
{kind=link}
| Author | Affiliation |
|---|---|
| Leslie S. Zun, MD, MBA | Rosalind Franklin University of Medicine and Science/Chicago Medical School, Department of Emergency Medicine Mount Sinai Hospital, Department of Emergency Medicine, Chicago, Illinois |
ABSTRACT
Introduction:
The purpose of this paper was to review and analyze all the literature concerning ED patient throughput. The secondary goal was to determine if certain factors would significantly alter patients’ ED throughput.
Methods:
A MEDLINE search was performed from 1966 to 2007 using the terms “turnaround,” “emergency departments,” “emergency medicine,” “efficiency,” “throughput,” “overcrowding” and “crowding.” Studies were graded using a scale of one to four based on the ACEP paper quality criteria. Inclusion criteria were English language and at least a level four or better on the quality scale. An analysis of successful procedures and techniques was performed.
Results:
Literature search using the key terms found 29 articles on turnaround times, 129 on ED efficiency, 3 on throughput, 64 on overcrowding and 52 on crowding. Twenty-six articles were found to meet the inclusion criteria. There were three level I studies, thirteen level II studies, five level III studies and five level IV studies. The studies were categorized into five areas: determinants (7), laboratories processes (4), triage process (3), academic responsibilities (2), and techniques (10). Few papers used the same techniques or process to examine or reduce patient throughput precluding a meta-analysis.
Conclusion:
An analysis of the literature was difficult because of varying study methodologies and less than ideal quality. EDs with combinations of low inpatient census, in-room registration, point of care testing and an urgent care area demonstrated increased patient throughput.
INTRODUCTION
