
{kind=link}
| Author | Affiliation |
|---|---|
| Louisa H. Schminke, MD | University of Bern, Department of Emergency Medicine, Bern, Switzerland |
| Victor Jeger, MD | University of Bern, Department of Emergency Medicine, Bern, Switzerland |
| Dimitrios S. Evangelopoulos, MD, PhD | University of Bern, Department of Emergency Medicine, Bern, Switzerland |
| Heinz Zimmerman, MD | University of Bern, Department of Emergency Medicine, Bern, Switzerland |
| Aristomenis K. Exadaktylos, MD | University of Bern, Department of Emergency Medicine, Bern, Switzerland |
ABSTRACT
Introduction:
About 10,000 escalator-related injuries per year result in emergency department treatment in the United States. Since the 1990s, a steady increase has been reported, but few statistics on escalator-related injuries have been published worldwide. We have therefore analyzed escalator accident statistics in admissions to our hospital in Switzerland since 2000.
Methods:
Using retrospective electronic patient chart analysis, we included in our study patients >16 years treated over an 11-year period. We categorized patients in terms of gender, age and associated risk factors, and classified accidents according to day, time, location and cause. Resulting trauma was categorized according to type and location. We divided post-admission treatment into surgical and conservative, and into treatment as an outpatient, in a short-stay unit, or as a hospital admission. Women and men were compared using Fisher’s exact test.
Results:
We identified 173 patients with 285 discrete injuries. Of these, 87 patients (50%) were women. Fifty-three (61%) of the women and 38 (44%) of the men were >60 years old (P = 0.033). Fifty percent of the men (43/86) of the men, but only 7% (6/87) of the women showed signs of alcohol intoxication (P < 0.0001). Accidents in women occurred predominantly on Tuesdays (19/87; 22%) between 12pmand 6pm (35/87; 40%), and in men on Saturdays (16/86; 19%) between 6pm and 12am (29/86; 34%; P = 0.0097). Sixty-two percent (44/71) of the accidents were in public transport facilities and 30% (21/71) in shopping centers. The majority of injuries in women were to the lower extremities (49/87; 56%), while most accidents in men were to the head and neck (51/86; 59%; P = 0.0052). About half (90; 52%) of the patients were treated conservatively. Almost half of all patients (76, 44%) required hospital admission. Of those, 45% left the hospital within 24 hours of admission (short stay unit) and 55% stayed longer than 24 hours.
Conclusion:
Escalator accidents can result in severe trauma. Significant gender differences in escalator accidents have been observed. Alcohol intoxication and age are significant risk factors in escalator-related accidents and might be possible targets for preventive measures.
INTRODUCTION
The first operational escalator was patented in 1892 and installed on Coney Island, New York, as an amusement ride. The device, however, was destined to serve as a serious means of transport.1,2Remarkably, wood was the key element in the construction of early escalator steps until metal took over in the 1920s, when the first escalator was installed in Germany.2–4 About 30 years later, in 1958, a department store in Basle was home to the first escalator in Switzerland.5
Today the escalator is everyday common means of transport. With a total length of 800 meters and a 24-hour transport capacity of 210,600 passengers, the longest outdoor escalator system in the world is used by more than 55,000 passengers in Hong Kong each day.6 The longest individual escalators can be found in St. Petersburg’s underground stations, comprising a length of around 142 meters at a height of 71 meters each.6
Because escalators are ubiquitous, it is, however, not surprising that they have also attracted negative attention as an accident location. In the United States (U.S.), about 10,000 escalator-related injuries requiring emergency department (ED) treatment are reported annually.7,8 The first reports of escalator-related injuries in Europe appeared in London in 1969.4 Twenty years later, 10 patients per month sought medical attention due to escalator accidents.9 In another study on escalator-related injuries, more than half happened in public transportation facilities and about 33% in shopping malls.10 There has recently been an increase in escalator-related accidents.11
Despite this increase in accidents and the possible severity of the resulting injuries only few statistics on escalator-related injuries have been published worldwide, mostly studies on children and case reports. In contrast, our study is a retrospective analysis with a broad patient age range and a long observation period. To our knowledge, this is the first study to analyze escalator-related accident patients admitted to a European Level I trauma center over an extended period. Our aim was to understand the character of escalator-related accidents and to identify risk factors and groups, in order to contribute to the development of effective preventive measurements.
