
{kind=link}
| Author | Affiliation |
|---|---|
| Tatsuki Sengoku, MD | Hitachi General Hospital, Emergency Medicine and Critical Care Medicine Department, Jonancho, Hitachi-shi, Ibaraki, Japan |
| Tomohiro Sonoo, MD | Hitachi General Hospital, Emergency Medicine and Critical Care Medicine Department, Jonancho, Hitachi-shi, Ibaraki, Japan |
| Kei Kira, MD | Hitachi General Hospital, Emergency Medicine and Critical Care Medicine Department, Jonancho, Hitachi-shi, Ibaraki, Japan |
| Yuji Takahashi, MD | Hitachi General Hospital, Emergency Medicine and Critical Care Medicine Department, Jonancho, Hitachi-shi, Ibaraki, Japan |
| Hideki Hashimoto, MD | Hitachi General Hospital, Emergency Medicine and Critical Care Medicine Department, Jonancho, Hitachi-shi, Ibaraki, Japan |
| Kensuke Nakamura, MD, PhD | Hitachi General Hospital, Emergency Medicine and Critical Care Medicine Department, Jonancho, Hitachi-shi, Ibaraki, Japan |
CASE PRESENTATION
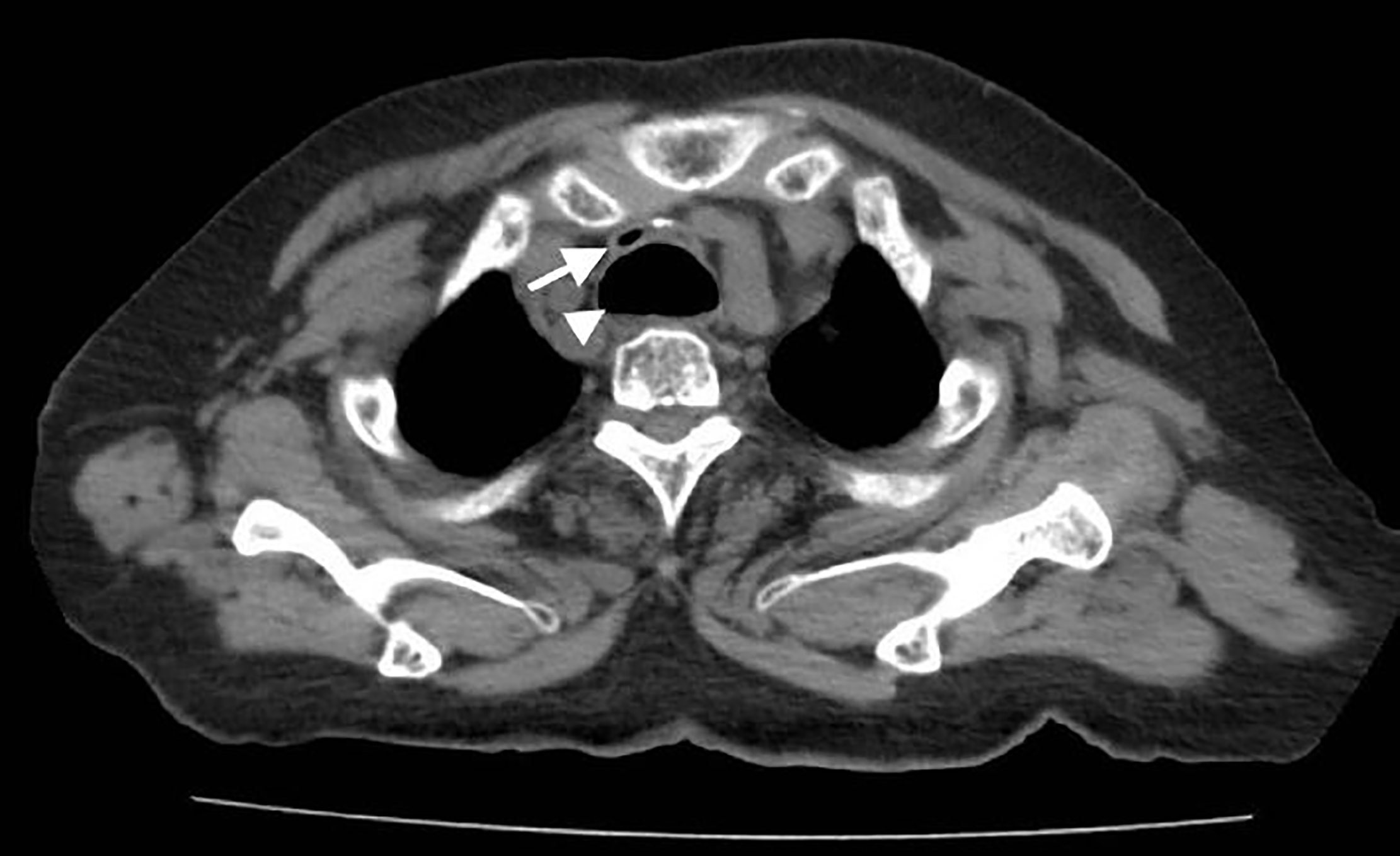
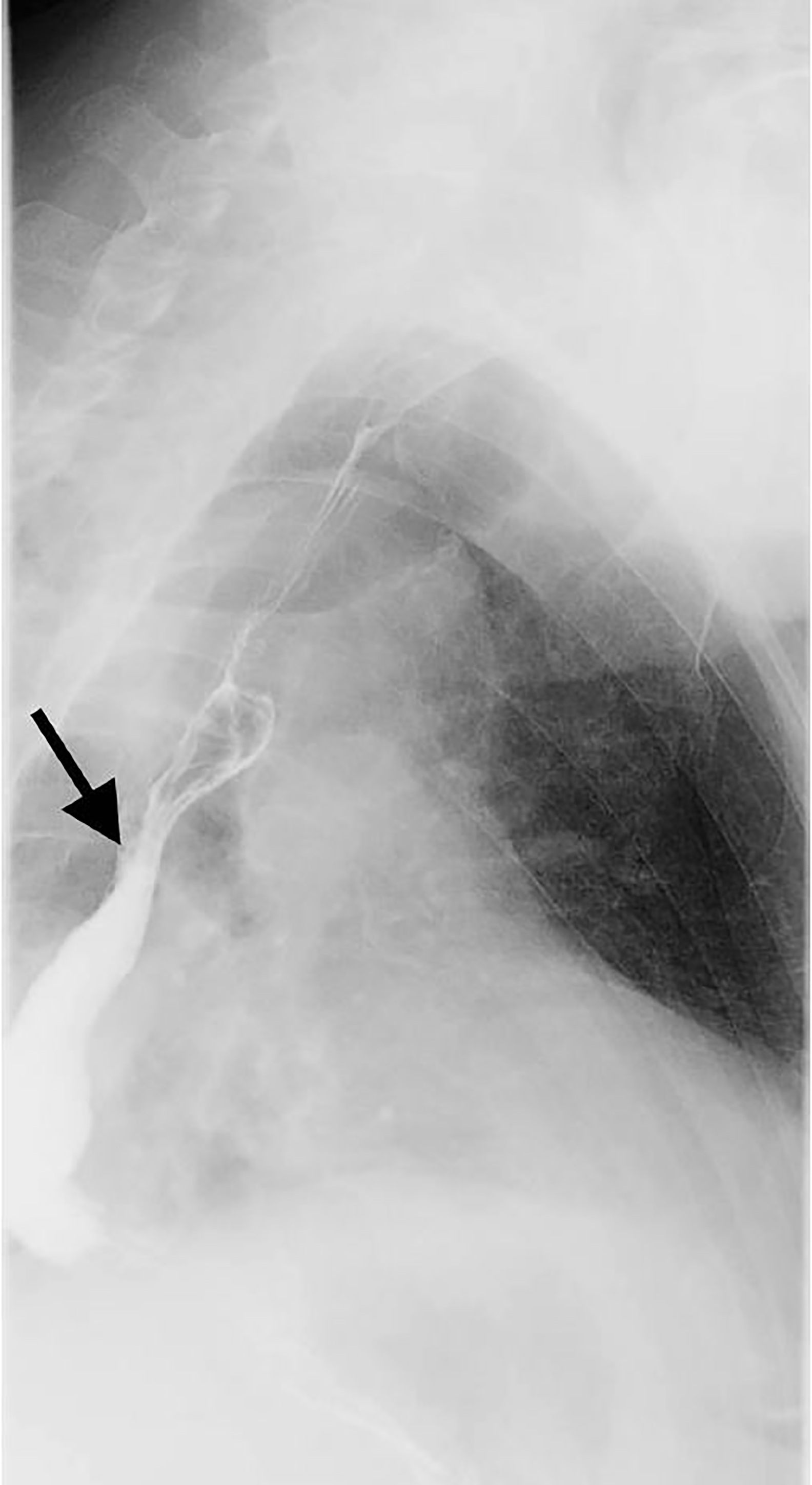
An 80-year-old woman with a medical history of diabetes and duodenal cancer presented to our emergency department (ED) complaining of sudden severe dyspnea after vomiting. She was alert and oriented on arrival, but showed tachypnea and poor oxygenation. Inspiratory stridor was evident. A computed tomography (CT) revealed a dilated esophagus with