Improving efficiency and throughput in the emergency department (ED) has multiple benefits. Better efficiency should increase patient satisfaction, enhance revenue and reduce ambulance diversion. The need to focus on ED efficiency has become more acute in recent years due to increasing litigation, including a case where a patient in Chicago died while waiting for care.1
EDs across the U.S. struggle to provide efficient care in a timely fashion. Increasing patient volumes, a reduction in the number of EDs, higher inpatient census and ED staff reduction all exacerbate the struggle. The purpose of this paper is to review the literature and summarize strategies used nationwide to deal with this crisis. Proven techniques could be used by hospital and ED managers.
METHODS
We searched MEDLINE from 1966 to March 2007 for English language articles using the keywords turnaround, efficiency, throughput, overcrowding and crowding. No other restrictions in the search fields were used. We also reviewed references from these articles to ensure that we included all possible studies.
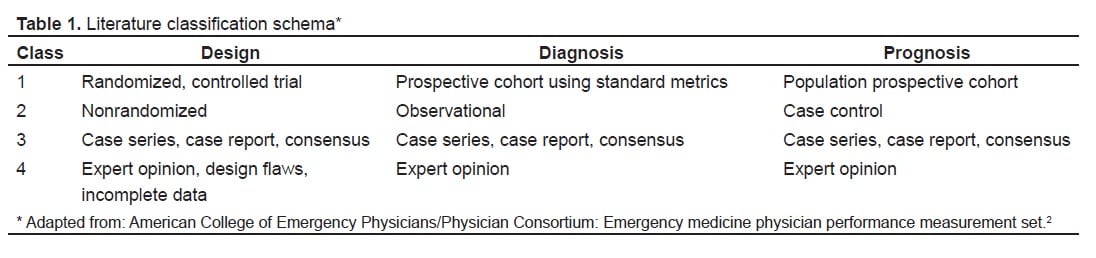
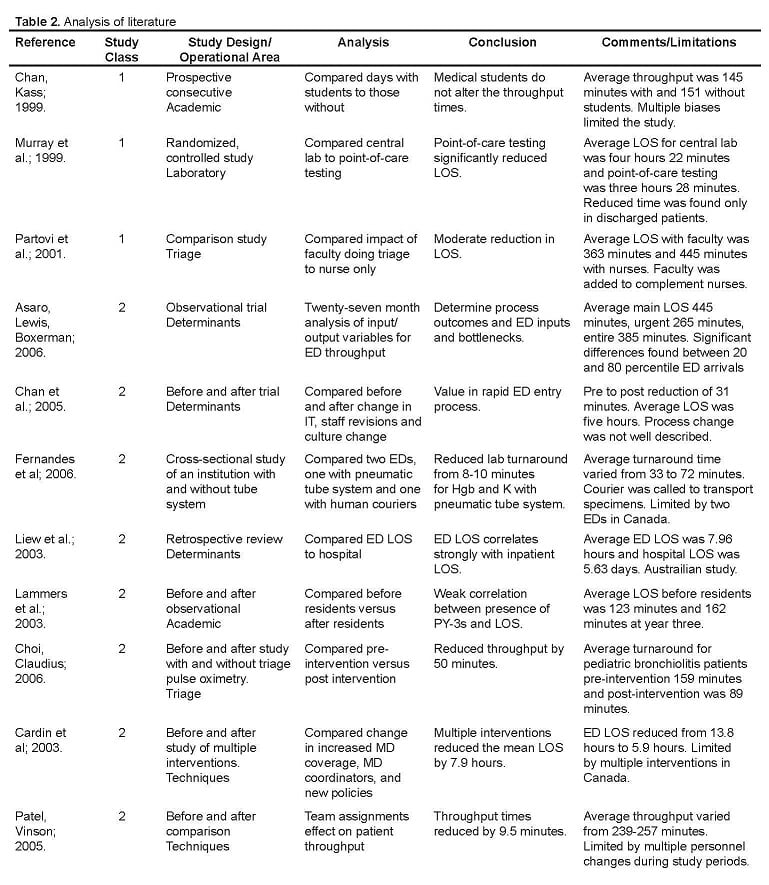
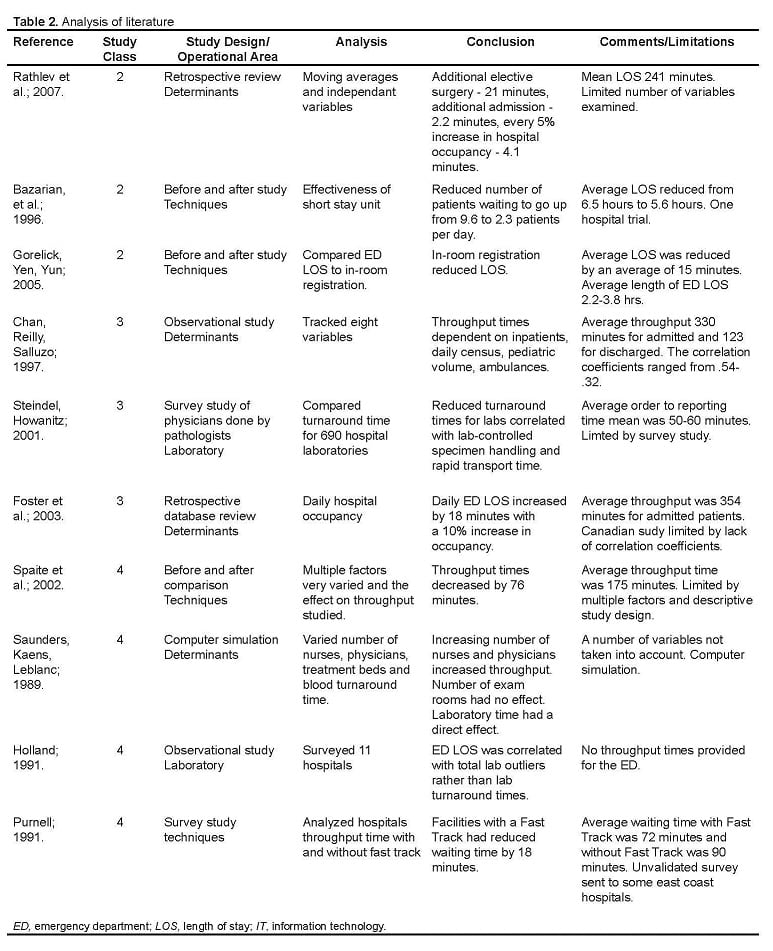
We required one or more factors related to throughput to include an article in further analysis. We used a classification system modified from the American College of Emergency Physicians to assess the study’s methodology and quality.2 To be more inclusive in the review, a fourth parameter was added to the classification system (Table 1). Each article was graded one to four based on this classification scheme. Those studies with confounding variables, problematic study design, limited data or poor presentations were downgraded to the next lower class. Due to the lack of uniformity and consistency within the literature, studies of similar design and technique could only be identified and grouped into five broad categories: throughput determinates, academic responsibilities, laboratories, triage, and techniques. A table of the findings was produced to summarize the class, design, analysis, conclusion and limitations of each study (Table 2).
