
{kind=link}
| Author | Affiliation |
|---|---|
| Matthew A. Wheatley, MD | Emory University School of Medicine, Department of Emergency Medicine, Atlanta, Georgia; Grady Health Systems, Department of Emergency Medicine, Atlanta, Georgia |
| Shikha Kapil, MD | Georgetown University School of Medicine, Department of Emergency Medicine, Washington, District of Columbia |
| Amanda Lewis, MSSc, PA-C | Emory University School of Medicine, Department of Emergency Medicine, Atlanta, Georgia; Grady Health Systems, Department of Emergency Medicine, Atlanta, Georgia |
| Jessica Walsh O’Sullivan, MD | Emory University School of Medicine, Department of Emergency Medicine, Atlanta, Georgia; Grady Health Systems, Department of Emergency Medicine, Atlanta, Georgia |
| Joshua Armentrout, MD | Atlanta Medical Center, Department of Emergency Medicine, Atlanta, Georgia |
| Tim P. Moran, PhD | Emory University School of Medicine, Department of Emergency Medicine, Atlanta, Georgia |
| Anwar Osborne, MD, MPM | Emory University School of Medicine, Department of Emergency Medicine, Atlanta, Georgia; Grady Health Systems, Department of Emergency Medicine, Atlanta, Georgia |
| Brooks L. Moore, MD | Emory University School of Medicine, Department of Emergency Medicine, Atlanta, Georgia; Grady Health Systems, Department of Emergency Medicine, Atlanta, Georgia |
| Bryan Morse, MD | Maine Medical Center, Department of Surgery and Surgical Critical Care, Portland, Maine |
| Peter Rhee, MD | Westchester Medical Center, Department of Surgery, Trauma Surgery, and Surgical Critical Care, Valhalla, New York |
| Faiz Ahmad, MD | Emory University School of Medicine, Department of Neurosurgery, Atlanta, Georgia |
| Hany Atallah, MD | Jackson Health System, Miami, Florida |
Introduction
Methods
Results
Discussion
Limitations
Conclusion
ABSTRACT
Introduction
Traumatic intracranial hemorrhages (TIH) have traditionally been managed in the intensive care unit (ICU) setting with neurosurgery consultation and repeat head CT (HCT) for each patient. Recent publications indicate patients with small TIH and normal neurological examinations who are not on anticoagulation do not require ICU-level care, repeat HCT, or neurosurgical consultation. It has been suggested that these patients can be safely discharged home after a short period of observation in emergency department observation units (EDOU) provided their symptoms do not progress.
Methods
This study is a retrospective cross-sectional evaluation of an EDOU protocol for minor traumatic brain injury (mTBI). It was conducted at a Level I trauma center. The protocol was developed by emergency medicine, neurosurgery and trauma surgery and modeled after the Brain Injury Guidelines (BIG). All patients were managed by attendings in the ED with discretionary neurosurgery and trauma surgery consultations. Patients were eligible for the mTBI protocol if they met BIG 1 or BIG 2 criteria (no intoxication, no anticoagulation, normal neurological examination, no or non-displaced skull fracture, subdural or intraparenchymal hematoma up to 7 millimeters, trace to localized subarachnoid hemorrhage), and had no other injuries or medical co-morbidities requiring admission. Protocol in the EDOU included routine neurological checks, symptom management, and repeat HCT for progression of symptoms. The EDOU group was compared with historical controls admitted with primary diagnosis of TIH over the 12 months prior to the initiation of the mTBI protocols. Primary outcome was reduction in EDOU length of stay (LOS) as compared to inpatient LOS. Secondary outcomes included rates of neurosurgical consultation, repeat HCT, conversion to inpatient admission, and need for emergent neurosurgical intervention.
