
{kind=link}
| Author | Affiliation |
|---|---|
| Eric B. Tomich, DO | Madigan Army Medical Center, Department of Emergency Medicine, Tacoma, WA |
| David Della-Giustina, MD | Madigan Army Medical Center, Department of Emergency Medicine, Tacoma, WA |
ABSTRACT
We present the case of a 45-year-old female who presented multiple times to the emergency department with acute low back pain and was subsequently diagnosed with bilateral psoas muscle abscess. Psoas abscess is an uncommon cause of acute low back pain that is associated with high morbidity and mortality. The onset of symptoms is frequently insidious and the clinical presentation vague. Proper diagnosis requires vigilance of the physician to recognize signs in the history and physical examination that are suggestive of a potentially serious spinal condition and initiate further workup. While most patients with acute low back pain have a benign etiology, this case report demonstrates the challenge of diagnosing a patient with bilateral psoas abscess who had few known risk factors and symptoms typical of mechanical low back pain.
CASE REPORT
A 45-year-old white female initially presented to the emergency department (ED) with a chief complaint of a traumatic severe left lower back pain for three days. The pain was sharp and radiated down her left anterior thigh. The pain worsened with movement and improved with rest, but persisted when lying still. Associated symptoms included dysuria and mild generalized abdominal pain. Past medical and surgical history was significant for genital herpes, iron deficient anemia, and hemorrhoidectomy. She took no prescription medicine. Social history was positive for tobacco use, but she denied alcohol or recreational drug use. Her job was labor intensive and involved heavy lifting. She first noticed the pain with associated stiffness upon waking the morning after a work shift. She denied trauma, fevers, rigors, weight loss, nausea, vomiting, diarrhea, constipation, vaginal bleeding or discharge, weakness or numbness in the lower extremities, and urinary incontinence. On physical examination she was afebrile with normal vital signs. She was in obvious discomfort and unable to sit up straight due to pain. Her gait was antalgic. She had tenderness to palpation and increased tone over her left lumbar paraspinal musculature. Her strength, reflexes and sensation of the lower extremities were normal. The remainder of the physical exam was unremarkable. She was diagnosed with lumbosacral strain and discharged home with a prescription of opiate analgesics.
The patient returned to the ED via ambulance four days later, tearful and writhing in pain. Her vital signs were normal. The physical examination was essentially unchanged from her previous encounter. Specifically, there was no midline spinal tenderness or neurologic deficits in the lower extremities. Straight leg testing was negative with reproduction of the back pain but without radiation. Plain spinal radiographs showed degenerative changes but no acute process. She was treated with intravenous (IV) opiates and antiemetics and was discharged to home when she stated her pain had diminished.
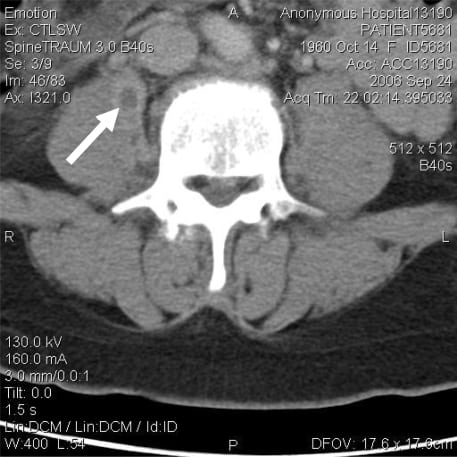
Four days later, or eight days after her initial presentation, she returned to the ED with worsening back pain and intermittent fevers up to 103°F. The pain was now located across the whole lower back with associated radiation down both anterior thighs. Heart rate and blood pressure were normal. On examination she had tenderness to palpation of the lumbar region with exacerbation of the pain upon flexion and extension of the trunk. Laboratory exam revealed a hemoglobin of 10.3 g/dl; white blood cell count of 8300 cells/mm3; and a negative urinalysis. IV opiates and benzodiazepines provided little relief. A non-contrast CT scan of the lumbar spine showed several small areas of low attenuation with peripheral enhancement in the medial margins of both psoas muscles (Figure 1). The largest of these collections measured 1.4 cm x 1.2 cm on the right and was consistent with psoas abscess collection. There was also abnormal enhancement of the paravertebral soft tissue near L3–L5, which was suspicious for diskitis. She was admitted to the hospital and started on IV ceftriaxone, metronidazole, and clindamycin for broad spectrum coverage, including anaerobes. A triple-contrast CT of the abdomen and pelvis to rule out an abdominal source of infection resulting in secondary extension to the psoas muscle was negative. MRI of the lumbar spine showed no signs of diskitis or vertebral osteomyelitis. On the second hospital day she underwent CT-guided drainage of the largest abscess in the right psoas muscle. This procedure resulted in approximately 1 mL of purulent fluid that revealed many white and red blood cells, and gram positive cocci. The fluid culture was positive for methicillin-sensitive Staphylococcus aureus (MSSA). The antibiotic regimen was changed to oral cephalexin. Two days following abscess drainage she was discharged home in stable condition. In follow up with her primary physician two weeks later she tested negative for HIV and a urine toxicology screen was positive for cocaine.
