
{kind=link}
| Author | Affiliation |
|---|---|
| Deena Ibrahim, MD | University of California, Irvine, Department of Emergency Medicine, Irvine, CA |
| Nina P. Patel | Stanford University School of Medicine, Stanford CA |
| Malkeet Gupta, MD, MS | University of California, Los Angeles, Department of Emergency Medicine, Westwood, CA |
| J Christian Fox, MD | University of California, Irvine, Department of Emergency Medicine, Irvine, CA |
| Shahram Lotfipour, MD, MPH | University of California, Irvine, Department of Emergency Medicine, Irvine, CA |
ABSTRACT
Introduction:
Intussusception is a condition found primarily in the pediatric population. In the adult population, however, intussusception is usually due to a pathological process, with a higher risk of bowel obstruction, vascular compromise, inflammatory changes, ischemia, and necrosis. Radiographic and sonographic evidence can aid in the diagnosis. Surgical intervention involving resection of affected bowel is the standard of care in adult cases of intussusception.
Case Report:
We present the case of a 21-year-old female who presented to the Emergency Department with diffuse cramping abdominal pain and distention. Workup revealed ileocecal intussusception, with a prior appendectomy scar serving as the lead point discovered during exploratory laparotomy. We also present the case of a 66-year-old male, who presented with one week of intermittent lower abdominal pain associated with several episodes of nausea and vomiting. Workup revealed ileocolic intussusception secondary to adenocarcinoma of the right colon, confirmed upon exploratory laparotomy with subsequent right hemicolectomy.
Conclusion:
In the adult population, intussusception is usually caused by a lead point, with subsequent telescoping of one part of the bowel into an adjacent segment. While intussusception can occur in any part of the bowel, it usually occurs between a freely moving segment and either a retroperitoneal or an adhesion-fixed segment. The etiology may be associated with pathological processes such as carcinoma or iatrogenic causes, such as scars or adhesions from prior surgeries. The cases presented here demonstrate important etiologies of abdominal pain in adult patients. Along with gynecological etiologies of lower quadrant abdominal pain in female patients, it is important for the emergency physician to expand the differential diagnosis to include other causes, such as intussusceptions, especially given the symptoms that could be associated with bowel obstruction.
INTRODUCTION
Intussusception is a rare cause of abdominal pain in the adult population, accounting for five percent of intussusception cases in all ages and 1–5% of intestinal obstruction.1 The clinical presentation in adults is often nonspecific, including abdominal pain and distention, nausea, vomiting, gastrointestinal bleeding and change in bowel movements.1–4 We present two cases of adult intussusception and then discuss diagnostic modalities, etiologies and treatment strategies.
Case 1
A 21-year-old female presented to the emergency department (ED) with a seven-hour history of distension and worsening diffuse cramping abdominal pain, greatest in the right lower quadrant. The pain was rated as a seven out of ten, with no aggravating or alleviating factors. It was associated with diarrhea and flatus. Her last meal was the night prior to presentation to ED. In the ED, the patient had six bowel movements. She denied any history of similar episodes of pain, as well as fever, chills, nausea, vomiting, weight gain or loss.
The patient’s medical history was significant for systemic lupus erythematous, patent foramen ovale, arteriovenous malformation of the lung status post coiling embolization, antiphospholipid syndrome and splenic and hepatic infarcts resulting in portal vein thrombosis requiring anticoagulation. The patient’s past surgical history was significant for an appendectomy. The patient was a gravida 1, para 1, status post natural spontaneous vaginal delivery, without any complications, approximately three months prior to her presentation. She denied history of sexually transmitted diseases or multiple sexual partners. Medications included Plaquenil, Coumadin, Prednisone, Ferrous Sulfate, Azathioprine, and Zoloft. She denied any tobacco, alcohol or illicit drug use.
On examination, her vital signs were included: temperature of 36.6 degrees Celsius, heart rate of 58 beats per minute, blood pressure of 96/58 mm Hg, respiratory rate of 16 breaths per minute, and oxygen saturation of 97% on room air. She appeared moderately ill, in apparent discomfort but no acute distress. Abdominal examination revealed diffuse tenderness on palpation, particularly in the right lower quadrant, tenderness to percussion, and high-pitched bowel sounds. A pelvic speculum exam revealed a normal cervix with no erythema or discharge. Bimanual exam revealed normal-sized uterus, with no adnexal masses and no tenderness to palpation. Her physical exam was otherwise benign.