Results
There were 169 patients placed on the mTBI protocol between September 1, 2016 and August 31, 2019. The control group consisted of 53 inpatients. Median LOS (interquartile range [IQR]) for EDOU patients was 24.8 (IQR: 18.8 – 29.9) hours compared with a median LOS for the comparison group of 60.2 (IQR: 45.1 – 85.0) hours (P < .001). In the EDOU group 47 (27.8%) patients got a repeat HCT compared with 40 (75.5%) inpatients, and 106 (62.7%) had a neurosurgical consultation compared with 53 (100%) inpatients. Subdural hematoma was the most common type of hemorrhage. It was found in 60 (35.5%) patients, and subarachnoid hemorrhage was found in 56 cases (33.1%). Eleven patients had multicompartment hemorrhage of various classifications. Twelve (7.1%) patients required hospital admission from the EDOU. None of the EDOU patients required emergent neurosurgical intervention.
Conclusion
Patients with minor TIH can be managed in an EDOU using an mTBI protocol and discretionary neurosurgical consults and repeat HCT. This is associated with a significant reduction in length of stay.
INTRODUCTION
Traumatic brain injury (TBI) is a frequent cause for emergency department (ED) visits. The US Centers for Disease Control and Prevention (CDC) estimated there were 2.5 million ED visits related to TBI in 2013, which represents an increase from 2007.1 Traumatic brain injury is grossly classified as mild, moderate, and severe based on the presenting Glasgow Coma Scale (GCS) score with mild TBI (mTBI) defined as a GCS of 13–15.2
Clinical policies and decision tools exist to aid the emergency physician (EP) in deciding which patients with mTBI need brain imaging.3,4 Once traumatic intracranial hemorrhages (TIH) are identified with head computed tomography (HCT), patients are typically admitted or transferred to a trauma center with neurosurgical capabilities. This can happen regardless of the size and location of the hemorrhage, or clinical condition of the patient. Inpatient care is typically in an intensive care unit (ICU) setting so that they can be monitored closely for clinical deterioration. In addition, patients routinely receive repeat HCT and neurosurgical consultation.5
Recent studies show routine follow-up HCT in many patients are not predictive of the need for neurosurgical intervention and this practice should be reserved for patients who demonstrate deterioration of neurologic exam.6-9 Retrospective studies by Joseph et al have concluded that minor TIH patients have low risk of requiring neurosurgical intervention and, therefore, can be managed without neurosurgical consultation.10,11 Multiple studies have examined the necessity of ICU admission for minor TIH. Patients with isolated traumatic subarachnoid hemorrhage have low rates of clinical and radiographic deterioration.12-14 Other studies have suggested that patients with minor TIH largely do not receive critical care interventions and, therefore, do not benefit from ICU admission.15,16 These are retrospective analyses with no universal definition of minor TIH. Hence, the question has come up about using ED observation units (EDOU) to monitor patients with minor TIH.14,17
In their 2015 validation of the Brian Injury Guideline (BIG) protocol, Joseph et al recommended up to 24-hour observation for patients with minor TIH without repeat HCT or neurosurgical consultation.18 Minor TIH fits with other conditions commonly managed in the EDOU setting, as it is a single condition and patients can be managed in under 24 hours.19 This allows the visits to be more focused, which leads to decreased length of stay (LOS) and decreased healthcare costs.20-27 Randomized controlled trials (RCT) that have compared EDOU and inpatient care for conditions such as chest pain, asthma, atrial fibrillation, and transient ischemic attack have found EDOU care to be more efficient and cost effective.28-36 Yun and colleagues have looked at managing patients with TIH in an EDOU setting where they performed a retrospective analysis of TIH patients before and after an EDOU protocol was implemented.37 They reported that use of the protocol was associated with decreased need for admission and lower likelihood of worsening TIH on repeat CT. There was no difference in LOS in EDOU patients pre-protocol and during the protocol.
This study evaluates the outcomes of patients managed in the EDOU using an mTBI protocol based on BIG criteria.
METHODS
This is a retrospective cross-sectional study performed at a Level I trauma center. Initial workup in the acute phase of care was provided primarily by the emergency medicine (EM) team consisting of an EM attending and either an EM resident or an EM advanced practice provider. Here, the trauma team was either activated to co-manage patients based on pre-set protocols or consulted at the discretion of the EM attending.
