
{kind=link}
| Author | Affiliation |
|---|---|
| Bethany A. West, MPH | Georgia State University’s Institute of Public Health in Atlanta, GA |
| Monica H. Swahn, PhD | Georgia State University’s Institute of Public Health in Atlanta, GA |
| Frances McCarty, PhD | Georgia State University’s Institute of Public Health in Atlanta, GA |
ABSTRACT
Introduction:
The current study examines the associations between a range of risk factors and reports of suicide attempts and attempts requiring medical care in a nationally representative study of high school students. The goal is to examine sex differences in the risk factors associated with suicide attempts and attempt-related injuries requiring treatment by a health-care provider.
Methods:
We used data from the 2007 Youth Risk Behavior Survey for students in grades 9–12 to assess the prevalence and risk factors for suicidal behavior, as well as differences in these for boys and girls. Cross-sectional multivariate logistic regression analyses were computed to determine the most important risk factors for suicide attempts and for suicide attempts requiring medical care for the sample overall and also stratified for boys and for girls.
Results:
Overall, 6.9% of adolescents attempted suicide (9.3% of girls versus 4.6% of boys). Girls were more likely than boys to report a suicide attempt in the past year (Adj.OR=2.89). Among girls, sadness (Adj.OR=5.74), weapon carrying (Adj.OR=1.48), dating violence (Adj.OR=1.60), forced sex (Adj.OR=1.72), and huffing glue (Adj.OR=2.04) were significantly associated with suicide attempts. Among boys, sadness (Adj.OR=10.96), weapon carrying (Adj.OR=1.66), forced sex (Adj.OR=2.60), huffing glue (OR=1.63), hard drug use (Adj.OR=2.18), and sports involvement (Adj.OR=1.52) were significantly associated with suicide attempts.
Conclusion:
These findings demonstrate similarities and differences in the modifiable risk factors that increase risk for suicide attempts among boys and girls. In terms of the differences between boys and girls, hard drug use and sports involvement may be important factors for suicide-prevention strategies directed specifically towards boys, while dating violence victimization may be an important risk factor to address for girls. Overall, these findings can help guide prevention, clinical practice, and intervention strategies to prevent suicidal behaviors among adolescents.
INTRODUCTION
Youth suicide is an increasingly important public health issue in the U.S. that impacts many adolescents, their families and communities.1–9 In 2006 suicide was the third leading cause of death among youth 10–24 years of age.2 Research shows that 8.4% (10.8% for girls and 6.0% for boys) of high school students in the U.S. reported attempting suicide in the past year.10 Several well known risk factors exist for suicidal behavior among youth.1,3–9 These include depression, impulsive and aggressive behaviors, previous victimization, social isolation, alcohol and drug use, sexual activity, and family factors. Previous studies show that several of these risk factors vary by sex.1,8–9,11–25However, considerable gaps still remain in understanding the extent to which these suicide risks vary by sex, particularly among nationally representative youth. More specific knowledge is needed to direct future youth suicide-prevention strategies and to decide how limited resources can be best dispersed.
The purpose of the current study is to examine the associations between a range of risk factors and reports of suicide attempts and attempts requiring medical care in a nationally representative study of high school students. The selected and modifiable risk factors have been identified as important in previous empirical and theoretical research including the developmental–transactional model of youth suicidal behaviors6 and will be examined separately for boys and girls since the prevalence of both the risk factors and the outcome often varies by sex.1,7,8,11,16,21,26 Moreover, focusing specifically on modifiable risk factors will ensure that information from the current study can inform future prevention strategies, clinical practice and resource allocation.
METHODS
Analyses are based on cross-sectional data from the 2007 Youth Risk Behavior Survey (YRBS), which includes a nationally representative sample (n=14,041) of high school students in grades 9–12. Details of the survey have been reported elsewhere.27–28 The overall response rate for the study was 68%. Students voluntarily completed the anonymous, self-administered questionnaire in school following local parental permission procedures. The data are weighted to be representative of high school students in the U.S. IRB approval was obtained at Georgia State University to conduct these secondary data analyses.
