
{kind=link}
| Author | Affiliation |
|---|---|
| Costandinos Tsagaratos, DO | University of Medicine and Dentistry at New Jersey, School of Osteopathic Medicine, Department of Emergency Medicine, Stratford, New Jersey |
| Farook W Taha, MS, IV | University of Medicine and Dentistry at New Jersey, School of Osteopathic Medicine, Department of Emergency Medicine, Stratford, New Jersey |
ABSTRACT
A 52-year-old Caucasian male presented to the emergency department complaining of nontraumatic painful swelling and redness of the distal left fourth finger for 2 days, associated with malaise and subjective fever. The patient denied medical history, drugs, tobacco, or alcohol use.
On physical exam, temperature was 100.8°F. Heart rate was 118 with normal blood pressure and respirations. The patient had significant tenderness to pulp of finger with good capillary refill and without fluctuance (Figure 1). Cardiac exam revealed 3/6 pansystolic murmur heard loudest at the left sternal border with transmission to the apex and into the cardiac base. The patient specifically denied history of heart murmur. Upon further questioning, the patient admitted to dental work done 3 weeks prior to presentation resulting in a tooth abscess requiring oral antibiotics.

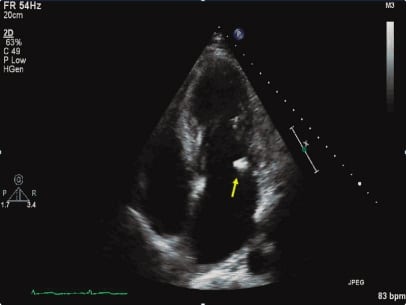
The patient had a white blood count of 16. A transthoracic echocardiogram was performed showing a 9-mm vegetation on the mitral valve consistent with infective endocarditis (IE) (Figure 2). The patient had 1 set of blood cultures drawn and was treated with appropriate intravenous antibiotics. Several sets were drawn on subsequent days, all of which showed no growth, likely secondary to partial treatment from oral antibiotics. Patient was treated empirically for a total of 6 weeks. He underwent surgical repair of leaflet due to concern of septic embolism after only 2 weeks of treatment. Patient fully recovered.
Infective endocarditis affects 10,000 to 20,000 people annually in the United States.1 Patients can present with fever, fatigue, malaise, night sweats, and weight loss. On exam, a new murmur or change in existing one are clues to making a preliminary diagnosis in the emergency department.1,2 Janeway lesions or Osler nodes can support clinical suspicion of IE.1,3 In a prospective cohort study, the International Collaboration on Endocarditis reported 3% of 2,648 adult patients with IE had Osler node.2 Infective endocarditis is diagnosed according to the Duke Criteria and the mainstay of treatment is Ivantibiotics.3
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted May 24, 2011; Revision received June 14, 2011; Accepted June 22, 2011
Reprints available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2011.6.6806
Address for Correspondence: Costandinos Tsagaratos, DO
University of Medicine and Dentistry at New Jersey, School of Osteopathic Medicine, Department of Emergency Medicine, 18 E Laurel Rd, Stratford, NJ 08084
E-mail: tsagarco@umdnj.edu
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding, sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Mylonakis E, Calderwood SB. Infective endocarditis in adults. N Engl J Med. 2001;345:1318–1330.[PubMed]
2. Murdoch DR, Corey GR, Hoen B, et al. International Collaboration on Endocarditis-Prospective Cohort Study (ICE-PCS) Investigators. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-Prospective Cohort Study. Arch Intern Med. 2009;169:463–473. Full-text, commentary can be found in Arch Intern Med. 2009;169:1720. [PubMed]
3. Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis: diagnosis, antimicrobial therapy, and management of complications: a statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association: endorsed by the Infectious Diseases Society of America. Circulation.2005;111:e394–e434. [PubMed]