The EDOU mTBI protocol was created by a multidisciplinary team of physicians from the trauma surgery service, EM, and neurosurgery. The EDOU protocol was based on the BIG protocol.11,18 We altered the protocol slightly to exclude epidural hematomas based on institutional expert opinion. This practice change was implemented as a quality improvement project first piloted September 1–December 31, 2016. In this phase, patients who met BIG 1 criteria (Table 1) were eligible for the EDOU protocol. Trauma and neurosurgical consultations were required for each patient. Beginning January 1, 2017, patients who met BIG 1 or 2 criteria were permitted in the EDOU. Trauma and neurosurgical consultations were at the discretion of the EM attending in all phases of care. Patients who were unable to ambulate independently, had intractable pain or vomiting, or other significant traumatic injuries were considered ineligible for EDOU. The guidelines for this protocol are summarized in Table 2.
| BIG 1 | BIG 2 | BIG 3 | |
|---|---|---|---|
| Neurological examination findings | Normal | Normal | Normal or abnormal |
| Intoxication | No | No | Yes |
| Anticoagulation | No | No | Yes |
| Skull fracture | No | Nondisplaced | Displaced |
| SDH, | ≤ 4 mm | 5–7 mm | ≥ 8 mm |
| EDH, mm | No | No | Any size |
| IPH | ≤ 4 mm, 1 location | 5–7 mm, 2 locations | ≥ 8 mm, multiple locations |
| SAH | Trace | Localized | Scattered |
| IVH | No | No | Yes |
SDH, subdural hematoma; mm, millimeters; EDH, epidural hematoma; IPH, intraparenchymal hemorrhage; SAH, subarachnoid hemorrhage; IVH, intraventricular hemorrhage.
| EDOU transfer criteria |
| Meets Brain Injury Guideline (BIG) 1 or BIG 2 criteria |
| Patient has spine cleared or is in Aspen collar and is able to ambulate without assistance |
| No other traumatic injuries that need continued evaluation or treatment. Splinted extremities are acceptable provided the patient is able to ambulate |
| Patient not having intractable pain/vomiting |
| Stable vital signs |
| Consultation in ED by trauma surgery and neurological surgery teams as deemed appropriate by ED attending |
| Exclusion criteria |
| Not meeting all of BIG 1 or BIG 2 criteria |
| Other injuries that still need evaluation/treatment |
| Inability to ambulate |
| Intractable pain/vomiting |
| Unstable vital signs (persistent tachycardia; tachypnea; hypotension) |
| Other indications for admission |
| Potential interventions |
| Serial neurologic exams including vital signs every 2 hours |
| 6–23 hour observation for change in neurological status |
| Advance diet as tolerated |
| Antiemetics/analgesics as needed |
| Repeat CT as indicated |
| Decision points/acute interventions |
| STAT repeat CT head and call to neurosurgery and trauma residents on call for |
| Decreased mental status based on Q2 hour checks |
| Seizure at any point |
| New focal neurologic deficits found on neuro checks |
| STAT trauma evaluation for: |
| Development of abnormal vital signs |
| Intractable pain |
| Inability to ambulate |
| Discharge criteria |
| Home |
| Acceptable vital signs |
| Normal serial neurologic exams |
| Tolerating diet as they were prior to admission |
| Able to ambulate and perform activities of daily living without assistance |
| Admit |
| Deterioration in clinical condition |
| Development of any exclusion criteria – including over read of initial CT head that includes BIG 2 or 3 criteria |
ED, emergency department; CT, computed tomography.
Interventions in the EDOU consisted of neurologic checks every two hours for up to 23 hours. These standard assessments, performed by nursing, involve testing for level of alertness, orientation, and gross deficits in limbs. Evidence of decreased mental status, seizure, or focal neurologic deficit prompted an emergent repeat HCT and consultation with both trauma surgery and neurosurgery. Symptoms were controlled with antiemetics and analgesics as needed. In the absence of clinical deterioration, repeat HCT was ordered at the discretion of the EDOU team. Patients were discharged home if symptoms were controlled with oral medication and they were able to eat and perform activities of daily living unassisted. Patients who were unable to do this were converted to inpatient status. They were admitted to the trauma service if they needed further treatment for their head injuries. Some were admitted to internal medicine due to occult medical issues that were identified during observation.