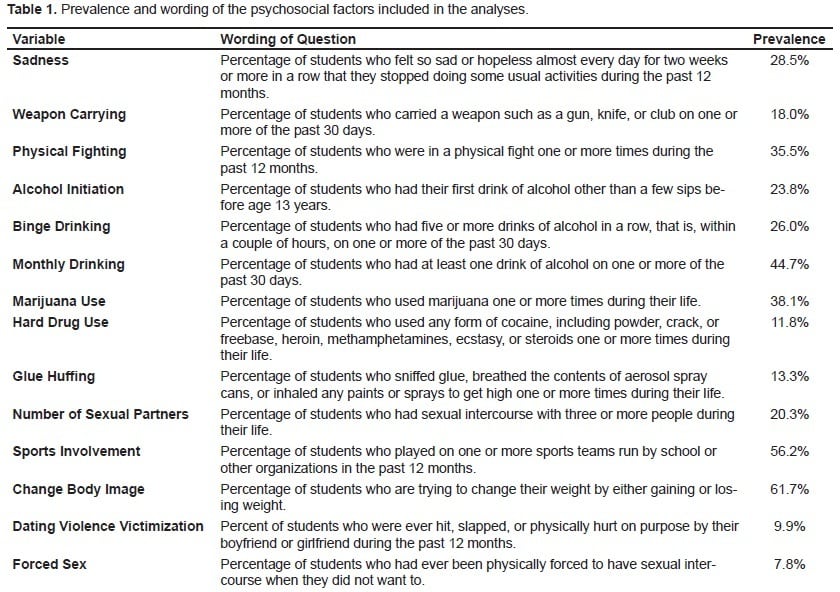
Table 1 presents the 14 psychosocial variables examined in our analysis. All of these factors were di/trichotomized and have been described elsewhere.27–28
Two outcome variables were examined: 1) “During the past 12 months, how many times did you actually attempt suicide?” (suicide attempt); 2) “If you attempted suicide during the past 12 months, did any attempt result in an injury, poisoning, or overdose that had to be treated by a doctor or nurse?” (suicide attempt requiring medical care). Both outcome variables were dichotomized into ‘No’ vs. ‘Any’ for all analyses. Associations between all previously listed risk factors and both of these outcome variables were examined separately.
Data Analysis
We computed prevalence estimates and multivariate logistic regression analyses with the SPSS (v 15.0) complex survey procedure to account for the complex sampling design. Odds Ratios (OR) were computed to evaluate the strength of the associations, and statistical significant levels were determined based on both p<0.05 and 95% confidence intervals (CIs) that did not include 1.
RESULTS
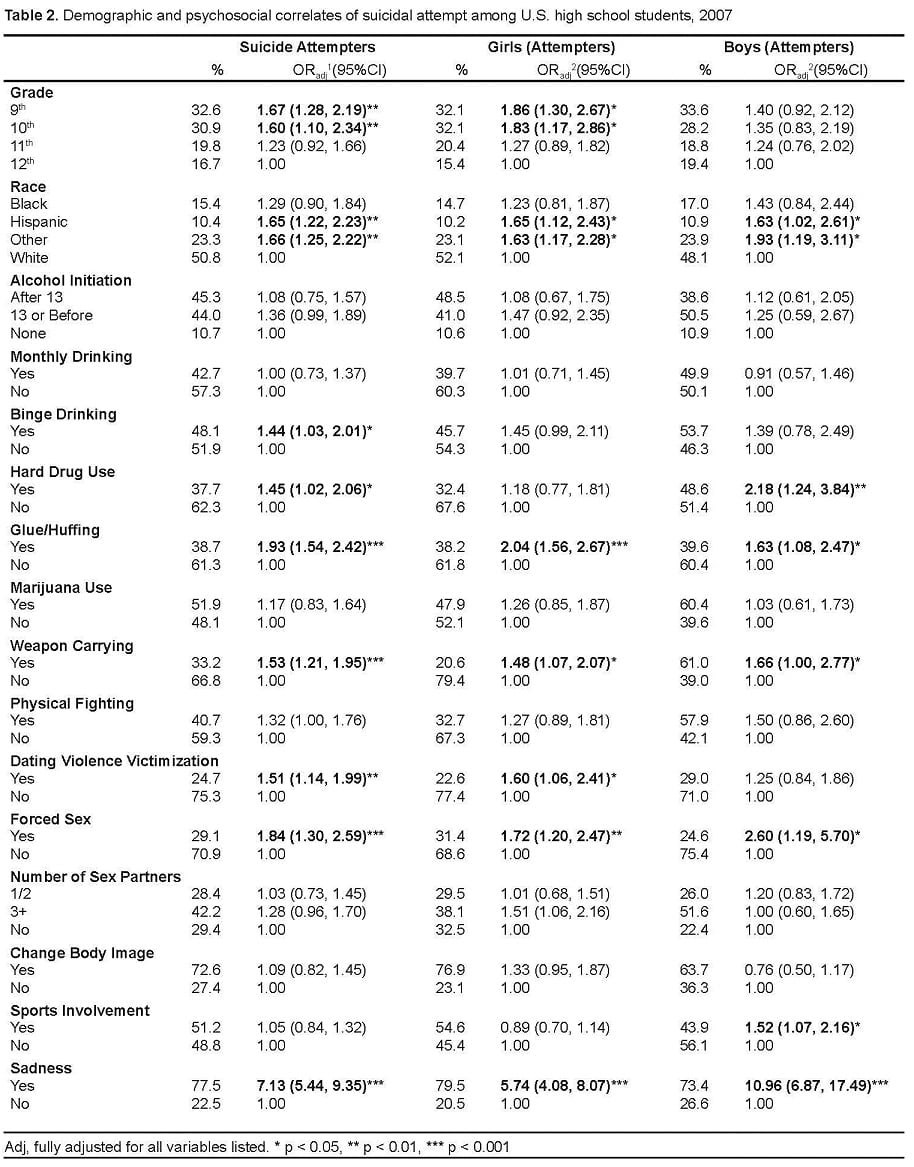
In 2007, 6.9% of high school students reported attempting suicide, and 2.0% reported a suicide attempt that required medical care. The prevalence and associations between demographic and other characteristics and suicide attempts is presented in Table 2. Overall, sadness, binge drinking, huffing glue, hard drug use, weapon-carrying, dating violence victimization, and forced sex were associated with attempting suicide. For girls, being in a younger grade, being of ‘other’ minority race or Hispanic ethnicity, sadness, huffing glue, weapon-carrying, dating violence victimization, and forced sex were significantly associated with suicide attempts. Similarly, for boys, sadness, hard drug use, glue huffing, weapon-carrying, forced sex, and sports involvement were significantly associated with suicide attempts.
