in the ED, including time constraints2,55,61,62,67,68; lack of established processes for addressing abuse16,67,69; and concern that screening may shift important ED resources away from acute care, lengthen ED stays, increase unreimbursed costs, and/or not be connected with appropriate interventions.70 Furthermore, while technology has the potential to make screening more efficient, certain “low-lift” technology strategies such as EHR alerts have not appreciably improved screening completion.17 Overall department culture and philosophy may also oppose social risk screening and challenge implementation.67
Consensus Conference participants noted that both rigorous quality improvement and implementation science begin with identifying local barriers to and facilitators for program success. Some participants recommended specific implementation frameworks, such as Exploration, Preparation, Implementation, and Sustainment71 and the Consolidated Frameworks for Implementation Research,12 as well as tools such as an Ishikawa diagram to identify factors within the local context contributing to efficient and accurate completion of screening and referral.72
Societal Barriers and the Payment/Policy Landscape
As insurance companies increasingly support value-based care, interest in addressing social determinants of health outside the hospital may increase. A current research gap is how payers and health systems can collaboratively address social risks and how to fairly attribute and compensate credit for successful interventions. We found no published literature evaluating the return on investment or cost-effectiveness for social risks screening in the ED, or on how incentives or mandates affect screening uptake. Participants identified incentives and regulation as critical to widespread implementation and called for rigorous studies (eg, multisite randomized control trials) demonstrating the ability for ED screening to ascertain and address patient social needs in order to justify these incentives and regulations.
Research Priorities:
What are patient-, clinician-, and systems-level barriers to social risks/needs screening in the ED? What strategies can be used to address the barriers to screening for social risks/needs in the ED? Do patient and clinician acceptability and accurate completion of screening improve when these barriers are addressed?
What is the “return on investment” for social risks/needs screening in the ED, considering broadly defined “returns” as well as costs (including time and resources) in the ED?
What strategies should be used to screen for social risks/needs among patients with psychiatric or high-acuity presentations? Non-English-speaking patients? Undocumented patients?
What factors of the payment and policy landscape (eg, mandates and funding) encourage/incentivize or discourage EDs from implementing social risk/need screening?
Types of Studies Needed
Consensus Conference discussions identified the need for studies using adaptive designs or hybrid effectiveness-implementation models to test multiple strategies for implementation and sustainability, in part to justify large-scale funding to make screening routine. Mixed-methods studies were also encouraged to show not just feasibility but how and why screening works and how these interventions can be sustained.
LIMITATIONS
This paper describes the series of activities leading to development of a research agenda on implementation of ED-based screening for social risks and needs as well as the research agenda itself. Although an extensive literature review was conducted at the beginning of this process, it was not designed as or intended to be a comprehensive systematic review. There is potential for omission of published or unpublished studies that might pertain to some of the research questions ultimately proposed. Furthermore, evidence was examined for quality, but no formal scoring with risk-of-bias tools was performed, as the goal was not to perform a systematic review but rather a focused, structured literature review to inform the consensus process. Another potential limitation is that the opinions and relative prioritization of research questions by the Consensus Conference participants could differ from opinions held by practitioners in the field more broadly.
CONCLUSION
This paper presents research gaps and priorities in implementing ED social risks and needs screening identified using an iterative, consensus-based approach involving an extensive literature review, expert assessment, and feedback from participants in the 2021 SAEM Consensus Conference. While there is much to learn about the efficiency and efficacy of different ED-based social risks and needs screening modalities, literature to date has shown that screenings are acceptable to patients and lead to their engagement with interventions.26,38,73 We highlight a need for more collaboration with various stakeholders in screening design and implementation. This engagement should be paired with rigorous evaluation of screening implementation processes to identify best practices, particularly for patients from diverse groups, ensuring that all patients receive evidence-based interventions to improve social risk and health outcomes.
Footnotes
Section Editor: Mandy J. Hill, DrPH, MPH
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Mackensie Yore, MD, MS, UCLA/VA National Clinician Scholars Program, 1100 Glendon Ave, Suite 900, Los Angeles, CA 90024, myore@mednet.ucla.edu 3 / 2023; 24:302 – 311
Submission history: Revision received May 7, 2022; Submitted November 7, 2022; Accepted October 6, 2022
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. No author has professional or financial relationships with any companies that are relevant to this study. There are no conflicts of interest or sources of funding to declare.