The patient’s workup included a white blood cell count of 6.2 thous/mcL (reference range: 4.0–10.5) and elevated liver enzymes with aspartate aminotransferase (AST) of 66 IU/L (reference range: 8–40) and alanine aminotransferase (ALT) of 115 IU/L (reference range: 0–60). Normal total bilirubin was 0.4mg/dL (reference range: 0–1.4) and normal alkaline phosphatase was 50 IU/L (reference range: 26–110). Prothrombin time (PT) and international normalized ratio (INR) were elevated at 15.2 (reference range: 9.6–11.8) and 1.31 (reference range: 0.89–1.11), respectively. Partial thromboplastin time (PTT) was normal at 28.6 (reference range: 24.2–32.6). Urine analysis was negative for urinary tract infection. Urine pregnancy test was negative. Abdominal and pelvic duplex ultrasounds were unremarkable. Computed tomography (CT) scan of abdomen and pelvis showed a target lesion in right lower quadrant with obstruction of contrast and pericolonic fat stranding indicative of intussusception at the ileocecal junction.
An acute care surgery consultation resulted in an exploratory laparotomy and ileocecectomy with primary repair. In the operating room, the intussuscepted portion appeared to be at the site of previous appendectomy scar, thickened cecum intussuscepted within itself. Patient tolerated the procedure well with minimal blood loss and no complications. The specimen showed a well-healed scar, measuring 0.7 cm in length and 0.1 cm in diameter. Specimen pathology revealed pseudomembranous colitis involving the cecum and inflammatory debris in the terminal ileum, eight reactive lymph nodes, without evidence of well-formed granulomas, vasculitis, polyps or malignancy. Post-operative course was unremarkable with normalization of liver enzymes, advancement of diet and return of normal bowel function. The patient was discharged three days after the operation.
Case 2
A 66-year-old male presented to the ED with a four-day history of intermittent lower abdominal pain associated with several episodes of nausea, vomiting, and diarrhea. He described the pain as dull and heavy, worse with lying on his back and better when he laid on his side, without prior episodes of similar pain. Review of symptoms was negative for fever, chills, weight loss, black or bloody stools, change in bowel caliber, urinary symptoms, recent travel, camping or unusual foods. He had no recent sick contacts. His past medical history included degenerative joint disease and a past surgical history of an appendectomy. He had no family history and a social history of cigarette smoking only.
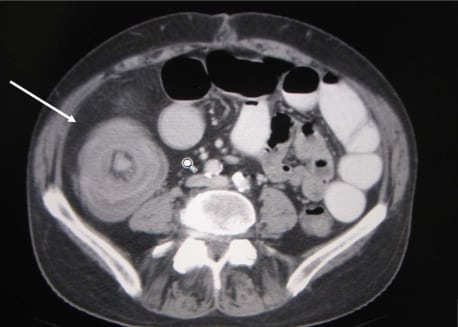
Initial vital signs were within normal limits: temperature 98 degrees Celsius, blood pressure of 122/82 mm Hg, heart rate of 98 beats per minute, respiratory rate of 18 breaths per minute, and oxygen saturation of 97% on room air. Initial exam revealed a patient in mild distress and an exam significant only for moderate suprapubic tenderness without rebound or guarding. There were no masses or hepato-splenomegaly appreciated. In addition, bowel sounds were normal. Initial lab tests including a complete blood count, chemistry panel, urinalysis and coagulation profile were significant only for a WBC count of 19,000 cells/L (70% neutrophils, 18% lymphocytes, 9% monocytes, 3% basophils) and a hematocrit of 39%. CT scan of the abdomen and pelvis revealed evidence of ileocolic intussusception with edematous and possibly ischemic bowel (Figure). A right hemicolectomy was subsequently performed with primary ileo-mid-transverse colostomy. Examination of the patient’s resected tissue revealed Duke’s C adenocarcinoma of the right colon. The Duke’s classification of colon cancer places patients into one of four categories based on spread of cancer. This patient’s classification indicates that he had cancer spread out of the confines of his bowel wall and into adjacent lymph nodes without spread of beyond the confines of the lymph nodes. His post-operative recovery was otherwise uneventful.
