
{kind=link}
| Author | Affiliation |
|---|---|
| John Malone, DO | Madigan Army Medical Center, Department of Internal Medicine, Tacoma, Washington |
| Riley Gebner, MD | Madigan Army Medical Center, Department of Emergency Medicine, Tacoma, Washington |
| Jonathan Weyand, MD | Madigan Army Medical Center, Department of Emergency Medicine, Tacoma, Washington |
ABSTRACT
Case Presentation
A 25-year-old woman presented to the emergency department with two weeks of crampy right-flank pain, and urinary urgency and frequency. She was found to have a staghorn calculus filling her entire right renal pelvis on computed tomography imaging.
Discussion
In contrast to ureteral calculi, staghorn calculi are more commonly observed in female patients and typically present with an indolent clinical course. A low threshold for imaging should be maintained, as prompt referral to urology for stone removal or treatment is necessary. Staghorn calculi have a high likelihood of leading to renal failure or urosepsis without treatment.
CASE PRESENTATION
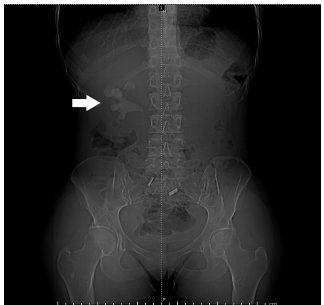
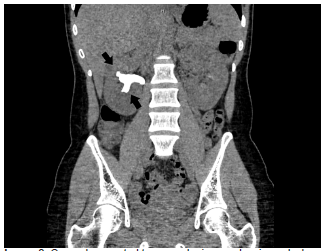
A 25-year-old Hispanic female presented to the emergency department (ED) with two weeks of waxing and waning right-sided flank pain. She described the pain as a cramping discomfort that worsened over the two weeks and was only mildly relieved by acetaminophen. She also reported urinary frequency and urgency without dysuria or hematuria. Physical examination was notable for right upper quadrant and mild right costovertebral angle tenderness. Urinalysis showed nitrite negative, leukocyte esterase positive urine with 685 white blood cells per high power field, 53 red blood cells per high power field, and appreciable bacteria. A computed tomography (CT) from the ED revealed a right staghorn calculus with hydronephrosis along with left nephrolithiasis (Images 1, 2).
DISCUSSION
Staghorn calculi are the only type of renal stones more commonly observed in female patients as a result of their association with urinary tract infections.1 Other patient characteristics associated with struvite stones include gross hematuria, lower urinary tract symptoms, fever on presentation, a past medical history of hypertension, and multiple stones on imaging.1 In contrast to nephroliths in the ureters, staghorn calculi often have an insidious course with mild or no pain; therefore, we suggest a low threshold for imaging (computed tomography or ultrasound) to accelerate definitive treatment.2 The goal of treatment is complete removal of the stone, as any remaining fragments may harbor bacteria that are difficult to sterilize with antibiotics.3,4 Without treatment, a staghorn calculus is likely to cause renal failure, urosepsis, or both.4,5 Early recognition and referral to urology is crucial to reduce the risk of morbidity and mortality in these patients.
CPC-EM Capsule
What do we already know about this clinical entity?
Struvite calculi are composed of magnesium ammonium phosphate (struvite) and calcium carbonate-apatite and are caused by urinary tract pathogens.
What is the major impact of the image(s)?
This image depicts struvite calculi within the renal pelvis and calyces giving the characteristic “staghorn” formation for which these stones are also named.
How might this improve emergency medicine practice?
As these stones are notably more insidious in presentation, earlier recognition and urgent referral will hopefully result in better outcomes for patients.
Footnotes
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
The authors attest that their institution requires neither Institutional Review Board approval, nor patient consent for publication of this case report. Documentation on file.
Address for Correspondence: Jonathan Weyand, MD, Madigan Army Medical Center, Department of Emergency Medicine, 9040 Jackson Avenue, Tacoma, WA 98431. Email: jonweyand11@yahoo.com. 5:360 – 361
Submission history: Revision received March 7, 2021; Submitted April 29, 2021; Accepted April 27, 2021
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none. The views expressed are those of the author(s) and do not reflect the official policy of the Department of the Army, the Department of Defense or the U.S. Government.
REFERENCES
1. Singh P, Enders FT, Vaughan LE, et al. Stone composition among first-time symptomatic kidney stone formers in the community. Mayo Clin Proc. 2015;90(10):1356-65.
2. Meng M, Chi T, Stoller ML. Struvite and staghorn calculi. 2021. Available at: https://emedicine.medscape.com/article/439127-overview#a10. Accessed May 22, 2020.
3. Diri A, Diri B. Management of staghorn renal stones. Ren Fail. 2018;40(1):357-62.
4. Preminger GM, Assimos DG, Lingeman JE, et al. Chapter 1: AUA Guideline on Management of Staghorn Calculi: Diagnosis and Treatment Recommendations. J Urol. 2005;173(6):1991-2000.
5. Akman T, Binbay M, Kezer C, et al. Factors affecting kidney function and stone recurrence rate after percutaneous nephrolithotomy for staghorn calculi: outcomes of a long-term followup. J Urol. 2012;187(5):1656-61.