REFERENCES
1. McGinnis JM, Foege WH. Actual causes of death in the United States. JAMA. 1993;270(18):2207-12.
2. Samuels-Kalow M, Molina M, Ciccolo G, et al. Patient and community organization perspectives on accessing social resources from the emergency department: a qualitative study. West J Emerg Med. 2020;21(4):964-73.
3. Alderwick H, Gottlieb LM. Meanings and misunderstandings: a social determinants of health lexicon for health care systems. Milbank Q. 2019;97(2):407-19.
4. Gottlieb L, Fichtenberg C, Alderwick H, et al. Social determinants of health: What’s a healthcare system to do?. J Healthc Manag. 2019;64(4):243-57.
5. Malecha PW, Williams JH, Kunzler NM, et al. Material needs of emergency department patients: a systematic review. Acad Emerg Med. 2018;25(3):330-59.
6. Stevens TB, Richmond NL, Pereira GF, et al. Prevalence of nonmedical problems among older adults presenting to the emergency department. Acad Emerg Med. 2014;21(6):651-8.
7. Gerber E, Gelberg L, Rotrosen J, et al. Health-related material needs and substance use among emergency department patients. Subst Abus. 2020;41(2):196-202.
8. Molina MF, Li CN, Manchanda EC, et al. Prevalence of emergency department social risk and social needs. West J Emerg Med. 2020;21(6):152-61.
9. Sanjuan PM, Rice SL, Witkiewitz K, et al. Alcohol, tobacco, and drug use among emergency department patients. Drug Alcohol Depend. 2014;138:32-8.
10. Wolford ML, Stagnitti MN. Number of adult visits by characteristics of practices identified as usual source of care providers during 2016—Results from the MEPS Medical Organizations Survey. Available at: http://www.ncbi.nlm.nih.gov/books/NBK579997/. Accessed September 22, 2022.
11. Liaw W, Petterson S, Rabin DL, et al. The impact of insurance and a usual source of care on emergency department use in the United States. Int J Family Med. 2014;2014:842847.
12. Keith RE, Crosson JC, O’Malley AS, et al. Using the Consolidated Framework for Implementation Research (CFIR) to produce actionable findings: a rapid-cycle evaluation approach to improving implementation. Implement Sci IS. 2017;12(1):15.
13. Evidence & Resource Library | SIREN. Available at: https://sirenetwork.ucsf.edu/tools/evidence-library. Accessed October 29, 2021.
14. ASPE Homepage. Available at: https://aspe.hhs.gov/node/1. Accessed October 29, 2021.
15. Health Leads. Available at: https://healthleadsusa.org/. Accessed October 29, 2021.
16. Scribano PV, Stevens J, Marshall J, et al. Feasibility of computerized screening for intimate partner violence in a pediatric emergency department. Pediatr Emerg Care. 2011;27(8):710-6.
17. Olson L, Anctil C, Fullerton L, et al. Increasing emergency physician recognition of domestic violence. Ann Emerg Med. 1996;27(6):741-6.
18. Gottlieb L, Hessler D, Long D, et al. A randomized trial on screening for social determinants of health: the iScreen study. Pediatrics. 2014;134(6):e1611-8.
19. Gabrielian S, Chen JC, Minhaj BP, et al. Feasibility and acceptability of a colocated homeless-tailored primary care clinic and emergency department. J Prim Care Community Health. 2017;8(4):338-44.
20. Egyud A, Stephens K, Swanson-Bierman B, et al. Implementation of human trafficking education and treatment algorithm in the emergency department. J Emerg Nurs. 2017;43(6):526-31.
21. Rhodes KV, Lauderdale DS, He T, et al. “Between me and the computer”: Increased detection of intimate partner violence using a computer questionnaire. Ann Emerg Med. 2002;40(5):476-84.
22. Levas MN, Hernandez-Meier JL, Kohlbeck S, et al. Integrating population health data on violence into the emergency department: a feasibility and implementation study. J Trauma Nurs. 2018;25(3):149-58.
23. Karnitschnig L, Bowker S. Intimate partner violence screening in the emergency department: a quality improvement project. J Emerg Nurs. 2020;46(3):345-53.
24. Langerman SD, Badolato GM, Rucker A, et al. Acceptability of adolescent social and behavioral health screening in the emergency department. J Adolesc Health. 2019;65(4):543-8.
25. Kocielnik R, Agapie E, Argyle A, et al. HarborBot: a chatbot for social needs screening. AMIA Annu Symp Proc. 2019;2019:552-61.
26. Hassan A, Scherer EA, Pikcilingis A, et al. Improving social determinants of health: effectiveness of a web-based intervention. Am J Prev Med. 2015;49(6):822-31.
