
{kind=link}
| Author | Affiliation |
|---|---|
| Curt Canine, DO, MS | Carl R Darnall Army Medical Center, Department of Emergency Medicine, Fort Hood, Texas |
| Lawrence Masullo, MD | Carl R Darnall Army Medical Center, Department of Emergency Medicine, Fort Hood, Texas |
CASE PRESENTATION
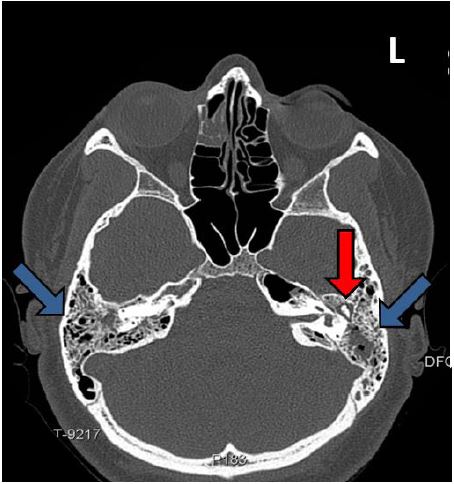
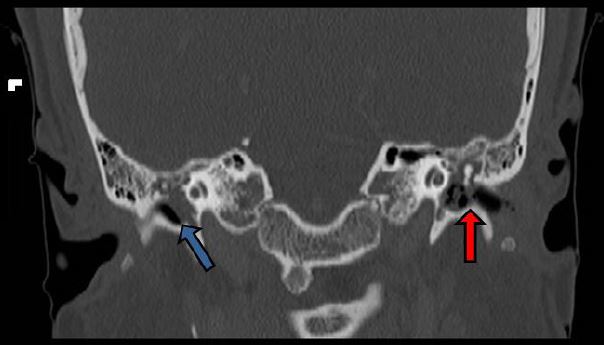
A 23-year-old female presented to the emergency department five weeks post-partum for headache, severe bilateral ear pain, and left ear drainage. Seven days prior she had been diagnosed with left otitis externa. Despite ofloxacin otic drops, pain progressed to involve both ears and became exacerbated by mastication or head rotation. Physical exam revealed right tympanic membrane (TM) erythema and bulging with purulent effusion; left TM completely obscured by swelling of the external auditory canal with seropurulent drainage present; moderate tenderness overlying bilateral mastoid processes; and severe pain on movement of the left ear helix. Leukocyte count (15.3 109/L; 81% neutrophils), and computed tomography (CT) were obtained (Images 1 and 2).
DIAGNOSIS
Acute bilateral mastoiditis
Acute mastoiditis (AM) is a rare but dangerous complication of otitis media (OM) with incidence of less than one per year per 100,000, primarily affecting children (median age 2.5 years)1,2,3,4,5 Bilateral AM is uncommon in children (0.3% of all AM cases), but has not been reported in healthy adults. Neither has postpartum AM been described. No CT images of AM in adults have been published. The aditus ad antrum is an anatomic connection between the middle ear and the mastoid antrum. Blockage, typically a result of swelling, traps infectious material in the antrum and prevents re-aeration. Causative organisms are similar to acute OM, including Streptococcus pneumoniae (most common), Group A streptococcus, Staphylococcus aureus, and Haemophilus influenza.2,3,4,6
The mastoid air cells are in close proximity to the posterior cranial fossa, lateral sinuses, facial nerve canal, semicircular canals, and the petrous tip of the temporal bone. Erosions and coalescence of air cells can cause temporal lobe abscess, lateral sinus septic thrombosis, facial nerve palsy, or meningitis.7,8,9 Ceftriaxone and vancomycin were administered intravenously to the patient, and she was admitted to medicine. Ear, nose and throat consult recommended amoxicillin clavulanate and ciprofloxacin/dexamethasone ear drops. Symptoms and exam were improved at follow-up four days later.
CPC-EM Capsule
What do we already know about this clinical entity?
Mastoiditis is uncommon, affecting mostly children. Bilateral disease has not been reported in healthy adults, but may cause abscess or meningitis.
What is the major impact of the image?
Emergency clinicians should recognize historical and physical exam features of mastoiditis and have an appreciation of radiographic findings to expedite definitive treatment of the patient.
How might this improve emergency medicine practice?
The images serve as a primer for recognition of mastoiditis, and remind the emergency provider that otitis externa is not always a benign process, but may progress to more serious disease.
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Address for Correspondence: Curt Canine, DO, MS, Carl R Darnall Army Medical Center, 36065 Santa Fe, Room 41-114 Fort Hood, TX 76544-5095. Email: Curt.R.Canine.mil@mail.mil. 1:433 – 434
Submission history: Revision received April 30, 2017; Submitted July 7, 2017; Accepted July 11, 2017
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. Dr. Canine is active duty with the U.S. Army, but received no special funding for this work or submission. No other conflicts to report for Dr. Canine or Dr. Masullo. The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or reflecting the views of the Department of the Army or the Department of Defense.
REFERENCES
1. Leskinen K, Jero J. Acute complications of otitis media in adults. Clin Otolaryngol. 2005;30(6):511-6.
2. Vassbotn FS, Klausen OG, Lind O, et al. Acute mastoiditis in a Norwegian population: a 20 year retrospective study. Int J Pediatr Otorhinolaryngol. 2002;62(3):237-42.
3. Palma S, Bovo R, Benatti A, et al. Mastoiditis in adults: a 19-year retrospective study. Eur Arch Otorhinolaryngol. 2014;271(5):925-31.
4. Stenfeldt K, Hermansson A. Acute mastoiditis in southern Sweden: a study of occurrence and clinical course of acute mastoiditis before and after introduction of new treatment recommendations for AOM. Eur Arch Otorhinolaryngol. 2010;267(12):1855-61.
5. Groth A, Enoksson F, Hultcrantz M, Stalfors J, Stenfeldt K, Hermansson A. Acute mastoiditis in children aged 0–16 years–a national study of 678 cases in Sweden comparing different age groups. Int J Pediatr Otorhinolaryngol. 2012;76(10):1494-500.
6. Minovi A, Dazert S. Diseases of the middle ear in childhood. GMS Curr Top Otorhinolaryngol Head Neck Surg. 2014;13.
7. Van Munster MP, Brus F, Mul D. Rare but numerous serious complications of acute otitis media in a young child. BMJ Case Rep. 2013.
8. Maranhão A, Andrade J, Godofredo V, et al. Epidemiology of intratemporal complications of otitis media. Int Arch Otorhinolaryngol. 2014;18(2):178-83.
9. Grafstein E, Fernandes CM, Samoyloff S. Lateral sinus thrombosis complicating mastoiditis. Ann Emerg Med. 1995;25(3):420-3.