
{kind=link}
| Author | Affiliation |
|---|---|
| Aaron Birch, MD | Madigan Army Medical Center, Department of Emergency Medicine, Tacoma, Washington |
| Ryan Walsh, MD | Madigan Army Medical Center, Department of Emergency Medicine, Tacoma, Washington |
| Diane Devita, MD | Madigan Army Medical Center, Department of Emergency Medicine, Tacoma, Washington |
ABSTRACT
Since the first description of the Chance fracture in 1948, there have been few case reports of unique mechanisms causing this classical flexion-extension injury to the spine in motor vehicle accidents, sports injury, and falls. To our knowledge, this injury has not been reported from a fall with the mechanistic forces acting laterally on the spine and with spinal support in place. We present a 21-year-old male who slid down a flight of stairs onto his side wearing a heavy mountaineering style backpack, subsequently sustaining a Chance fracture of his first lumbar vertebrae.
INTRODUCTION
Chance fractures are seen usually as the result of flexion-extension injury, most notably during motor vehicle collisions with the advent of lap seatbelts. Case reports have also been reported from an individual who fell 20 feet landing on his feet with forward flexion, an adolescent female who fell from height, and a 25-year-old snowboarder following a backwards fall.1–3 To our knowledge, this is the first reported case of a Chance fracture sustained after falling onto and subsequently sliding down a flight of stairs.
CASE REPORT
We present a 21-year-old male with no significant past medical history who presented to the emergency department (ED) after a fall down approximately 10 stairs. The patient reported he was wearing a heavy mountaineering style backpack when he tripped, fell onto the side of his low back and then slid down the stairs. On initial presentation, he complained of severe pain to his low back. The patient was deemed reliable, without any propensity for dishonesty or malingering, and there was no identifiable recompense or profitable gain other than correcting his condition.
Physical exam showed normal vital signs and no external evidence of trauma with midline point tenderness from his mid-thoracic to lumbar spine without crepitus. A neurologic exam was normal to include full range of motion and sensation to both his lower extremities with normal rectal tone and no saddle anesthesia. Cervical, thoracic, and lumbar spine radiographs were obtained, which were significant for mild anterior wedging of the first lumbar (L1) vertebrae of uncertain chronicity. The patient’s pain was resolved after morphine 12mg IV and ketorolac 30 mg IV. After a period of observation, he was found to be ambulatory and was therefore discharged home with oxycodone/acetaminophen, 72-hour primary care follow-up, and strict return precautions.
The patient returned 30 hours after discharge with continued severe low-back pain that was unrelieved with the prior pain medications. His exam was unchanged from the prior ED visit with normal vital signs. During this visit a magnetic resonance image of the lumbar spine was obtained which revealed a Chance fracture involving the body of L1 extending into the pedicle with probable pars interarticularis involvement without cord compression (Figure 1). Neurosurgery was consulted, and the patient was initially treated by conservative medical management with a thoracolumbar spinal orthosis, and later taken to the operating room for postero-lateral fusion of T12-L2. He was discharged after 7 days in good condition.
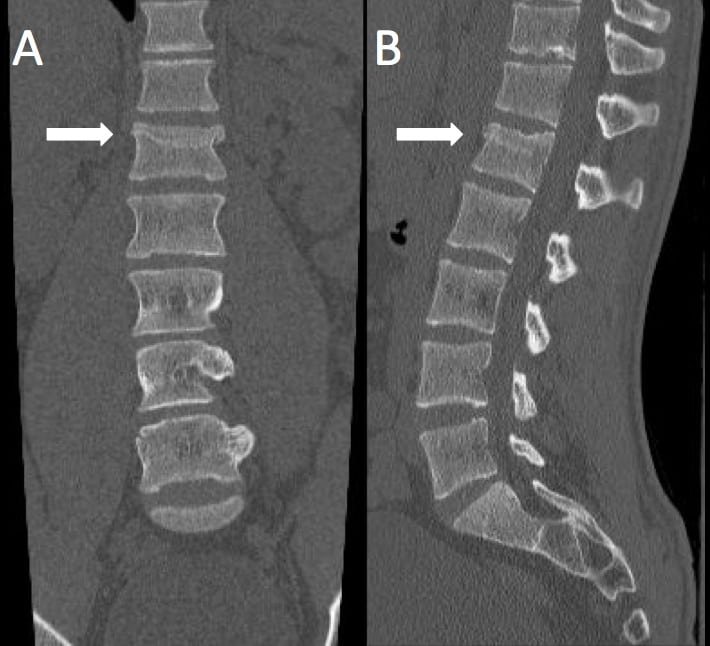
Chance fracture labeled A (antero-posterior view) and B (lateral view)involving body of the first lumbar vertebrae extending into the pedicle with probable pars interarticularis involvement without cord compression.