27. Cullen D, Blauch A, Mirth M, et al. Complete eats: summer meals offered by the emergency department for food insecurity. Pediatrics. 2019;144(4):e20190201.
28. Wallace AS, Luther B, Guo JW, et al. Implementing a social determinants screening and referral infrastructure during routine emergency department visits, Utah, 2017–2018. Prev Chronic Dis. 2020;17:E45.
29. Rumball-Smith J, Fromkin J, Rosenthal B, et al. Implementation of routine electronic health record-based child abuse screening in general emergency departments. Child Abuse Negl. 2018;85:58-67.
30. Clark CJ, Wetzel M, Renner LM, et al. Linking partner violence survivors to supportive services: impact of the M Health Community Network project on healthcare utilization. BMC Health Serv Res. 2019;19(1):479.
31. Robinson T, Bryan L, Johnson V, et al. Hunger: a missed opportunity for screening in the pediatric emergency department. Clin Pediatr (Phila). 2018;57(11):1318-25.
32. Trautman DE, McCarthy ML, Miller N, et al. Intimate partner violence and emergency department screening: computerized screening versus usual care. Ann Emerg Med. 2007;49(4):526-34.
33. Rhodes KV, Drum M, Anliker E, et al. Lowering the threshold for discussions of domestic violence: a randomized controlled trial of computer screening. Arch Intern Med. 2006;166(10):1107-14.
34. Ranney ML, Choo EK, Spirito A, et al. Adolescents’ preference for technology-based emergency department behavioral interventions: does it depend on risky behaviors?. Pediatr Emerg Care. 2013;29(4):475-81.
35. Dugaw JE, Civello K, Chuinard C, et al. Will patients use a computer to give a medical history?. J Fam Pract. 2000;49(10):921-3.
36. Bernstein J, Dorfman D, Lunstead J, et al. Reaching adolescents for prevention: the role of pediatric emergency department health promotion advocates. Pediatr Emerg Care. 2017;33(4):223-9.
37. Sandhu S, Xu J, Blanchard L, et al. A community resource navigator model: utilizing student volunteers to integrate health and social care in a community health center setting. Int J Integr Care. 2021;21(1):2.
38. Gottlieb LM, Hessler D, Long D, et al. Effects of social needs screening and in-person service navigation on child health: a randomized clinical trial. JAMA Pediatr. 2016;170(11):e162521.
39. Losonczy LI, Hsieh D, Wang M, et al. The Highland Health Advocates: a preliminary evaluation of a novel programme addressing the social needs of emergency department patients. Emerg Med J. 2017;34(9):599-605.
40. Greenwood-Ericksen M, DeJonckheere M, Syed F, et al. Implementation of health-related social needs screening at michigan health centers: a qualitative study. Ann Fam Med. 2021;19(4):310-7.
41. Margolis P, Provost LP, Schoettker PJ, et al. Quality improvement, clinical research, and quality improvement research—opportunities for integration. Pediatr Clin North Am. 2009;56(4):831-41.
42. Langley GJ, Moen R, Nolan KM, et al. Implementing a Change. The Improvement Guide: A Practical Approach to Enhancing Organizational Performance. 2009.
43. Campbell M, Fitzpatrick R, Haines A, et al. Framework for design and evaluation of complex interventions to improve health. BMJ. 2000;321(7262):694-6.
44. Hwang S, Birken SA, Melvin CL, et al. Designs and methods for implementation research: advancing the mission of the CTSA program. J Clin Transl Sci. ;4(3):159-67.
45. Moen RD, Nolan TW, Provost LP. Principles for Design and Analysis of Planned Experiments. Quality Improvement Through Planned Experimentation. 2012.
46. Speroff T, O’Connor GT. Study designs for PDSA quality improvement research. Qual Manag Health Care. 2004;13(1):17-32.
47. Hugl-Wajek JA, Cairo D, Shah S, et al. Detection of domestic violence by a domestic violence advocate in the ED. J Emerg Med. 2012;43(5):860-5.
48. Tiller J, Reynolds S. Human trafficking in the emergency department: improving our response to a vulnerable population. West J Emerg Med. 2020;21(3):549-54.
49. Gordon JA, Dupuie TA. Child health insurance outreach through the emergency department a pilot study. Acad Emerg Med. 2001;8(11):1088-90.
50. Rodriguez B, Mandich M. What victims of domestic violence experience in emergency departments; a cross sectional study. Arch Acad Emerg Med. 2019;7(1):e68.
