
{kind=link}
| Author | Affiliation |
|---|---|
| Jake Toy, DO | Harbor-UCLA Medical Center, Department of Emergency Medicine, Torrance, California |
| Alexander Garrett, MD | Harbor-UCLA Medical Center, Department of Emergency Medicine, Torrance, California |
| Yiju Teresa Liu, MD | Harbor-UCLA Medical Center, Department of Emergency Medicine, Torrance, California |
ABSTRACT
A 52-year-old man without known medical history presented with painful, progressive, bilateral lower extremity edema over a two-week period. An abdominal exam noted a firm left upper quadrant mass. Emergency department (ED) point-of-care ultrasound (POCUS) revealed a hyperechoic, heterogeneous structure in the inferior vena cava that was determined to represent a tumor thrombus extending from a primary renal cell carcinoma. This case demonstrates how POCUS was valuable in rapidly diagnosing this rare cause of lower extremity edema and its usefulness in directing the initial ED management of this patient.
CASE PRESENTATION
A 52-year-old man with no medical history presented to the emergency department (ED) with painful, progressive, bilateral lower extremity edema over a two-week period. The patient also had the following complaints: difficulty with ambulation; blood in his urine; dull, left lower quadrant abdominal pain for one month; and an 80-pound weight loss over two years. Vital signs were within normal limits. Palpation of the abdomen revealed a large, firm mass in the left upper quadrant and 2+ pitting edema in the bilateral lower extremities up to the mid-shin. Point-of-care ultrasound (POCUS) of the heart and lower extremities were unremarkable. Abdominal POCUS revealed a hyperechoic, heterogeneous structure in the inferior vena cava (IVC) (Image 1 and Video).

DISCUSSION
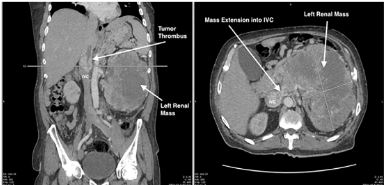
ED POCUS revealed a hyperechoic, heterogeneous structure in the IVC representing a tumor thrombus, which often results after intravascular extension of a primary tumor. This occurs most commonly in the setting of the following: renal cell carcinoma (RCC); hepatocellular carcinoma; Wilms tumor; and adrenal cortical carcinoma.1 Computed tomography demonstrated continuity between a large heterogeneous left kidney mass and tumor thrombus in the IVC (Image 2). The patient was ultimately diagnosed with high-grade clear cell RCC with tumor thrombus extension into the IVC likely resulting in his bilateral leg swelling.
To date, no previous images in the literature have demonstrated POCUS identification of an IVC tumor thrombus in the ED. Radiology literature dating back to the 1980s attempted to characterize known IVC tumor thrombi with ultrasound.2 In emergency medicine literature, two case reports describe the detection of IVC thrombosis during an ED POCUS exam, although neither was associated with extension from intra-abdominal malignancy.3,4 In this case, POCUS allowed clinicians to quickly identify the likely etiology of this patient’s lower extremity swelling, and guided initial clinical management and additional advanced imaging decisions.
CPC-EM Capsule
What do we already know about this clinical entity?
No known reports to date have published images depicting an inferior vena cava (IVC) tumor thrombus detected on emergency department point-of-care ultrasound (POCUS).
What is the major impact of the image(s)?
This case describes how POCUS was used to rapidly identify an IVC tumor thrombus as the etiology of bilateral lower leg swelling, which in turn guided initial management.
How might this improve emergency medicine practice?
The case emphasizes that POCUS is an effective and versatile tool to make rapid diagnoses in the emergency department.
Footnotes
Section Editor: Shahram Lotfipour, MD,MPH
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
Address for Correspondence:Jake Toy, DO, Harbor-UCLA Medical Center, Department of Emergency Medicine, 1000 W Carson St., Building D9, Torrance, CA 90509. Email: jake.toy@gmail.com. 3:451 – 452
Submission history: Revision received May 9, 2019; Submitted August 9, 2019; Accepted September 6, 2019
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Quencer KB, Friedman T, Sheth R, et al. Tumor thrombus: incidence, imaging, prognosis and treatment. Cardiovasc Diagn Ther. 2017;7(Suppl 3):S165-77.
2. Pussell SJ, Cosgrove DO. Ultrasound features of tumour thrombus in the IVC in retroperitoneal tumours. Br J Radiol. 1981;54(646):866-9.
3. Yanuck J, Ghanem G, Lahham S. Detection of inferior vena cava thrombosis extending into the right atrium using point-of-care ultrasound. Clin Pract Cases Emerg Med. 2019;3(1):67-8.
4. Lahham S, Tsai L, Wilson SP, et al. Thrombosis of inferior vena cava diagnosed using point-of-care ultrasound after pediatric near-syncope. J Emerg Med. 2016;51(4):e89-91.
SUPPLEMENTARY MATERIAL
Point-of-care ultrasound of the abdomen.