DISCUSSION
Anatomy
The psoas muscle originates from the lateral borders of the 12th thoracic to the 5th lumbar vertebrae in the retroperitoneal space and inserts at the lesser trochanter of the femur. In 70% of people it is a single structure known as the psoas muscle, but 30% have the psoas minor that lies anterior to the major.1 The fibers of the psoas muscle blend with those of the iliacus to form the iliopsoas, which functions as the chief flexor of the hip. Innervation arises from the lumbar plexus via branches of the L2–L4 nerves. The psoas is surrounded by a rich venous plexus, which could explain its predisposition to infection from hematogenous spread.2
Etiology and Epidemiology
Back pain is second only to upper respiratory infections as a cause for symptom-related visits to primary care physicians.3 Acute low back pain is defined as pain present for six weeks or less.4 Psoas abscess can be classified as either primary or secondary. The etiology of primary psoas abscess remains uncertain. Current literature suggests that it results from either hematogenous spread from occult infection or local trauma with resultant intramuscular hematoma formation, which predisposes to abscess formation.5,6 Primary psoas abscess occurs most commonly in patients with a history of diabetes, injection drug use, alcoholism, AIDS, renal failure, hematologic malignancy, immunosuppression, or malnutrition. Additional risk factors include age under 20 years, males (3:1 predominance), and low socioeconomic status.5–8 In the United States, primary psoas abscess makes up 61% of cases. The predominant organism is Staphylococcus aureus (over 88%), followed byEscherichia coli and Streptococcus.1,5,8,9 Secondary psoas abscess is often caused by a mixed flora of enteric bacteria, commonly E. coli and Bacteroides.9 Mycobacterium tuberculosis infection of the spine, known as Pott’s disease, is the most frequent cause of secondary psoas abscess in developing countries.8 Conditions associated with secondary psoas abscess include Crohn’s disease, diverticulitis, appendicitis, colorectal cancer, urinary tract infection, vertebral osteomyelitis, mycotic abdominal aortic aneurysm, endocarditis, and history of instrumentation in or around the spine.1,5 It is noteworthy that bilateral psoas abscess occurs in just 3% of all cases, primary or secondary.10
History and Physical
Symptoms are often nonspecific, which makes it difficult to make the diagnosis at the initial visit. The classic triad of fever, back pain, and psoas spasm is present in only 30% of patients.11 Other common symptoms include malaise, weight loss, nausea, anorexia, and pain that radiates to the flank, groin, or anterior thigh. 5,6,8 Back pain is the most frequently encountered symptom, with a mean duration of 10.6 days before presentation.11 On examination, the presence of a limp, palpable mass in the inguinal region, severe pain upon passive hyperextension of the hip or active flexion of the psoas against the examiner’s hand can be specific for psoas abscess. 5 Correct and early diagnosis is difficult, with arthritis, vertebral osteomyelitis, lumbar strain, and abdominal/urologic disorders being the most common alternative diagnoses.11,12 Patients that present with symptoms of septic shock or those with a Mycobacterium tuberculosis etiology are even less likely to have classic signs and symptoms which may delay definitive diagnosis and treatment.13,14
Laboratory and Radiological Testing
In general, laboratory testing is nonspecific in diagnosing psoas abscess; however, abnormal results may prompt one to pursue infection as a source of the patient’s symptoms. If there is any concern of infection, whether it be diskitis or psoas abscess, then a complete blood count (CBC), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), blood cultures, and urinalysis (UA) may be helpful.1,6,8 In a retrospective review of 11 cases, leukocytosis was the most common laboratory finding.15 Blood cultures are positive in about 50% of patients.8 ESR and CRP will generally be elevated and may be useful in following the disease course. Pyuria and anemia are also common.6Plain radiographs are typically unremarkable unless there is underlying diskitis or