51. Wallerstein N, Duran B. Community-based participatory research contributions to intervention research: the intersection of science and practice to improve health equity. Am J Public Health. 2010;100(S1):S40-6.
52. Israel BA, Schultz AJ, Parker EA, Becker AB, Allen AJ, Guzman R, Lichtenstein R. Critical Issues in Developing and Following CBPR Principles. Community-Based Participatory Research for Health: Advancing Social Health Equity. 2017:31-44.
53. Choo EK, Nicolaidis C, Jenkinson RH, et al. Failure of intimate partner violence screening among patients with substance use disorders. Acad Emerg Med. 2010;17(8):886-9.
54. Bair-Merritt MH, Mollen CJ, Yau PL, et al. Health care providers’ opinions on intimate partner violence resources and screening in a pediatric emergency department. Pediatr Emerg Care. 2006;22(3):150-3.
55. Dowd MD, Kennedy C, Knapp JF, et al. Mothers’ and health care providers’ perspectives on screening for intimate partner violence in a pediatric emergency department. Arch Pediatr Adolesc Med. 2002;156(8):794-9.
56. Marchis EHD, Hessler D, Fichtenberg C, et al. Assessment of social risk factors and interest in receiving health care–based social assistance among adult patients and adult caregivers of pediatric patients. JAMA Netw Open. 2020;3(10):e2021201.
57. Greenberg MR, Weinstock M, Fenimore DG, et al. Emergency department tobacco cessation program: staff participation and intervention success among patients. J Am Osteopath Assoc. 2008;108(8):391-6.
58. Quiñones-Rivera A, Wing HE, Barr-Walker J, et al. Provider impacts of socioeconomic risk screening and referral programs: a scoping review. J Am Board Fam Med. 2021;34(4):820-31.
59. Krimm J, Heinzer MM. Domestic violence screening in the emergency department of an urban hospital. J Natl Med Assoc. 2002;94(6):484-91.
60. Winfield L. Social determinants matter, but who is responsible? 2017 Survey of Physicians on Social Determinants of Health.
61. Wright RJ, Wright RO, Isaac NE. Response to battered mothers in the pediatric emergency department: a call for an interdisciplinary approach to family violence. Pediatrics. 1997;99(2):186-92.
62. McGrath ME, Bettacchi A, Duffy SJ, et al. Violence against women: provider barriers to intervention in emergency departments. Acad Emerg Med. 1997;4(4):297-300.
63. Daugherty J, Houry D. Intimate partner violence screening in the emergency department. J Postgrad Med. 2008;54(4):301.
64. McCaw B, Berman WH, Syme SL, et al. Beyond screening for domestic violence a systems model approach in a managed care setting. Am J Prev Med. 2001;21(3):170-6.
65. Houry D, Kaslow NJ, Kemball RS, et al. Does screening in the emergency department hurt or help victims of intimate partner violence?. Ann Emerg Med. 2008;51(4):433-42e7.
66. Larkin GL, Rolniak S, Hyman KB, et al. Effect of an administrative intervention on rates of screening for domestic violence in an urban emergency department. Am J Public Health. 2011;90(9):1444-8.
67. Hamberger LK, Rhodes K, Brown J. Screening and intervention for intimate partner violence in healthcare settings: creating sustainable system-level programs. J Womens Health (Larchmt). 2015;24(1):86-91.
68. Beach SR, Carpenter CR, Rosen T, et al. Screening and detection of elder abuse: research opportunities and lessons learned from emergency geriatric care, intimate partner violence, and child abuse. J Elder Abuse Negl. 2016;28(4–5):185-216.
69. Salhi BA, White MH, Pitts SR, et al. Homelessness and emergency medicine: a review of the literature. Acad Emerg Med. 2018;25(5):577-93.
70. Delgado MK, Acosta CD, Ginde AA, et al. National survey of preventive health services in us emergency departments. Ann Emerg Med. 2011;57(2):104-8e2.
71. Aarons GA, Hurlburt M, Horwitz SM. Advancing a conceptual model of evidence-based practice implementation in public service sectors. Adm Policy Ment Health. 2011;38(1):4-23.
72. Mackey KE, Bourn SS. Defining, measuring, and improving quality. Emergency Medical Services. 2015:509-16.
73. Walton MA, Chermack ST, Shope JT, et al. Effects of a brief intervention for reducing violence and alcohol misuse among adolescents: a randomized controlled trial. JAMA. 2010;304(5):527.