METHODS
All data were collected prospectively, entered into our ED’s centralized electronic database (Qualicare, Switzerland) and analyzed retrospectively. We searched the database for patients presenting to our department (Emergency Department of Bern University Hospital, Level I trauma center) over an 11-year period (Feburary 2000-November 2011). The study comprises patients > 16 years, because at Bern University Hospital patients < 17 years are treated in the Department of Pediatrics.
We scanned patient reports electronically for the key word “escalator” (German “Rolltreppe”). Those containing the word “escalator” anywhere in the record were selected and reviewed twice by the authors AE and LS to ensure that they were escalator-related events.
We categorized patients by gender, age and associated risk factors (intoxication with alcohol or drugs, use of personal items on the escalator, e.g. luggage, pushchair). Age stratification was used to clarify the dependence of the incidence of escalator accidents on the age group. We classified each accident according to day, time, location and cause. The resulting trauma was categorized by type and location. We divided post-admission treatment into surgical, conservative, at the outpatient clinic, in a short-stay unit < 24 hours), or as hospital admission.
Dependent variables were patient age, associated risk factors, time of accident, location of injuries, type of therapy and type of patient management. Gender was the independent variable in our study.
We performed group comparisons with Fisher’s exact test. A P-value of < 0.05 was considered significant. We used Prism 5 (GraphPad Software Inc., La Jolla, California, U.S.) for statistical calculations.
Our study did not require institutional review board review.
RESULTS
One hundred seventy-three accidents in 173 patients were identified, 87 (50%) in women and 86 (50%) in men. Sixty-one percent (53/87) of the women and 44% (38/86) of the men were > 60 years (P = 0.033; Figure 1). Two fatalities occurred: cardiac event (prior to accident) and intracranial bleeding (result of accident).
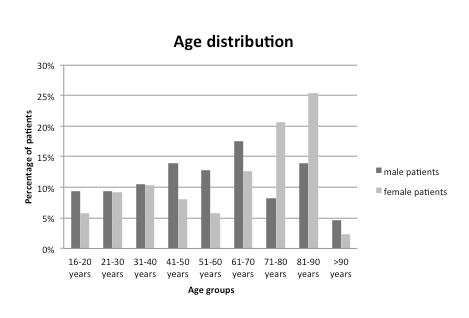
Distribution of age in men and women receiving emergency treatment for escalator-related injuries.
Our data demonstrated that 43/86 (50%) of the men and 6/87 (7%) of the women showed signs of alcohol intoxication (P < 0.0001; Figure 2). The majority of accidents were caused by slipping or falling (133; 77%). The next most frequent cause was fellow passengers (19; 11%). Twelve percent of the accidents had other causes (personal items, disregarding usage guidelines, or escalator malfunction: each < 6%). Gender differences for drug intoxication and the use of personal items were not statistically significant (Figure 2).
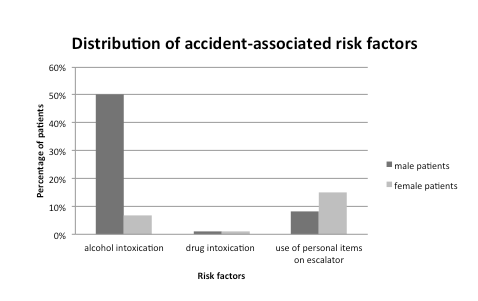
Distribution of accident associated risk factors in men and women receiving emergency treatment for escalator-rrelated injuries.
Accidents in women occurred mainly on Tuesdays (19/87; 22%), between noon and 6pm (35/87; 40%), while accidents in men occurred mainly on Saturdays (16/86; 19%) between 6pm and midnight (29/86; 34%; P = 0.0097). The accident location was known in 71 (41%) cases. Of those, 44 (62%) were public transport facilities and 21 (30%) shopping centers.
Two hundred eighty-five injuries were reported in 173 patients (Figure 3), with 160 soft tissue injuries seen in 160 (92%) patients, 76 fractures in 46 (27%) patients, 4 dislocations in 4 (2%) patients and 31 craniocerebral injuries in 31 (18%) patients (Figure 4). Fourteen injuries belonged to none of the categories mentioned above. The following types of fractures occurred: 18 (24%) skull/cervical fractures, 16 (21%) upper extremity fractures, 22 (29%) rib fractures, 5 (7%) hip fractures, and 15 (20%) lower extremity fractures. Of 4 dislocations, 2 involved the shoulder, 1 a facet joint of the cervical spine, and 1 of the teeth.

Distribution of injured body regions in men and women receiving emergency treatment for escalator-related injuries.

