
{kind=link}
| Author | Affiliation |
|---|---|
| Eric Silman | Department of Emergency Medicine, University of California Irvine School of Medicine |
| Mark I. Langdorf, MD, MHPE | Department of Emergency Medicine, University of California Irvine School of Medicine |
| Scott Rudkin, MD, MBA | Department of Emergency Medicine, University of California Irvine School of Medicine |
| Shahram Lotfipour, MD, MPH | Department of Emergency Medicine, University of California Irvine School of Medicine |
An 11-month-old Hispanic male was brought to the emergency department (ED) by paramedics after being struck in his stroller by a full-size pickup truck. Witnesses told medics on the scene that the stroller was pushed 20 feet but did not tip over, and the patient was not ejected. The patient’s mother was also struck and sustained an ankle fracture. At the scene the patient was alert with stable vital signs and no visible injuries. The stroller was noted by the paramedics to be extensively damaged. On arrival in the ED the patient’s vital signs were stable and exam revealed no signs of external trauma or neurologic deficits. CT of the head and neck was normal, but the patient was admitted for observation due to the presumed serious mechanism of injury and uncertain history. Six hours after admission the patient was unable to move his lower extremities, and lower extremity sensation was significantly decreased. MRI revealed significant spinal cord contusion and hemorrhage from C7 to T1, as well as ventral subdural hemorrhage from C2 through C7, and evidence of interspinous ligament rupture between C5 and C6. Neurosurgery treated the injuries non-operatively and the patient remained paraplegic.
Due to the inherent flexibility of the pediatric cervical spine and supporting ligaments, blunt trauma may cause significant spinal cord injury without visible fracture or dislocation. Spinal cord injury without radiographic abnormality (SCIWORA) is defined as any objective signs of myelopathy as a result of trauma in the presence of normal radiographs.1 This relatively rare but devastating pattern of injury was originally described in children by Pang and colleagues in 1982. Children with SCIWORA experience delayed onset of neurologic deficits, sometimes up to four days after the initial injury, and generally have poor outcomes. Recently the NEXUS study group prospectively identified 27 adult patients with SCIWORA (0.08% of the total 34,069 patients enrolled), but none of the over 3,000 children enrolled had SCIWORA.2
Despite its low incidence, SCIWORA remains a concern in any pediatric blunt trauma patient with delayed onset of neurologic signs or symptoms, and urgent MRI is indicated. This case also illustrates the importance of a thorough and accurate history from medics and witnesses in cases of pediatric trauma, where the patient (and often the parents) may provide incomplete or inaccurate information.
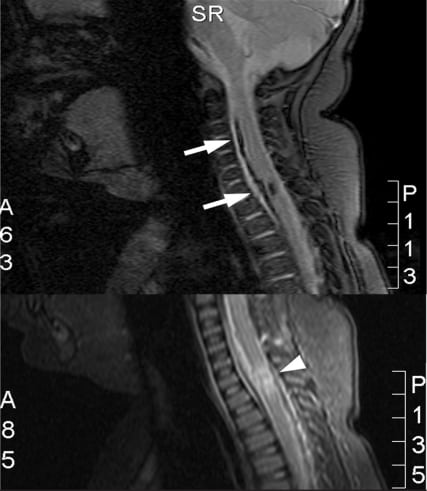
Upper plate, T1-weighted image showing anterior subdural hemorrhage from C2 to C7 (arrows). Lower plate, T2-weighted image showing extensive cord hemorrhage between C7 and T1.
Footnotes
Supervising Section Editor: Sean O. Henderson, MD
Submission history: Submitted January 14, 2008; Revision Received February 17, 2008; Accepted February 22, 2008
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Shahram Lotfipour, MD, MPH. Department of Emergency Medicine, University of California Irvine School of Medicine, 101 The City Dr., Orange, CA 92868
Email: SHL@uci.edu
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Pang D, Wilberger JE., Jr Spinal cord injury without radiographic abnormalities in children. J Neurosurg. 1982;57:114–29. [PubMed]
2. Hendey GW, Wolfson AB, Mower WR, Hoffman JR. Spinal cord injury without radiographic abnormality: results of the National Emergency X-Radiography Utilization Study in blunt cervical trauma. J Trauma. 2002;53:1–4. [PubMed]