
{kind=link}
| Author | Affiliation |
|---|---|
| Sean Patrick Nordt, MD, PharmD | University of Southern California, Department of Emergency Medicine, Los Angeles, California |
| Christopher Bowns, MD | Los Angeles County + University of Southern California Medical Center, Department of Emergency Medicine, Los Angeles, California |
| Julieta Moran, MD | Los Angeles County + University of Southern California Medical Center, Department of Emergency Medicine, Los Angeles, California |
| H. Brendan Kelleher, MD | Los Angeles County + University of Southern California Medical Center, Department of Emergency Medicine, Los Angeles, California |
| Stuart Swadron, MD | University of Southern California, Department of Emergency Medicine, Los Angeles, California |
ABSTRACT
We present a case of acute appendicitis from mobile cecum presenting with left upper quadrant abdominal pain.
A 58-year-old male with history of hypertension presented with constant left upper quadrant (LUQ) pain for 3 days. He denied fevers, chills, had no anorexia or association with eating, and no changes in bowel or bladder function. He was nontoxic appearing with normal vital signs. Abdomen was soft with tenderness to palpation in LUQ with normal bowel sounds. There were no masses, guarding, or other areas of tenderness. Remainder of the examination was normal. White blood count was 10,600/mm3 with 74.9% neutrophils with otherwise normal indices. Serum chemistry, urinalysis, and liver function tests, including lipase, were all in normal range. C-reactive protein (CRP) was 217 mg/L (reference range: 0–7 mg/L). A computerized tomography (CT) with intravenous contrast was obtained.
Diagnosis: Left-sided Appendicitis
The CT demonstrated a mobilized mesocecum in the left upper quadrant with a large, inflamed thick-walled appendix consistent with acute appendicitis. He underwent a laparotomy. The colon and cecum were found in the left upper quadrant with an inflamed, enlarged appendix. No malrotation or other congenital abnormalities were seen. Histology demonstrated a gangrenous appendix. He tolerated surgery well and was discharged home two days later.
Left-sided acute appendicitis is predominantly seen with congenital anomalies, e.g., situs inversus totalis and midgut malrotation.1 The majority of these present with left lower quadrant pain.1 The patient presented had LUQ pain due to a hypermobile colon. Though not specific, an elevated CRP has been suggested as a marker of acute appendicitis.2 The elevated CRP and clinical concern led to obtaining the CT.
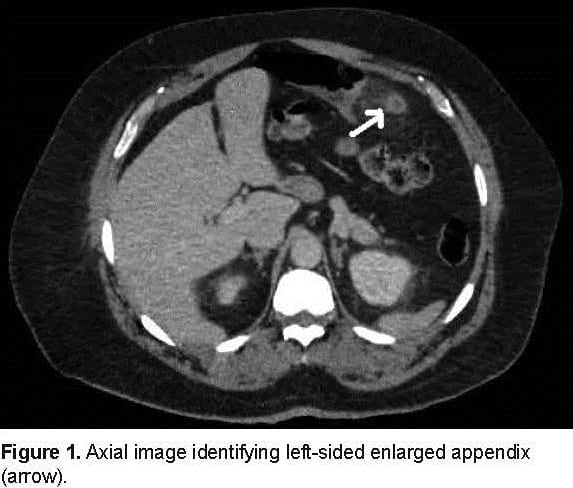
Axial image identifying left-sided enlarged appendix (arrow).
.")
Coronal image identifying left upper quadrant acute appendicitis (arrow).
Footnotes
Supervising Section Editor: Sean O. Henderson, MD
Submission history: Submitted January 10, 2012; Accepted March 8, 2012
Full text available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2012.1.11737
Address for Correspondence: Sean Patrick Nordt, MD, PharmD, Deparment of Emergency Medicine, University of Southern California, 1200 North State Street, Unit 1, Room 1011, Los Angeles, CA 90033
Email: spnordt@hotmail.com
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Akbulut S, Ulku A, Senol A, et al. Left-sided appendicitis: review of 95 published cases and a case report. World J Gastroeterol. 2010;16:5598–5602.
2. Andersson REB. Meta-analysis of the clinical and laboratory diagnosis of appendicitis.Br J Surg. 2004;2004:28–37. [PubMed]