RESULTS
The literature search using the keywords crossed with “emergency departments” and “emergency medicine” (EM) found 29 articles related to turnaround, 129 articles related to efficiency, four articles related to throughput, 52 articles related to crowding and 64 articles related to overcrowding.
Twenty-six articles were found to meet the inclusion criteria. Studies that lacked data, had poor scientific design or provided limited information were not rated. There were three level I studies, 13 level II studies, five level III studies and five level IV studies (Table 2). We then sorted them, using the five broad categories throughput determinants (seven articles), laboratories processes (four articles), academic responsibilities (two articles), triage process (three articles), and throughput reduction techniques (10 articles).
Throughput Determinants
Several articles focused on the correlation between throughput time and ED factors. The articles showed that ED length of stay (LOS) increased substantially with increased admissions, number of ambulance arrivals, number of pediatric patients and ED census.3–8 Rathlev et al.8 found that daily mean LOS was increased not only by number of ED admission and hospital occupancy but also by elective surgical admission. Interestingly, two of the studies did not find a significant correlation between the throughput time and hours of nursing coverage, day of the week or urgent care hours.3,4Saunders et al.9 performed a computer simulation study of ED operations and found that throughput times correlated directly with laboratory service times and inversely with number of physicians and nurses. This latter relationship had a ceiling where a continued increase in providers demonstrated no change in throughput time.9
Academic
Two studies examined the effect of teaching on ED throughput. Chan et al.10 examined how medical students affected ED throughput and found that fourth year medical students’ precepting for four weeks in the ED did not change the LOS for patients. A similar study11 looking at the effects of adding EM residents found that the residents increased the total throughput time an average of seven to 39 minutes.
Laboratories
In a study of 11 hospital EDs, Holland et al.12 found that addressing the laboratory outliers rather than the mean turnaround time can reduce the ED LOS. In a study of 690 hospital laboratories, Steindel and Howanitz13 found that faster throughputs were related to lab control of the specimen handling and rapid transport times. Murray et al.14 performed a randomized controlled trial comparing point-of-care testing to central laboratory testing and found that point-of-care testing reduced the median stay by 54 minutes. Study supplies and equipment but not grant funding were provided for this potentially biased study. In a comparison study of the use of a pneumatic tube delivery system versus human couriers, Fernandes et al.15 found that a tube system reduced lab reporting time by 8–10 minutes.
Triage
Partovi et al.16 compared the LOS in triage with and without an emergency physician, and found an 18% reduction in LOS when a physician began patient evaluation and treatment in triage. This paper reported a significant cost of physicians in triage, which may outweigh the benefits of reduced LOS. Choi and Claudius17 studied the use of pulse oximetry on bronchiolitis patients in triage and found that it could reduce throughput by 50 minutes. The authors did not study the reason for decreased throughput time nor describe how the evaluation and treatment may have been altered with pulse oximetry measurement; however, they suggested that identification of hypoxia changes management, and proper patient placement to urgent care or main ED may have accounted for this time reduction.
Techniques
Multiple studies described techniques used to reduce ED LOS. Spaite et al.18 examined one ED that employed a rapid process redesign, and found that it led to a 76-minute reduction in average patient LOS. The rapid redesign focused on staffing and internal processes, triage and registration procedures and diagnostic radiology, laboratory and bed availabilities. This rapid improvement process occurred over three months and cost the hospital over $1 million annually. This cost was offset by increased revenue, providing a net annualized profit of $300,000. Purnell et al.19 surveyed 185 hospitals and found that an urgent care unit reduced patient wait times by 20%. This limited survey study performed in 1989 found that the mean wait time was 72 minutes in EDs with fast track and 90 minutes for those without.
In a comparison of multiple interventions, Cardin et al.20 found that increased emergency physician (EP) coverage, designation of a physician coordinator and changes in hospital policies on laboratory, consultations and admission procedures could reduce ED mean LOS from 13.8 hours to 5.9 hours. The article focused on the effect of the interventions on return visits and hospital readmissions and not on the interventions used and associated costs. There were ten total interventions noted in the appendix with transfer-to-ward within one hour of bed assignment having the most impact.
Patel and Vinson21 used an ED team concept, which joined an EP with two nurses and one technician. This novel change lead to improved patient satisfaction with an increase of 3.1% in reported “very good” or “excellent” ratings, a reduction in the time required to see a physician, a 7.7% increase in number of patients seen within one hour, and a 0.7% decrease in patients who left without being seen.