Distribution of injury types in men and women receiving emergency treatment for escalator-related injuries.
Craniocerebral injuries with cerebral bleeding occurred in 10 (6%) patients, requiring surgery in 2 patients and resulting in death in 1 patient. The majority of injuries in women were lower extremity injuries (49/87; 56%), whereas in men they involved the head and neck regions (51/86; 59%) (P = 0.0052; Figure 3). Multiple body regions were involved in 70 (40%) patients. Intracranial injuries were found in 31/85 (36%) and skull fractures in 17/85 (20%) of all head injuries.
The vast majority of patients (135, 78%) were transported to our trauma center by emergency medicine technicians. Thirty-eight (22%) patients were walk-ins (transport by foot or private transport).
Ninety patients (52%) were treated conservatively. No gender differences were observed. Of all surgical patients, 24/83 (29%) underwent surgery and 64/83 (77%) had surgical wound treatment. Almost half of all patients (76, 44%) were in need of hospital admission. Of those, 45% left the hospital within 24 hours of admission (short stay unit) and 55% stayed longer than 24 hours.
The majority of patients with soft tissue injuries (94 patients, 59%) were outpatients. Thirty-three (21%) patients with soft tissue injuries were admitted to our short stay unit and the same number to the hospital. In contrast, the majority of patients with fractures/dislocations (33 patients, 66%) were admitted to the hospital. Six (12%) patients with fractures/dislocations were admitted to our short stay unit and 11 (22%) were outpatients. Most patients with craniocerebral injuries (12 patients, 39%) stayed at out short stay unit. Almost the same numbers of patients with craniocerebral injuries were outpatients or were admitted to the hospital (9 and 10 patients, 29% and 32%, respectively).
DISCUSSION
The results of this study show that only about 1 percent of the patients at our Level I trauma center are victims of escalator-related accidents. In contrast to Chi et al12, Murphy and Moore9, and O’Neil et al13, we observed equal proportions of men and women, independent of age. O’Neil et al13analyzed only patients aged 65 and older, the majority of whom were women. In our study, the majority of patients older than 64 years were also women. This may be due to demographic factors.14,15 In addition, most escalator-related accidents are caused by falls, which occur more frequently in elderly women than in elderly men.9,12,13,16–18 Fifty percent of our patients were ≥ 65 years, which is consistent with demographic factors, given the fact that most escalator-related accidents were falls and that the rate of nonfatal injuries due to falls increases with age.19Additionally, the prevalence of fear of escalator use, the distress due to insecurity and the disrespect for safety rules increase with age.20
Our findings on alcohol consumption were consistent with those of Murphy and Moore.9 Almost one third of patients showed signs of alcohol influence, the large majority of whom were men.9 O’Farrell et al21 and Haberkern et al22 analyzed alcohol intoxication in Ireland and Switzerland and also identified a preponderance of men (70% and 60% respectively). Chi et al12 and O’Neil et al13 reported alcohol use in only 3% and < 1% of all cases, respectively. This might be explained by the national differences in alcohol consumption (Taiwan, U.S, Switzerland), by the age of the patients (> 64) in O’Neil et al’s23 study and by the very strict alcohol consumption laws in the U.S. We are aware of the fact that we only analyzed alcohol consumption in patients from one trauma center while other studies reported national data on alcohol consumption.
As far as the causes are concerned, the results of this study agree with those of Chi et al12 and O’Neil et al.13 Falls were the most common cause. Accidental falls have been reported to be the most common cause of nonfatal injury.17,18,24 In our study and in Chi et al’s12 study, around 10% of accidents were due to fellow passengers, in comparison with O’Neil et al’s13 figure of only 3 %. This might be because O’Neil et al13 included only patients > 64 years (frequency of falls increasing with age).13,25
An increased number of accidents was observed in women on Tuesdays and in men on Saturdays. As 50% of men in our study showed signs of alcohol intoxication and 36% of all male patients suffered from head/neck injuries under alcohol influence, we consider that our peak on Saturdays is consistent with the following studies: Puljula et al26 reported that alcohol-related head trauma in men occurred predominantly on Saturdays.27 In a study by O’Farrell et al21 most male alcohol intoxication patients presented to the ED on weekends. Furthermore, we identified a higher number of accidents in men between 6pm and midnight. A peak incidence at night has also been reported for fatal alcohol-related traffic accidents (77% at night, 22% during the day).28,29
The lower extremities and the head were the most frequently injured regions. Most injuries in women involved the lower extremities and in men the head or neck. We interpret our high proportion of head and neck injuries in men as being associated with alcohol intake, for the following reasons. We found a high proportion of men under alcohol influence (50%) and calculated that the risk for head trauma under alcohol intoxication was much higher than that for other types of trauma under alcohol intoxication (73% versus ≤ 30%). Savola et al30 also reported a strong preponderance of head injuries over other injury types in alcoholically intoxicated patients.