DISCUSSION
Mechanical low back pain is one of the most common patient complaints expressed to emergency physicians in the United States accounting for more than 6 million cases annually, with fractures a less common cause of low back pain. Chance fractures, first described in 1948 by Chance,4 are fractures caused by simultaneous flexion and distraction forces on the spinal column. The injury, most commonly to the T12-L2 spinal vertebrae, is a transverse fracture of the posterior spinous process, pedicles, and vertebral body. Due to their radiographic appearance, these are sometimes misdiagnosed as compression fractures. Most commonly seen in motor vehicle collisions with the advent of the lap seatbelt due to sudden stopping forces acting on the spine, they have decreased in incidence with the development of shoulder seatbelts.5,6
In this case, the mechanism of injury is uncharacteristic of prior descriptions of Chance fractures. This individual was wearing a sturdy mountaineering style backpack with spinal support that should allow for minimal flexion and extension of the spine while falling onto his side causing lateral flexion (Figure 2). Thus, the patient falling onto his side with the supportive backpack in place would most likely cause a lateral compression fracture and less likely a flexion-extension injury making this a unique mechanism of injury for a Chance fracture.
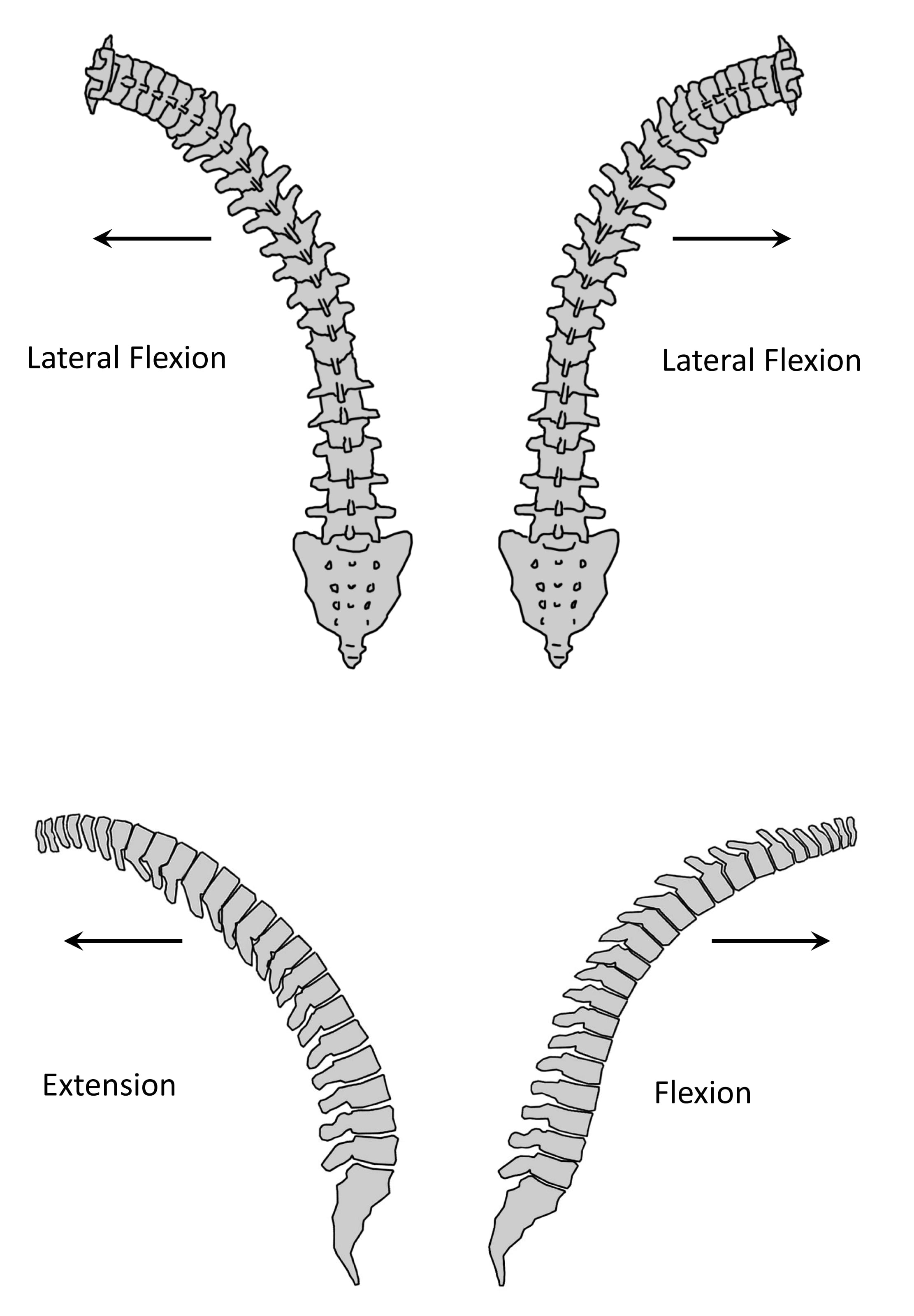
Different depictions of flexion and extension of the spine.
As emergency physicians we are trained to have a high index of suspicion when the mechanism suggests potential life-, limb-, or eye-threatening etiologies. Although this type of injury was initially described as a flexion-extension injury, when moderate to severe shearing forces are placed on the spine, as this case illustrates, the emergency physician must consider a Chance fracture in the differential diagnosis even when the mechanism is less significant.
