
{kind=link}
| Author | Affiliation |
|---|---|
| Jack S. Wu, MD | University of Illinois College of Medicine, Chicago, IL |
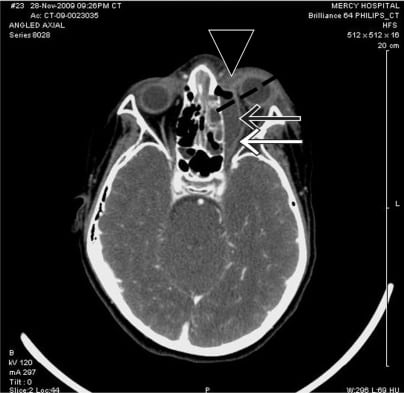
A seven-year-old male presented with fever, left-sided facial redness, swelling and proptosis over a 24-hour period. He had noted left-sided toothache and rhinorrhea over the preceding week. On presentation, he stated that he was unable to see “anything, including light” from his left eye. On physical examination, the patient was febrile with left periorbital swelling and significant left-sided proptosis, chemosis and loss of extra-ocular movements. As a part of the evaluation we obtained, a contrast-enhanced computed tomography (CT) scan, which demonstrated extraconal orbital subperiosteal abscess with air-fluid collection along the medial and anterior walls of the maxillary sinus with associated lateral displacement of the left medial and inferior recti, left preseptal cellulitis with proptosis, left maxillary and ethmoid sinusitis. We began intravenous Unasyn, and the patient underwent intraoperative drainage of the left orbital abscess, maxillary antrostomy, and total ethmoidectomy.
Orbital infections are posterior to the orbital septum and involve the orbit itself as compared to periorbital infections.1 Given the make-up of its anatomical boundaries, the etiology of orbital cellulitis and abscess is often due to extensions of sinus infections.1 Case reports from odontogenic sources have also been reported.2 Physical exam differentiations between orbital infections from periorbital infections include proptosis, chemosis, and ophthalmoplegia.1 CT scanning may assist in diagnostic differentiation, as well as in determining which patients will benefit from surgical intervention.3,4 Common contrast-enhanced CT scan findings of orbital abscess include ring-enhanced lesion or an air-fluid level in the extraconal space, displacement of adjacent rectus muscle, marked proptosis, and in advanced cases osteomyelitis of the orbital wall.4 Causative organisms of orbital cellulitis and abscess include S. pneumonia, nontypable Haemophilus influenzae, Moraxella catarrhalis, group A Streptococcuus, Staphylococcus aureus, and anaerobes. Treatment involves intravenous antimicrobial therapy and in some cases surgical drainage.1,5,6


Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted April 4, 2010; Revision Received April 26, 2010; Accepted May 6, 2010.
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Jack S. Wu, MD, Department of Emergency Medicine, Mercy Hospital Medical Center, 2525 S. Michigan Avenue, Chicago, IL 60616
Email: jack.wu.md@gmail.com
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Givner LB. Periorbital versus orbital cellulitis. Pediatr Infect Dis J. 2002;21(12):1157–8. [PubMed]
2. Stübinger S, Leiggener C, Sader R, et al. Intraorbital abscess: a rare complication after maxillary molar extraction. J Am Dent Assoc. 2005;136(7):921–5. [PubMed]
3. Rudloe TF, Harper MB, Prabhu SP, et al. Acute Periorbital Infections: Who Needs Emergent Imaging. Pediatrics. 2010 Mar 1;
4. Eustis HS, Mafee MF, Walton C, et al. MR imaging and CT of orbital infections and complications in acute rhinosinusitis. Radiol Clin North Am. 1998;36(6):1165–1183. xi. [PubMed]
5. Starkey CR, Steele RW. Medical management of orbital cellulitis. Pediatr Infect Dis J.2001;20:1002–5. [PubMed]
6. Fakhri S, Pereira K. Endoscopic management of orbital abscesses. Otolaryngol Clin North Am.2006;39(5):1037–47. [PubMed]