Soft tissue injuries were the major injury type, followed by fractures or dislocations and craniocerebral injuries. The majority of head injuries in our patients, however, were soft tissue injuries. We believe that these injuries are correlated with the escalator design.31
In our study, almost half of all patients were in need of hospital admission, of whom 55% stayed longer than 24 hours. We had fewer outpatients (56%) than O’Neil et al13 (92%) or Murphy and Moore9 (84%), possibly because many patients used our short stay unit (stay < 24 hours). These patients may not have been immediately discharged due to alcohol intoxication or their distance from home. Our study did not cover cost or length of stay.
LIMITATIONS
This analysis is based on records from a single trauma center and may not be representative on a national level. Furthermore, data were retrieved from the narrative section of patient reports. This information may be poorly formulated, so that there may be gaps in the data or misinterpreted data.
CONCLUSION
Escalator-related accidents can cause significant medical consequences. Even though most patients suffered soft tissue injuries, many suffered severe injuries, injuries to multiple body parts, or had to be admitted to the hospital or undergo surgery. There were even 2 fatalities.
The identification of risk factors or groups at risk might support the development of preventive measures. Age and alcohol intoxication were the major risk factors identified. Furthermore, we found significant gender differences for the risk factors age and alcohol intoxication, as well as for the time of accident and injury location. Consequently, 2 risk groups were identified: Elderly women and men < 60 under the influence of alcohol. The risk factor of age may increase with the aging of the population; perhaps courses for elderly passengers might be introduced in the correct use of escalators. The risk factor of alcohol intoxication might be addressed by limiting escalator use for those under the influence of alcohol, with punishment if this was disregarded.
Our study is a retrospective analysis with a patient sample from 1 Swiss Level I trauma center. In order to better characterize the emerging public health risk of escalator use, additional information would be desirable – ideally from a prospective study for the whole of Switzerland.
Footnotes
Supervising Section Editor: Bharath Chakravarthy, MD, MPH
Submission history: Submitted March 11, 2012; Revision received August 27, 2012; Accepted December 5, 2012
Full text available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2012.12.13346
Address for Correspondence: Dimitrios S. Evangelopoulos, MD, PhD, Department of Emergency Medicine, Inselspital, University of Bern, Bern, Switzerland. Email: ds.evangelopoulos@gmail.com.
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. The Elevator Museum Available at: http://www.theelevatormuseum.org/. Accessed January 25, 2012.
2. Otis Elevator Company Available at: http://www.otisworldwide.com/pdf/AboutEscalators.pdf. Accessed on January 30, 2012.
3. Spiegel Online. Available at:http://einestages.spiegel.de/static/topicalbumbackground/4281/kathedralen_des_kaufrauschs.html. Accessed January 30, 2012.
4. Khalil PN, Huber-Wagner S, Kanz KG, et al. Rolltreppenstürze und ihre Folgen: Worauf müssen Sie achten? MMW Fortschr Med. 2008;150:38–40. [PubMed]
5. Lienhard JP. Webjournal.ch – Literaturhaus à L Alsacienne.“ Webjournal.ch. Available at:http://www.webjournal.ch/article.php?article_id=829. Accessed January 28, 2012.
6. Sustainable Cities TM Available at: http://sustainablecities.dk/en/city-projects/cases/hong-kong-re-discovering-escalators-as-public-transport). Accessed January 25, 2012.
7. McCann M, Zaleski N. Electronic Library of Construction Occupational Safety and Health. Deaths and Injuries Involving Elevators and Escalators. 2006. Available athttp://www.elcosh.org/record/document/405/d000397.pdf. Accessed January 25, 2012.
8. United States Consumer Product Safety Commission Available at:http://www.cpsc.gov/cpscpub/prerel/prhtml08/08264.html. Accessed January 25, 2012.
9. Murphy JP, Moore FP. Escalator injuries. Injury. 1992;23:336–38. [PubMed]
10. Austrian Road Safety Board (KFV) Available at:http://www.kfv.at/kfv/landesstellen/tirol/presse/presse-details-tirol/artikel/2354/. Accessed January 25, 2012.