The intervention group was identified through an EDOU census report generated through the electronic health record (EHR). Because the EHR allowed use of the discrete variable “EDOU Pathway” it was not necessary to use International Classification of Diseases, 10th Modification (ICD-10) codes to identify all the patients in the EDOU on this pathway. The database was queried for all patients on the mTBI protocol from its inception on September 1, 2016, through August 31, 2019. The report provides patient level ED and EDOU LOS data as well as final disposition: inpatient conversion or discharge from EDOU. Trained chart abstractors (EM residents) obtained age, gender, mechanism of injury, initial HCT reading by radiologist, TIH category as determined by trauma surgeons, disposition from the EDOU (be it admission or discharge to home), and follow-up information. Length of stay for the intervention group was calculated on the EHR report unless specified below. We defined ED LOS as patient arrival until they physically left the department. Length of stay in the EDOU was calculated as time of arrival in the EDOU until the time of the admission or discharge order in the EHR. Admission and discharge order times were manually abstracted via chart review. Total LOS was calculated as the sum of ED and EDOU LOS.
The comparison group was made up of patients admitted to the trauma service for TIH from September 1, 2015–August 31, 2016. Patients were identified by querying the trauma registry for all patients who were admitted with a primary diagnosis of TIH based on ICD-10 code. The trauma registry is a database maintained by the Trauma and Acute Care Surgery service. Minor TBI inclusion criteria were retrospectively applied to these patients to select the group that would have been eligible for EDOU. Trained chart abstractors obtained demographic, imaging, disposition, and follow-up information on comparison group patients. Although the group for comparison was derived from the registry database at our institution and the intervention group was derived from an EHR report, ultimately the chart abstractors used the same EHR system (Epic Systems Corporation, Verona, WI) to obtain the results used in the analyses.
We described LOS using medians and interquartile ranges. All other variables were described using counts and percentages. The primary research question regarded whether the mTBI protocol reduced the median LOS. This was tested using quantile regressions. Quantile evaluates the association between some predictor and a given quantile/percentile of the outcome while controlling for other variables (eg, whether an intervention reduces the 50th percentile/median or 75th percentile of an outcome). Adjusted analyses controlled for the effects of age, gender, mechanism of injury, neurosurgery consultation, repeat HCT, and BIG level. We computed P-values and 95% confidence intervals (CI) as bootstrapped estimates (10,000 resamples). Categorical patient characteristics were compared across groups using the χ2 test. Analyses were conducted using R v. 3.5.2 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
During the study period 209 patients were placed on the mTBI protocol. We excluded 40 patients from this analysis because they did not have an acute TIH or were admitted as inpatients to the trauma service but boarding in the EDOU. The control group consisted of 53 patients. Demographic and clinical information for the intervention and comparison groups are summarized in Table 3.
| Characteristic | Control (n = 53) | Intervention (n = 169) | P |
|---|---|---|---|
| Age | 36 (26.5 – 55) | 41 (27.5 – 57) | .39 |
| Gender | .34 | ||
| Male | 35 (66.0) | 98 (58.0) | |
| Female | 18 (34.0) | 71 (42.0) | |
| Mechanism | .08 | ||
| Assault | 15 (28.3) | 26 (15.4) | |
| Bike/ATV/Scooter | 1 (1.9) | 8 (4.7) | |
| Fall | 10 (18.9) | 57 (33.7) | |
| MVC | 20 (37.7) | 67 (39.6) | |
| Ped vs Vehicle | 4 (7.5) | 7 (4.1) | |
| Other | 3 (5.7) | 4 (2.4) | |
| Big Protocol | .40 | ||
| 1 | 41 (77.4) | 135 (79.9) | |
| 2 | 12 (22.6) | 30 (17.8) | |
| 3 | 0 (0) | 4 (2.4) | |
| NSGY | 53 (100) | 106 (62.7) | <.001 |
| Repeat HCT | 40 (75.5) | 46 (27.4) | <.001 |
| LOS | 60.2 (45.1 – 85.0) | 24.8 (18.8 – 29.9) | <.001 |
ATV, all terrain vehicle; MVC, motor-vehicle collision; Ped, pedestrian; NSGY, neurosurgery; HCT, head computed tomography; LOS, length of stay.