Another published approach to reducing the ED LOS was to use a 72-hour admission unit on an existing medical unit with 16 beds designated for ED overflow patients.22 This study, which used a short-stay, 72-hour unit found that chest pain and asthma patients had a significant reduction in ED throughput times. Mean ED time was reduced from 7.3 to 5.5 hours per chest pain patient, and 5.0 to 2.9 hours per patient with asthma; however, patients with sickle-cell disease or seizures showed no decrease. The article notes that no other changes in protocols, staffing or processes occurred during the study period. Although this study examined the effect of a short stay unit, in essence it was evaluating the effect of increased inpatient capacity on LOS in the ED. Gorelich, Yen and Yun23 found that in-room registration reduced the length of ED stay by 15.0 minutes or 9.3%.
DISCUSSION
After a thorough review of the literature, we were unable to find consensus on techniques to improve ED efficiency and thereby decrease LOS. This is most likely due to environmental, demographic, or institutional variations. One could conjecture that there are significant differences between teaching and non-teaching, small community versus large university, trauma versus non-trauma centers, and large-volume versus small-volume hospitals that prevent agreement on specific techniques. In other studies, the conclusions were not intuitive or widely accepted. For instance, two studies found that residents slowed patient throughput but medical students did not. Unfortunately, there are no comparisons of those institutions with both medical students and residents, level of student or residents, or the effect of residents from other services.
Despite a lack of consensus, this analysis demonstrates that there are a number of scientifically-based procedures to reduce ED patient LOS that could be useful. Certain strategies appear to be universally accepted. These include pulse oximetry determination in triage, bedside registration, point-of-care testing, use of an urgent care area, and efficient lab, radiograph and hospital admission processes. Furthermore, the use of physicians in triage was found to be effective, although a cost versus benefit analysis is needed. The ability to apply and implement many of these procedures in other EDs is dependent on local factors, politics and resources.
Many other articles were reviewed that were not included in this study either because they did not meet the study requirements or were not found in MEDLINE. The study required that the article include some type of research rather than a description of process improvement techniques. Valuable information on throughput is frequently published in hospital or management journals that discuss process improvement.
Based on a review of the literature on reducing patient LOS in the ED, the best means for improvement is first to select the appropriate determinants that drive patient throughput at the local level, such as number of admissions, number of ambulance arrivals and ED census, and then review and revise the processes that drive the throughput determinants and monitor the data to ensure that the changed processes accomplish the goal to improve throughput.
In the author’s experience, the critical success factors to implement the necessary changes were to obtain accurate and timely throughput data to review, obtain buy-in to the process from senior management as well as staff who will have to implement the changes, and determine what the cost/benefit ratio will be. At the author’s hospital, LOS was reduced by 31% and the left-without-treatment rate was reduced from 10% to 2% without any additional costs in a three-month time period. The keys to success were a rapid redesign process involving all hospital departments and services, as well as senior management and line staff, using accurate and correct ED data and having managers focus on a self–initiated process improvement methodology.
LIMITATIONS
These data could not be tabulated to perform a meta-analysis because of diverse study designs and the marginal quality of the papers. In general, the research methodology in these administrative studies was not as rigorous as other scientific research. Most were observational or before-and-after studies, which included potential confounding variables. Additional factors to explain the problems with this type of research include lack of external funding, difficulty in isolating specific techniques to reduce LOS, or difficulty performing randomized interventions. The analysis of each article was scientifically based, but there was always the possibility of rater bias. Lastly, the grouping of study topics was arbitrary but necessary to determine trends and commonalities.
CONCLUSION
The world’s ED throughput literature is limited in applicability from one institution to another; however, there do appear to be some overarching alterations in behavior that will serve to speed patients through the ED. Useful strategies include improvements in triage, urgent care centers, point-of-care testing and bedside registration.
Footnotes
Supervising Section Editor: Christopher A. Kahn, MD, MPH
Submission history: Submitted March 31, 2008; Revision Received September 15, 2008; Accepted November 24, 2008
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Leslie S Zun, MD, MBA. Chairman, Department of Emergency Medicine Mt. Sinai Hospital Medical Center, 15th and California, Chicago, Illinois 60608
Email: zunl@sinai.org
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Sorrel AL. Woman’s death in hospital emergency department ruled a homicide.AMNews. 2006 Oct 16;
2. American College of Emergency Physicians/Physician Consortium Emergency Medicine Physician performance measurement set. Available at:www3.acep.org/WorkArea/showcontent.aspx?id=31584. Accessed November 07, 2007.