11. Rochowansky T. Mehr Sicherheit Bei Aufzügen Und Fahrtreppen in Österreich. Available at:http://www.ots.at/presseaussendung/OTS_20070221_OTS0053/mehr-sicherheit-bei-aufzuegen-und-fahrtreppen-in-oesterreich. Accessed January 30, 2012.
12. Chi CF, Chang TC, Tsou CL. In-depth investigation of escalator riding accidents in heavy capacity MRT stations. Accident Anal. Prevent. 2005;38:662–670. [PubMed]
13. O’Neil J, Steele GK, Huisingh C, et al. Escalator-related injuries among older adults in the United States, 1991–2005. Accid Anal Prev. 2008;40:527–533. [PubMed]
14. United States Census Bureau Available at:http://www.census.gov/prod/cen2010/briefs/c2010br-03.pdf. Accessed on February 3rd 2012.
15. Swiss Federal Statistical Office Available at: http://www.pxweb.bfs.admin.ch/Dialog/varval.asp?ma=px-d-01-2A02&path=../Database/German_01%20-%20Bev%F6lkerung/012%20-%20Bev%F6lkerungsstand%20und%20-bewegung/&lang=1&prod=01&openChild=true&secprod=2. Accessed February 4, 2012.
16. Centers for Disease Control and Prevention Available at:http://www.cdc.gov/HomeandRecreationalSafety/Falls/adultfalls.html. Accessed February 3, 2012.
17. Centers for Disease Control and Prevention, web -based Injury Statistics Query and Reporting System (WISQARS) Available at: http://www.cdc.gov/injury/wisqars/. Accessed February 4, 2012.
18. Statistics Canada Available at: http://www.statcan.gc.ca/pub/82-625-x/2010002/article/11272-eng.htm. Accessed February 5, 2012.
19. http://www.healthyagingprograms.org/resources/FallsFreeReviewPaperFinal.pdf. Accessed February 5, 2012.
20. Swiss Council for Accident Prevention Available at:http://www.bfu.ch/German/forschung/Forschungsergebnisse/pdfForschungergebnisse/Reports/zusammenfassungen/Pilot_9707_Zsfg.pdf,bfu. Accessed February 6, 2012.
21. O’Farrell A, Allwright S, Downey J, et al. The burden of alcohol misuse on emergency in-patient hospital admissions among residents from a health board region in Ireland. Addiction.2004;99:1279–1285. [PubMed]
22. Haberkern M, Exadaktylos AK, Marty H. Alcohol intoxication at a university hospital acute medicine unit with special consideration of young adults: an 8-year observational study from Switzerland. Emerg Med J. 2010;27:199–202. [PubMed]
23. World Health Organization Available at:http://www.who.int/substanceabuse/publications/globalalcoholreport/msbgsruprofiles.pdf. Accessed February 3, 2012.
24. Clinical Excellence Commission, The NSW Falls Prevention Program Available at:http://www.cec.health.nsw.gov.au/programs/falls-prevention. Accessed on February 5th 2012.
25. WHO Global Report on Falls Prevention in Older Age, 2007 Available at:http://www.who.int/ageing/publications/Fallsprevention7March.pdf. Accessed February 5, 2012.
26. Puljula J, Savola O, Tuomivaara V, et al. Weekday distribution of head traumas in patients admitted to the emergency department of a city hospital: effects of age, gender and drinking pattern.Alcohol Alcohol. 2007;42:474–479. [PubMed]
27. Nova Scotia Health Promotion and Protection Available at:http://www.gov.ns.ca/hpp/publications/seniorsfalls.pdf. Accessed February 3, 2012.
28. National Institute of Alcohol Abuse and Alcoholism Available at:http://pubs.niaaa.nih.gov/publications/arh27-1/63-78.htm. Accessed February 5, 2012.
29. National Highway Traffic Safety Administration Available at:http://www.nhtsa.gov/DOT/NHTSA/Traffic%20Injury%20Control/Articles/Associated%20Files/811175.pdf. Accessed February 6, 2012.
30. Savola O, Niemela O, Hillbom M. Alcohol intake and the pattern of trauma in young adults and working aged people admitted after trauma. Alcohol Alcohol. 2005;40:269–273. [PubMed]
31. Bakken GM, Harvey CH, Hyde AS, et al. Falls and Related Injuries: Slips, Trips, Missteps and Their Consequences. 2nth ed. Tucson: Lawyers & Judges Publishing Company; 2007. p. 220.