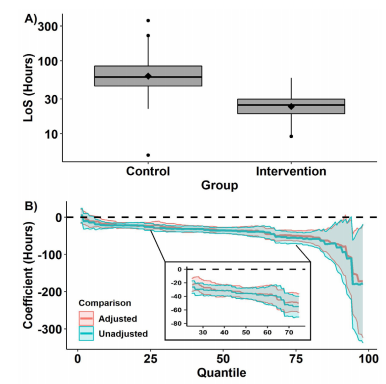
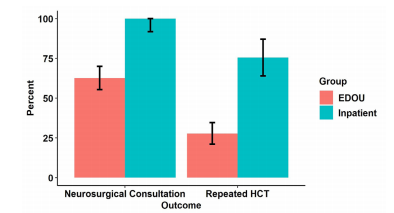
The primary outcome is presented in Figure 1. Median LOS (IQR) for EDOU patients was 24.8 (IQR: 18.8 – 29.9) hours compared with a median LOS for the comparison group of 60.2 (IQR: 45.1 – 85.0) hours. This 35.4 (95% CI, 27.3 – 43.5) hour reduction was significant (P < .001). In the adjusted analyses, the intervention was associated with a 35.5 (95% CI, 27.2 – 43.8, P < .001) hour reduction is LOS. In the EDOU group 47 (27.8%) patients got a repeat HCT compared with 40 (75.5%) inpatients, and 106 (62.7%) had a neurosurgical consultation compared with 53 (100%) inpatients (Figure 2). Subdural hematoma was the most common type of hemorrhage. It was found in 60 (35.5%) of patients, and subarachnoid hemorrhage was found in 56 cases (33.1%). Eleven patients had multicompartment hemorrhage of various classifications.
Twelve (7.1%) patients required hospital admission from the EDOU. Reasons for admission are explained in Table 4. Average inpatient LOS was 3.25 days. Only three patients required ICU care, and four were admitted to the internal medicine service. Ten of the admitted patients were able to be discharged home following their hospitalization. One patient was transferred to hospice, and one was discharged to rehab. None of the patients managed in the EDOU required neurosurgical intervention. There was only one patient death in the EDOU group. Based on review of clinical records, this was thought to be due to metabolic encephalopathy and not head injury.
| Patient number | Age/gender | HCT finding | Reason for admission | Type of bed | Inpatient LOS |
|---|---|---|---|---|---|
| 15 | 25/F | Trace SAH (overread as negative) | Persistent tachycardia | Trauma floor | 2 days |
| 16 | 59/M | Subacute subdural | Dizziness, bradycardia | Medical telemetry | 4 days |
| 17 | 25/F | Trace SAH | Vomiting, worsening CT | Trauma ICU | 2 days |
| 22 | 31/F | Trace SAH vs artifact | Pain control | Trauma floor | 3 days |
| 58 | 40/M | Subdural skull fracture | Worsening CT | Trauma ICU | 5 days |
| 107 | 51/M | Scattered punctate hyperdensities likely artifact | Persistent Confusion | Trauma floor | 6 days |
| 108 | 79/F | 4mm SDH | Gait instability | Trauma floor | 2 days |
| 114 | 77/M | 3mm SDH | Worsening mental status | Medical ICU | 11 days |
| 115 | 77/M | Small SAH vs artifact | New atrial flutter | Medical telemetry | 1 day |
| 119 | 90/F | Trace SAH | Unable to ambulate | Medical floor | 1 day |
| 133 | 27/F | Streak artifact vs hemorrhagic contusion | Dizziness | Trauma floor | 1 day |
| 134 | 18/F | R frontal SAH, R IPH | CT over-read | Trauma floor | 1 day |
HCT, head computed tomography; LOS, length of stay; M, male; F, female; SAH, subarachnoid hemorrhage; mm, millimeters; ICU, intensive care unit; SDH, subdural hematoma; IPH, intraparenchymal hemorrhage.