3. Chan L, Reilly KM, Saluzzo RF. Variables that affect patient throughput times in an academic emergency department. Am J Med Quality. 1997;12:183–186.
4. Chan TC, Killeen JP, Kelly D, Guss DA. Impact of rapid entry and accelerated care at triage on reducing emergency department patient wait times, lengths of stay, and rate of left without being seen. Ann Emerg Med. 2005;46:491–497. [PubMed]
5. Foster AJ, Steill I, Wells G, et al. The effect of hospital occupancy on emergency department length of stay and patient disposition. Acad Emerg Med. 2003;10:127–33.[PubMed]
6. Liew D, Liew D, Kennedy MP. Emergency department length of stay independently predicts excess inpatient length of stay. Med J Australia. 2003;179:524–526. [PubMed]
7. Asaro PV, Lewis LM, Boxerman SB. The impact of input and output factors on emergency department throughput. Acad Emerg Med. 2007;14:235–42. [PubMed]
8. Rathlev NK, et al. Time series analysis of variables associated with daily mean emergency department length of stay. Ann Emerg Med. 2007;49:265–271. [PubMed]
9. Saunders CE, Makens PK, Leblanc LJ. Modeling emergency department operations using computer simulation systems. Ann Emerg Med. 1989;18:134–140. [PubMed]
10. Chan L, Kass LE. Impact of medical student preceptorship on ED patient throughput time. AM J Emerg Med. 1999;17:41–43. [PubMed]
11. Lammers RL, Roiger M, Rice L, et al. The effect of a new emergency medicine residency program on patient length of stay in a community hospital emergency department. Acad Emerge Med. 2003;10:725–730.
12. Holland LL, Smith LL, Blick KE. Reducing laboratory turnaround time outliers can reduce emergency department patient length of stay. Am J Clic Pathol. 2005;124:672–674.
13. Steindel SJ, Howanitz PJ. Physician satisfaction and emergency department laboratory test turnaround time: Observations based on College of American Pathologists Q-Probes Studies. Arch Pathol Lab Med. 2001;125:863–871. [PubMed]
14. Murray RP, Leroux M, Sabga E, Palatnich W, Ludwig L. Effect of point-of-care testing on length of stay in an adult emergency department. J Emerg Med. 1999;17:811–814.[PubMed]
15. Fernandes CM, Worster A, Eva K, Hill S, McCallum C. Pneumatic tube delivery system for blood samples reduces turnaround times without affecting sample quality. J Emerg Nurs. 2006;32:139–143. [PubMed]
16. Partovi SN, Nelson BK, Bryan ED, et al. Faculty triage shortens emergency department length of stay. Acad Emerg Med. 2001;8:990–995. [PubMed]
17. Choi J, Claudius I. Decrease in emergency department length of stay as a result of triage pulse oximetry. Ped Emerg Care. 2006;22:412–414.
18. Spaite DW, Bartholomeaux F, Guisto J, Lindberg E, et al. Rapid process redesign in a university-based emergency department: Decreasing waiting time intervals and improving patient satisfaction. Ann Emerg Med. 2002;39:168–177. [PubMed]
19. Purnell LD. A survey of emergency department triage in 185 hospitals: physical facilities, fast track systems, patient-classification systems, waiting times, and qualification, training and skills of triage personnel. J Emerg Nurs. 1991;17:402–407.[PubMed]
20. Cardin S, Afilalo M, Lang E, Collet JP, et al. Intervention to decrease emergency department crowding: does it have effect on return visits and hospital readmissions? Ann Emerg Med. 2003;41:173–185. [PubMed]
21. Patel PB, Vinson DR. Team assignment system: expediting emergency department care. Ann Emerg Med. 2005;46:499–506. [PubMed]
22. Bazarian JJ, Schneider SM, Newman VJ, Chodosh J. Do admitted patients held in the emergency department impact the throughput of treat-and-release patients? Acad Emerg Med. 1996;3:1113–1118. [PubMed]
23. Gorelick MH, Yen K, Yun HJ. The effect of in-room registration on emergency department length of stay. Ann Emerg Med. 2005;45:128–133. [PubMed]