Footnotes
Supervising Section Editor: Rick A. McPheeters, DO
Submission history: Submitted May 14, 2012; Revision received August 2, 2012; Accepted September 6, 2012
Full text available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2012.9.12646
Address for Correspondence: Aaron Birch, Madigan Army Center, Bldg 9040 Fitzsimmons Drive, Tacoma, WA 98431. Email: asbirch@gmail.com
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
The views expressed are those of the author(s) and do not reflect the official policy of the Department of the Army, the Department of Defense or the U.S. Government.
REFERENCES
1. Knapp JF, Harakas AP, Edwards RK, et al. Unusual mechanism of Chance fracture in an adolescent.Pediatr Emerg Care. 1987;3(4):256–257. [PubMed]
2. Todkar M. Unusual mechanism of Chance fracture in an adult. Acta Orthop Belg. 2005;71(5):628–629. [PubMed]
3. Hakozaki M, Otani K, Kikuchi S, et al. Chance fracture of the lumbar spine in an amateur snowboarder: a case report. J Sports Med Phys Fitness. 2010;50(2):214–216. [PubMed]
4. Chance GQ. Note on a type of flexion fracture of the spine. Br J Radiol. 1948;21(249):452–453.[PubMed]
5. Wheeless CR. Chance Fracture of the Spine. Wheeless’ Textbook of Orthopaedics. Available at:http://www.wheelessonline.com/ortho/chance_fracture_of_the_spine. Accessed May 7, 2012.
6. Geiderman JM, Katz D. General Principles of Orthopedic Injuries. In: Marx JA, Hockberger RS, Walls RM, editors. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 7th ed. Philadelphia PA: Mosby Elsevier; 2010. p. 468.