Follow-up information was available on only 45 (26.6%) patients. Twelve patients reported mild symptoms of headache or dizziness. One patient had persistent headache three months later. No patients required readmission or neurosurgical intervention due to their head injuries. Two patients were called back to the ED due to CT over-reads. Neither of these visits resulted in an admission. Seven patients received outpatient imaging due to persistent symptoms, but no neurosurgical intervention was required for these patients.
DISCUSSION
We found a significant difference in our primary outcome of EDOU vs inpatient LOS. Management of patients with mTBI in the EDOU was associated with significant reduction in LOS when compared with patients in inpatient settings. This is consistent with the above studies on EDOU vs inpatient care. This finding differs somewhat from the EDOU study by Yun et al in that they did not compare EDOU and inpatient data, but rather the LOS in the ED portion of care only.37 This difference is not as surprising as the preponderance of other studies showing benefit in LOS for EDOU pathways when compared to usual care in an inpatient setting.
Overall, our protocol is similar to the one reported in the Yun study. There were minor differences in inclusion criteria such as the upper limit of subdural hematoma. Interventions in the EDOU were similar between the two groups including frequent neurologic checks and repeat HCT for clinical deterioration. In addition, we found a low rate of adverse events in the EDOU group, which is consistent with previous studies on minor TIH. None of the patients in the intervention group required emergent neurosurgical intervention. The most common reasons for inpatient admission were persistent symptoms due to head injury or other traumatic or medical issues that presented during the observation period. This is summarized in Table 4. Further study is needed to determine predictors for inpatient conversion in this group.
Patients in the EDOU had a lower rate of neurosurgical consultation and repeat HCT when compared with their inpatient counterparts. Repeat HCTs were ordered based on clinical concern or recommendations from radiology or neurosurgical consultants. Further study is needed to determine the clinical necessity of these interventions in the EDOU setting.
LIMITATIONS
There are many limitations to this study given its single-center, retrospective design. A large, multicenter RCT is needed to better understand the true relationship between EDOU care and LOS. In addition, because adverse outcomes in BIG 1 and 2 class TIH are rare, larger numbers are needed to truly understand the safety of this approach. However, because TIH patient are a high-risk population a more precise understanding of the rates of hemorrhage progression and need for emergent neurosurgical intervention is essential before EDOU care can be widely recommended.
The biggest limitation of this study is the limited follow-up information in the intervention group. Because this study began as a quality improvement initiative, there initially was not a robust mechanism to conduct follow-up interviews to investigate whether patients were still experiencing symptoms or had repeated medical visits due to their injuries. This is an important area for future study. Patients were chosen for the EDOU based on clinician gestalt that the patient fit within the inclusion/exclusion guidelines. This could introduce bias into the results as patients who were thought to be sicker or more complicated were likely admitted to inpatient units. The control group for this study is small and thus may limit the strength of association of some of the outcomes. This study was conducted in an urban teaching facility and Level 1 trauma center; thus, it may not be translatable to smaller or rural centers without trauma or neurosurgical services. Further studies involving non-Level I trauma centers are necessary.
CONCLUSION
Use of an EDOU to observe patients with minor traumatic hemorrhage as defined by the Brain Injury Guidelines classification was associated with significantly reduced length of stay and low overall incidence of adverse events. Care in the ED observation unit was also associated with fewer repeat head computed tomography and neurosurgical consultations. Further study is needed to determine predictors for inpatient conversion, follow-up needs, and ability of smaller, non-trauma centers to use this protocol.
Population Health Research Capsule
What do we already know about this issue?
Patients with small traumatic intracranial hemorrhages (TIH) often utilize intensive care, serial head computed tomographies (CT) and neurosurgical consultation, even though they rarely benefit from these resources.
What was the research question?
Can management of patients with minor traumatic intracranial hemorrhages be accomplished in emergency department observational units (EDOUs) and use fewer resources?
What was the major finding of the study?
Minor TIH patients in EDOUs are associated with a shorter length of stay, fewer repeat CTs and neurosurgical consults.
How does this improve population health?
Stable patients with small traumatic hemorrhages may not benefit from more interventions and critical care. This could lead to cost savings for this group of patients.