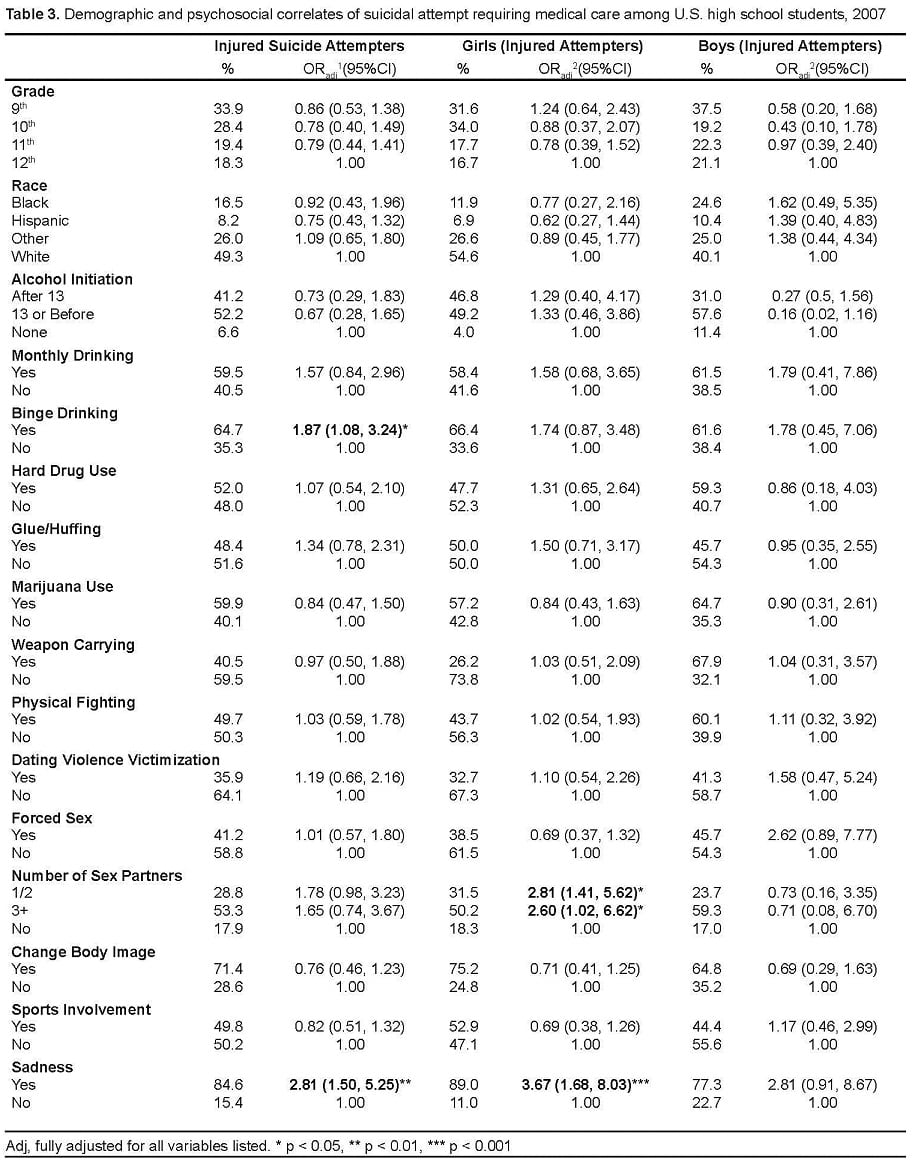
Associations between risk factors and suicide attempts requiring medical care are presented in Table 3. In these analyses, sadness and binge drinking were significantly associated with suicide attempts requiring medical care. Stratified analyses by sex show that for girls, sadness and having sex with more than two partners were significantly associated with suicide attempts requiring medical care. However, for boys, none of these risk factors were found to be significantly associated with suicide attempts requiring medical care.
DISCUSSION
This study examined the risk behaviors associated with suicide attempts and suicide attempts requiring medical care among high school students in the U.S. using recent national data. Four important findings need to be highlighted. First, the findings confirm previous research that have identified important risk factors for suicidal behaviors among youth.1,3–9,11–25 In particular, the current findings show that sadness, substance use, and violent victimization were among the most important risk factors for suicide attempts among both girls and boys. Second, this study did not find significant associations, for boys or girls, between early alcohol use initiation, monthly drinking, or binge drinking and suicide attempts which have been observed in previous research.8,24 This finding is intriguing and warrants further analyses and replication. Third, this study demonstrates that there is a range of factors contributing to suicide attempts, among both boys and girls. However, in analyses specifically of those adolescents who had attempted suicide and required medical care, few risk factors were statistically important. This finding underscores the importance for future research to consider more proximal situational and contextual factors to determine risk for injury specifically. Finally, the study highlights important sex differences in the risk factors that are important for both suicide attempts and for attempts requiring medical care. These findings need to be considered in future research, as well as in clinical practice, especially for the emergency departments (ED) where adolescent may seek care. Research shows that a suicide attempt is the strongest predictor for a future attempt and completed suicide.29–31 Therefore, appropriate clinical intervention at the time of seeking care in the ED that is designed to reduce future attempts and injuries will be needed. Moreover, researchers also must consider the need to develop and implement potentially sex-specific prevention strategies directed towards boys and girls, separately.
Overall, these findings highlight that sadness, substance use and violent victimization remain critically important factors for suicidal behaviors and should be a priority for prevention efforts. Although the study did not specifically assess health utilization or service provision, the relatively high prevalence of these risk factors examined appear to indicate high levels of unmet health needs and the importance of providing more health services to youth. Unfortunately, mental health treatment and related services are typically underfunded at all levels of government.32,33 However, these strategies need to be reconsidered within the context of adolescent health promotion and suicide prevention.