vertebral osteomyelitis that has been present for several weeks. Because ultrasound is diagnostic in only 60% of cases and MRI appears to have no better than the 90% sensitivity and 80% specificity of CT for diagnosing psoas abscess,1 IV contrast-enhanced spiral CT has become the gold standard in imaging.8 However, MRI is better than CT at imaging the spinal canal and provides a more complete evaluation for all potential sources of back pain. CT of the abdomen and pelvis with oral and IV contrast should also be considered, especially in cases where secondary psoas abscess is suspected. Ultimately, definitive diagnosis and treatment is achieved with CT-guided drainage and culture of fluid.6
Management and Outcomes
The initial treatment of primary psoas abscess involves the empiric use of IV anti-staphylococcal antibiotics since nearly 90% are due to S. aureus. These should have coverage against most gram positive organisms, including MRSA, with vancomycin, linezolid or clindamycin being appropriate choices. In secondary psoas abscess a mixed flora of enteric pathogens predominate. Antibiotics need to have coverage for both gram negative and anaerobic bacteria. Fluroquinolones, anti-psuedomonal penicillins, late generation cephalosporins, plus or minus metronidazole should be used empirically for maximal coverage.11,16 The antibiotic regimen can later be changed to reflect the results of the culture and sensitivity profile and in general is continued for two weeks after abscess drainage.2 CT-guided percutaneous drainage (PCD) or surgical drainage are the two definitive treatment modalities. PCD is less invasive and is currently the treatment of choice, especially in primary psoas abscess.17 Surgical drainage is indicated when PCD fails, or if there is a contraindication to PCD or abdominal pathology that requires intervention. Surgical drainage has been associated with shorter hospital stays when compared to PCD in secondary abscess due to the higher incidence of concurrent intra-abdominal pathology.18 Mortality rates for primary and secondary psoas abscess are 2.4% and 18.9% respectively.16 Death is usually due to inadequate or delayed treatment, with mortality close to 100% in patients who did not undergo drainage, most often from sepsis.6,16
CONCLUSION
Psoas abscess is an unusual cause of back pain that is often missed initially, as illustrated by this case. Perhaps if our patient had admitted to illicit drug use, as was discovered at a subsequent outpatient visit, the diagnosis could have been made sooner. It is still unknown whether she was using injection drugs, but with her ultimate diagnosis of primary psoas abscess secondary to MSSA coupled with a negative HIV test and no history of diabetes or immunosuppressed state, it seems plausible. Our patient’s management was consistent with the literature as to antibiotic choices and abscess drainage, resulting in a favorable outcome. It is important for emergency physicians to be aware of signs and symptoms suggestive of a serious spinal condition and initiate further workup. One should consider psoas abscess as a cause of back pain in the patient who presents with known risk factors: fever, unremitting pain, pain on hyperextension of the hip, and evidence of psoas spasm. Laboratory testing is helpful but not sufficient to confirm or rule out the diagnosis; therefore spinal imaging with CT or MRI is the test of choice to make the diagnosis. All patients with psoas abscess require hospitalization for surgical or percutaneous drainage and treatment with antibiotics.
Footnotes
The opinions or assertions contained herein are the private views of the authors and not to be construed as official or reflecting the views of the Department of the Army, the Department of Defense or the U.S. Government.
Supervising Section Editor: Chris Mills, MD
Submission history: Submitted June 13, 2008; Revision Received August 4, 2008; Accepted November 10, 2008
Reprints available
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Eric B. Tomich, DO, Madigan Army Medical Center, Department of Emergency Medicine, Bldg 9040 Fitzsimmons Ave, Tacoma, WA 98431
Email: eric.tomich@us.army.mil
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.