Footnotes
Section Editor: Patrick Maher, MD, MS
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Matthew A Wheatley, MD, Emory University School of Medicine, Department of Emergency Medicine, 201 Dowman Drive, Atlanta, Georgia 30322. Email: mwheatl@emory.edu. 7 / 2021; 22:943 – 950
Submission history: Revision received October 27, 2020; Submitted April 15, 2021; Accepted April 21, 2021
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. No author has professional or financial relationships with any companies that are relevant to this study. There are no conflicts of interest or sources of funding to declare.
REFERENCES
1. Taylor CA, Bell JM, Breiding MJ, et al. Traumatic brain injury-related emergency department visits, hospitalizations, and deaths – United States, 2007 and 2013. MMWR Surveill Summ. 2017;66(9):1-16.
2. Carroll LJ, Cassidy JD, Holm L, et al. Methodological issues and research recommendations for mild traumatic brain injury: the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. J Rehabil Med. 2004(43 Suppl):113-25.
3. Jagoda AS, Bazarian JJ, Bruns JJ, et al. Clinical policy: neuroimaging and decisionmaking in adult mild traumatic brain injury in the acute setting. Ann Emerg Med. 2008;52(6):714-48.
4. Stiell IG, Clement CM, Rowe BH, et al. Comparison of the Canadian CT Head Rule and the New Orleans Criteria in patients with minor head injury. JAMA. 2005;294(12):1511-8.
5. Wang MC, Linnau KF, Tirschwell DL, et al. Utility of repeat head computed tomography after blunt head trauma: a systematic review. J Trauma. 2006;61(1):226-33.
6. Stippler M, Smith C, McLean AR, et al. Utility of routine follow-up head CT scanning after mild traumatic brain injury: a systematic review of the literature. Emerg Med J. 2012;29(7):528-32.
7. Joseph B, Aziz H, Pandit V, et al. A three-year prospective study of repeat head computed tomography in patients with traumatic brain injury. J Am Coll Surg. 2014;219(1):45-51.
8. Brown CV, Weng J, Oh D, et al. Does routine serial computed tomography of the head influence management of traumatic brain injury? A prospective evaluation. J Trauma. 2004;57(5):939-43.
9. Chao A, Pearl J, Perdue P, et al. Utility of routine serial computed tomography for blunt intracranial injury. J Trauma. 2001;51(5):870-5.
10. Joseph B, Aziz H, Sadoun M, et al. The acute care surgery model: managing traumatic brain injury without an inpatient neurosurgical consultation. J Trauma Acute Care Surg. 2013;75(1):102-5.
11. Joseph B, Friese RS, Sadoun M, et al. The BIG (brain injury guidelines) project: defining the management of traumatic brain injury by acute care surgeons. J Trauma Acute Care Surg. 2014;76(4):965-9.
12. Pruitt P, Penn J, Peak D, et al. Identifying patients with mild traumatic intracranial hemorrhage at low risk of decompensation who are safe for ED observation. Am J Emerg Med. 2017;35(2):255-9.
13. Borczuk P, Penn J, Peak D, et al. Patients with traumatic subarachnoid hemorrhage are at low risk for deterioration or neurosurgical intervention. J Trauma Acute Care Surg. 2013;74(6):1504-9.
14. Phelan HA, Richter AA, Scott WW, et al. Does isolated traumatic subarachnoid hemorrhage merit a lower intensity level of observation than other traumatic brain injury?. J Neurotrauma. 2014;31(20):1733-6.
15. Washington CW, Grubb RL. Are routine repeat imaging and intensive care unit admission necessary in mild traumatic brain injury?. J Neurosurg. 2012;116(3):549-57.
16. Nishijima DK, Haukoos JS, Newgard CD, et al. Variability of ICU use in adult patients with minor traumatic intracranial hemorrhage. Ann Emerg Med. 2013;61(5):509-17.e4.
17. Fabbri A, Servadei F, Marchesini G, et al. Observational approach to subjects with mild-to-moderate head injury and initial non-neurosurgical lesions. J Neurol Neurosurg Psychiatry. 2008;79(10):1180-5.