The findings also highlight that younger girls are at increased risk for suicide attempts, which may be due to transitions within adolescence as well as pubertal development. Previous research has shown that younger girls are more likely to engage in suicidal behaviors than younger boys, implicating the hormonal changes that girls undergo during puberty as the cause of this phenomenon.34
LIMITATIONS
Several limitations should be considered when interpreting the findings of this study. First, it is based on students who are attending school; therefore, the findings may not be generalizable to students who no longer attend school. Second, the data were self reported and may reflect biases and misreporting. Third, while the study included a very large sample that was also weighted to be nationally representative, the overall response rate for the survey was a relatively low 68% which may also have impacted the findings. Fourth, because of the cross-sectional survey design, the temporal ordering or any causality between the risk factors and outcome variables could not be determined. Fifth, the measures used were given equal weight and based on single indicators, not a comprehensive scale, which may further have impacted the findings. Sixth, the risk factors examined reflected different time frames, which may have also impacted the findings. Seventh, other factors not captured in the current study may also be important for suicide attempts and related injuries and should be considered in future research. Eighth, findings regarding boys who reported a suicide attempt requiring medical care should be interpreted with caution due to the smaller number of boys who actually had an attempt that required medical care (n=114). Finally, the risk factors examined in the current study were dichotomized, which could have further impacted the findings. However, dichotomization has been shown to generate findings that are both easily understandable and do not decrease the strength of association.35
CONCLUSION
These findings provide an updated view based on recent and nationally representative data of the risk factors likely to increase risk for suicide attempt or suicide attempt-related injuries among high school students. Sadness, substance use, and prior victimization were particularly strong risk factors for suicide attempts. However, important differences were noted between boys and girls. These differences should be considered in future research, clinical practice and in the design of future prevention efforts. Although youth suicide mortality has seen a slight decline over the past few years,2,14 the current findings suggest that youth suicidal behavior and related injuries remain a significant problem that need renewed resources and prevention efforts.
Footnotes
This manuscript, was prepared as part of a larger thesis, submitted as partial fulfillment of the requirements for a Masters in Public Health Degree in the Institute of Public Health, Georgia State University by the first author (Bethany West) under the guidance of the co-authors Drs. Monica Swahn and Frances McCarthy. Partial funding to support the preparation of the manuscript was obtained by Bethany West as the recipient of the Emory University’s Center for Injury Control’s Summer Scholarship with Dr. Monica Swahn as the faculty advisor.
Supervising Section Editor: Abigail Hankin, MD, MPH
Submission history: Submitted March 1, 2010; Revision Received April 15, 2010; Accepted April 15, 2010
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Bethany A. West, MPH Centers for Disease Control and Prevention 4770 Buford Highway NE, Mailstop F62 Atlanta, GA 30341
Email: bwest2@cdc.gov
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Waller MW, Hallfors DD, Halpern CT, et al. Gender differences in associations between depressive symptoms and patterns of substance use and risky behavior among a nationally representative sample of U.S. adolescents. Arch of W Men Heal. 2006;9:139–50.
2. CDC, National Center for Injury Prevention and Control Web-based Injury Statistics Query and Reporting System (WISQARS) Available at: www.cdc.gov/ncipc/wisqars Accessed March 31, 2008.
3. Swahn MH, Simon TR, Hertz MF, et al. Linking dating violence, peer violence, and suicidal behaviors among high-risk youth. Am J of Prev Med. 2008;34(1):30–8. [PubMed]
4. Department of Health and Human Services The Surgeon General’s call to action to prevent suicide.Washington, DC: Department of Health and Human Services; 1999. Available at:http://www.surgeongeneral.gov/library/calltoaction/default.htm. Accessed March 31, 2008.
5. Moscicki EK. Epidemiology of completed and attempted suicide: toward a framework for prevention. Clin Neurosci Res. 2001;1:310–23.
6. Bridge JA, Goldstein TR, Brent DA. Adolescent suicide and suicidal behavior. J Child Psychol Psychiatry. 2006;47:372–94. [PubMed]
7. Borowsky IW, Ireland M, Resnick MD. Adolescent suicide attempts: risks and protectors.Pediatrics. 2001;107:485–93. [PubMed]
8. Swahn MH, Bossarte RM. Gender, early alcohol use, and suicide ideation and attempts: findings from the 2005 Youth Risk Behavior Survey. J of Adol Heal. 2007;41:175–81.
9. Cho H, Hallfors DD, Iritani BJ. Early initiation of substance use and subsequent risk factors related to suicide among urban high school students. Addict Behav. 2007;32:1628–39. [PubMed]
10. CDC, YRBSS Online Youth online: comprehensive results interactive query system. Available at:http://apps.nccd.cdc.gov/yrbss/. Accessed March 31, 2008.
11. Kreiter SR, Krowchuk DP, Woods CR, et al. Gender differences in risk behaviors among adolescents who experience date fighting. Pediatri. 1999;104:1286–92.
12. Orr DP, Beiter M, Ingersoll G. Premature sexual activity as an indicator of psychosocial risk.Pediatri. 1991;87(2):141–7.