food bolus and intraluminal air compressing the trachea at the level of the sternoclavicular joint (Image 1). Her symptoms improved after 30 minutes of rest and oxygen administration; however, she was admitted for observation. Repeat CT (Image 2) and esophagography (Image 3) were performed six days later and revealed no abnormality or evidence of esophageal dysfunction. The patient’s repeat CT, esophagography, and esophagogastroscopy revealed no abnormality or evidence of hiatal herniation or esophageal achalasia.

DISCUSSION
This case presented reversible, severe tracheal compression by dilated esophagus with no functional abnormality. Cases of tracheal compression by dilated esophagus with structural diseases such as hiatal herniation1 or functional diseases such as esophageal achalasia2 have been reported. Dyspnea caused by esophageal achalasia is reportedly common in elderly women, who usually recover after treatment for esophageal achalasia.2 Unfortunately, functional evaluation of the esophagus is not performed in all cases. Some cases improve without treatment.3 Results obtained in this case suggest that a functionally normal esophagus can sometimes become sufficiently dilated to compress the upper airway, causing severe dyspnea. Spontaneous esophageal dilation is a rare cause of tracheal obstruction, but it is worth considering when no other cause is evident.
CPC-EM Capsule
What do we already know about this clinical entity?
Cases of tracheal compression by dilated esophagus with hiatal herniation or esophageal achalasia have been reported.
What is the major impact of the image(s)?
Reversible tracheal compression by dilated functionally normal esophagus was evident on the first CT.
How might this improve emergency medicine practice?
Spontaneous esophageal dilation is rare, but worth considering when we see the ED patients complaining of sudden severe dyspnea.
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Address for Correspondence: Tomohiro Sonoo MD, Hitachi General Hospital, Emergency Medicine and Critical Care Medicine Department, 2-1-1 Jonancho, Hitachi-shi, Ibaraki, Japan, 3170077. Email: tomohiro.sono.st@hitachi.com. 2:177 – 178
Submission history: Revision received January 10, 2018; Submitted March 12, 2018; Accepted March 21, 2018
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Miyake Y, Fujimoto T, Ikenaga M, et al. A Case of Large Sliding Hiatal Hernia of the Esophagus Associated with Dyspnea. J Jpn Clin Surg. 1997;58(5):1014-7.
2. Hatakeyama J, Takei T, Ito T, et al. Airway obstruction in a patient with achalasia: a case report and a review of the literature. JAAM. 2010;21(7):377-82.
3. Westbrook JL. Oesophageal achalasia causing respiratory obstruction. Anaesthesia. 1992;47(1):38-40.