18. Joseph B, Pandit V, Haider AA, et al. Improving hospital quality and costs in nonoperative traumatic brain injury: the role of acute care surgeons. JAMA Surg. 2015;150(9):866-72.
19. Ross MA, Aurora T, Graff L, et al. State of the art: emergency department observation units. Crit Pathw Cardiol. 2012;11(3):128-38.
20. Ross MA, Hockenberry JM, Mutter R, et al. Protocol-driven emergency department observation units offer savings, shorter stays, and reduced admissions. Health Aff (Millwood). 2013;32(12):2149-56.
21. Wright B, Zhang X, Rahman M, et al. Informing Medicare’s Two-Midnight Rule Policy with an analysis of hospital-based long observation stays. Ann Emerg Med. 2018;72(2):166-70.
22. Baugh CW, Venkatesh AK, Hilton JA, et al. Making greater use of dedicated hospital observation units for many short-stay patients could save $3.1 billion a year. Health Aff (Millwood). 2012;31(10):2314-23.
23. Baugh CW, Venkatesh AK, Bohan JS. Emergency department observation units: a clinical and financial benefit for hospitals. Health Care Manage Rev. 2011;36(1):28-37.
24. Schuur JD, Venkatesh AK. The growing role of emergency departments in hospital admissions. N Engl J Med. 2012;367(5):391-3.
25. Baugh CW, Schuur JD. Observation care: high-value care or a cost-shifting loophole?. N Engl J Med. 2013;369(4):302-5.
26. Schrager J, Wheatley M, Georgiopoulou V, et al. Favorable bed utilization and readmission rates for emergency department observation unit heart failure patients. Acad Emerg Med. 2013;20(6):554-61.
27. Baugh CW, Liang LJ, Probst MA, et al. National cost savings from observation unit management of syncope. Acad Emerg Med. 2015;22(8):934-41.
28. Gomez MA, Anderson JL, Karagounis LA, et al. An emergency department-based protocol for rapidly ruling out myocardial ischemia reduces hospital time and expense: results of a randomized study (ROMIO). J Am Coll Cardiol. 1996;28(1):25-33.
29. Roberts RR, Zalenski RJ, Mensah EK, et al. Costs of an emergency department-based accelerated diagnostic protocol vs hospitalization in patients with chest pain: a randomized controlled trial. JAMA. 1997;278(20):1670-6.
30. McDermott MF, Murphy DG, Zalenski RJ, et al. A comparison between emergency diagnostic and treatment unit and inpatient care in the management of acute asthma. Arch Intern Med. 1997;157(18):2055-62.
31. Farkouh ME, Smars PA, Reeder GS, et al. A clinical trial of a chest-pain observation unit for patients with unstable angina. Chest Pain Evaluation in the Emergency Room (CHEER) Investigators. N Engl J Med. 1998;339(26):1882-8.
32. Rydman RJ, Isola ML, Roberts RR, et al. Emergency department observation unit versus hospital inpatient care for a chronic asthmatic population: a randomized trial of health status outcome and cost. Med Care. 1998;36(4):599-609.
33. Shen WK, Decker WW, Smars PA, et al. Syncope Evaluation in the Emergency Department Study (SEEDS): a multidisciplinary approach to syncope management. Circulation. 2004;110(24):3636-45.
34. Ross MA, Compton S, Medado P, et al. An emergency department diagnostic protocol for patients with transient ischemic attack: a randomized controlled trial. Ann Emerg Med. 2007;50(2):109-19.
35. Decker WW, Smars PA, Vaidyanathan L, et al. A prospective, randomized trial of an emergency department observation unit for acute onset atrial fibrillation. Ann Emerg Med. 2008;52(4):322-8.
36. Sun BC, McCreath H, Liang LJ, et al. Randomized clinical trial of an emergency department observation syncope protocol versus routine inpatient admission. Ann Emerg Med. 2014;64(2):167-75.
37. Yun BJ, Borczuk P, Wang L, et al. Evaluation of a low-risk mild traumatic brain injury and intracranial hemorrhage emergency department observation protocol. Acad Emerg Med. 2018;25(7):769-75.