13. Swahn MH, Bossarte RM, Sullivent EE. Age of alcohol use initiation, suicidal behavior, and peer and dating violence victimization and perpetration among high-risk, seventh-grade adolescents.Pediatr. 2008;121(2):297–305.
14. CDC Suicide trends among youths and young adults aged 10–24 years — United States, 1990—2004. MMWR. 2007;56(35):905–8. [PubMed]
15. Adcock A, Nagy S, Simpson JA. Selected risk factors in adolescent suicide attempts. Adolesc.1991;26(104):817–27.
16. Shrier LA, Pierce JD, Emans SJ, et al. Gender differences in risk behaviors associated with forced or pressured sex. Arch Pediatr Adolesc Med. 1998;152:57–63. [PubMed]
17. Brunner R, Parzer P, Haffner J, et al. Prevalence and psychological correlates of occasional and repetitive deliberate self-harm in adolescents. Arch Pediatr Adolesc Med. 2007;161(7):641–9.[PubMed]
18. Silverman JG, Raj A, Mucci LA, et al. Dating violence against adolescent girls and associated substance use, unhealthy weight control, sexual risk behavior, pregnancy, and suicidality. JAMA.2001;286(5):572–9. [PubMed]
19. Berenson AB, Wiemann CM, McCombs S. Exposure to violence and associated health-risk behaviors among adolescent girls. Arch Pediatr Adolesc Med. 2001;155:1238–42. [PubMed]
20. Bae S, Ye R, Chen S, et al. Risky behaviors and factors associated with suicide attempt in adolescents. Arch Suicide Res. 2005;9:193–202. [PubMed]
21. Ge X, Conger RD, Elder GH., Jr Pubertal transition, stressful life events, and the emergence of gender differences in adolescent depressive symptoms. Dev Psychol. 2001;37(3):404–17. [PubMed]
22. Brady J. The associations between alcohol misuses and suicidal behavior. Alcohol Alcohol.2006;41(5):473–8. [PubMed]
23. Dunn MS, Goodrow B, Givens C, et al. Substance use behavior and suicide indicators among rural middle school students. J of School Health. 2008;78(1):26–31. [PubMed]
24. Miller JW, Naimi TS, Brewer RD, et al. Binge drinking and associated health risk behaviors among high school students. Pediatrics. 2007;119(1):76–85. [PubMed]
25. Olshen E, McVeigh KH, Wunsch-Hitzig RA, et al. Dating violence, sexual assault, and suicide attempts among urban teenagers. Arch Pediatr Adolesc Med. 2007;161(6):539–45. [PubMed]
26. Allison S, Roeger L, Martin G, et al. Gender differences in the relationship between depression and suicidal ideation in young adolescents. Aust N Z J Psychiatry. 2001;35(4):498–503. [PubMed]
27. CDC 2002 Surveillance Summaries. MMWR. 2002;51(SS–4):1–64.
28. CDC YRBS: Data user’s manual. 2007. Available at:http://www.cdc.gov/HealthyYouth/yrbs/pdf/2007_National_YRBS_Data_Users_Manual.pdf. Accessed March 31, 2008.
29. Qin P, Jepsen P, Norgard B, et al. Hospital admission for non-fatal poisoning with weak analgesics and risk for subsequent suicide: a population study. Psychol Med. 2009;39(11):1867–73. [PubMed]
30. Comtois KA. A review of interventions to reduce the prevalence of parasuicide. Psychiatr Serv.2002;53(9):1138–44. [PubMed]
31. Deykin EY, Perlow R, McNamarra J. Non-fatal suicidal and life-threatening behavior among 13- to 17-year old adolescents seeking emergency medical care. Am J Public Health. 1985;75(1):90–2.[PMC free article] [PubMed]
32. Ruiz P. The fiscal crisis in New York City: effects on the mental health care of minority populations. Am J Psychiatry. 1979;136(1):93–6. [PubMed]
33. Final budget for fiscal year 2006 changes Medicaid and Medicare rules, cuts funds for mental health programs. Psychiatr Serv. 2006;57(3):432–3. No Author. [PubMed]
34. Born L, Shea A, Steiner M. The roots of depression in adolescent girls: is menarche the key? Curr Psychiatry Rep. 2002;4(6):449–60. [PubMed]
35. Farrington DP, Loeber R. Some benefits of dichotomization in psychiatric and criminological research. Crim Behav Ment Health. 2000;10(2):100–23.