
{kind=link}
| Author | Affiliation |
|---|---|
| Ernesto Muñoz-Mahamud, MD | Hospital Clinic of Barcelona, Department of Orthopaedic Surgery and Traumatology, University of Barcelona, Barcelona, Spain |
| Andrés Combalia, MD, PhD | Hospital Clinic of Barcelona, Department of Orthopaedic Surgery and Traumatology, University of Barcelona, Barcelona, Spain |
INTRODUCTION
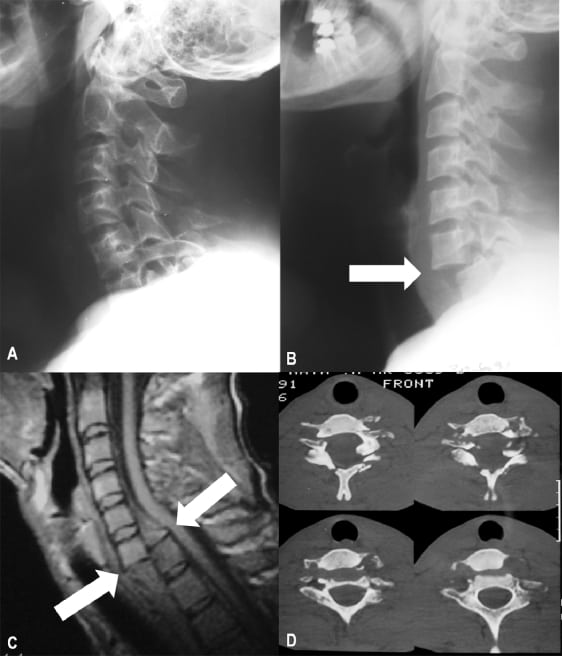
A 30-year-old man presented to the emergency department after a motorcycle accident at high speed. He reported neck pain and referred paresthesia along the fourth and fifth fingers of both the left and the right hand. The patient arrived at hospital hemodynamically stable. His Glasgow Coma Scale was 15 and the physical examination revealed numbness of the ulnar side of the left and the right hand as well as pain located at the lower cervical spine. Initial radiograph image of the cervical spine did not show any spine injury (Figure, part A). Since this initial radiograph had not included the vertebral spine below C6, the image was then repeated to include the whole cervical spine (Figure, part B; see arrow). A dislocation C6 to C7 injury was then disclosed. Computerized tomography and magnetic resonance imaging were performed as well so as to complete the study, depicting a comminuted fracture dislocation C6 to C7 injury by a mechanism of extension-compression1 (Figure, parts C and D). The patient was taken early to the operating room so as to be operated through a double approach in lateral decubitus under halo traction.
An accurate detailed history and physical examination are essential if a diagnosis of cervical spinal injury is not to be missed. The reported frequency of missed injuries ranges from 4% to 30%, and the most common cited reason for this is inadequate radiologic examination.2,3 Lateral cervical spine radiograph images must visualize the entire cervical spine. When lower vertebras are not included, repeated radiograph images showing the entire cervical spine are mandatory. When an injury is missed initially, the delay in diagnosis puts the patient at risk for progressive instability and neurologic deterioration.4 Prompt reduction and internal stabilization has been advocated to achieve full recovery.
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted March 27, 2011; Accepted March 28, 2011
Reprints available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2011.3.2266
Address for Correspondence: Ernesto Mun˜ oz-Mahamud, MD
Hospital Clinic of Barcelona, Department of Orthopaedic Surgery and Traumatology, University of Barcelona, C/Villarroel 170, Barcelona, 08036, Spain
E-mail: e.munoz.mahamud@gmail.com
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Allen BL, Ferguson RL, Lehmann TR, et al. A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine. 1982;;7:1–27. [PubMed]
2. Bohlman HH. Acute fractures and dislocations of the cervical spine: an analysis of three hundred hospitalized patients and review of the literature. J Bone Joint Surg Am. 1979;;61:1119–1142.[PubMed]
3. Gerrelts BD, Petersen EU, Mabry J, et al. Delayed diagnosis of cervical spine injuries. J Trauma.1991;;31:1622–1626. [PubMed]
4. Reid DC, Henderson R, Saboe L, et al. Etiology and clinical course of missed spine fractures. J Trauma. 1987;;27:980–986. [PubMed]