DISCUSSION
Intussusception, defined as telescoping of a proximal part of small bowel along with its mesentery into an adjacent segment, leading to impaired peristalsis, obstruction, and possible vascular compromise, occurs mostly in the pediatric population. The classic triad of intermittent abdominal pain, bloody diarrhea, and a palpable tender mass has been described primarily in children.1 However, in adults, nausea, vomiting, gastrointestinal bleeding, changes in bowel habits and abdominal distension are the more common, nonspecific symptoms and signs of intussusception.2–6
In the adult population, intussusception is a rare condition, accounting for only 5% of all cases across all ages and 1–5% of small bowel obstruction.2 Primary or idiopathic intussusception accounts for about 8–20% of cases.2,4,7 Secondary intussusception, which is more commonly present in the adult population, is associated with a pathological condition involving a lead point. This causes one section of the bowel along with its mesentery to prolapse into adjacent bowel, leading to possible intestinal obstruction, vascular compromise, inflammatory changes, ischemia and even necrosis.3,8,9 Lead points could be intraluminal lesions, such as inflammatory lesions, Meckel’s diverticulum, polyps, or extraluminal lesions, such as adhesions, lipomas, lymphomas, and metastases. Malignancies are associated with 30% of small bowel intussusception, and 66% of large bowel intussusception.10 Intussusceptions are classified according to their locations: enteroenteric, colocolic, ileocolic, and ileocecal.3,11–13
As seen in both cases, the presenting symptoms and physical exam findings were not specific for intussusception. Abdominal pain and distention along with changes in bowel movements are symptoms associated with a long list of differential diagnoses, including gynecological causes in female patients. However, with a negative pelvic exam and transvaginal ultrasound, attention is then directed to non-gynecological causes. Radiologic evidence helps in narrowing down and focusing attention to a subset of possible etiologies, as demonstrated with CT of the abdomen and pelvis in case one, demonstrating ileocecal intussusception around a previous appendectomy scar.
Plain abdominal radiographs is typically the first diagnostic screening tool, demonstrating an bowel obstruction or perforation. However, radiographs are neither sensitive nor specific for intussusception.10,14–16 Ultrasonography is a useful clinical tool for the diagnosis of intussusception in both children and adults with high sensitivity and specificity: 98–100%, and 88%, respectively.17 Ultrasonography reveals a “target” or “doughnut” sign on the transverse view and the “pseudo-kidney” sign or “hay-fork” sign in the longitudinal view.18–21 CT is the most commonly used diagnostic modality with diagnostic accuracy of 58–100%.2,7,22–27 CT shows “target” or “sausage”-shaped lesions, as well as defines the location, the nature and the relationship of the lesion to surrounding tissues.11,22
Surgical resection of involved bowel segments serves as the treatment of choice in the adult population,4 since the lead point could be a malignancy, which could not only metastasize but also compromise blood flow, leading to necrosis of the involved bowel.
CONCLUSION
In the adult population, presenting complaints and physical exam are not sensitive or specific in making the diagnosis and identifying the lead point.28,29 Radiographic evidence is needed in the diagnosis of intussusception. Once suspected, surgical intervention is necessary to prevent further obstruction, vascular compromise, ischemia and necrosis of bowel. These cases are presented to increase awareness regarding intussusception in the adult population, where carcinoma and surgical scars can serve as lead points. Non-gynecological causes of right lower quadrant abdominal pain in female patients should also be considered, especially with a negative pelvic exam and transvaginal ultrasound.
Footnotes
Supervising Section Editor: Laleh Gharahbaghian, MD
Submission history: Submitted July 25, 2009; Revision Received November 29, 2009; Accepted January 11, 2010
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Shahram Lotfipour, MD, MPH, Department of Emergency Medicine, University of California, Irvine, 101 The City Dr., Orange, CA 92868
Email: SHL@uci.edu
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Harrington L, et al. Ultrasonographic and clinical predictors of intussusception. J Pediatr.1998;132(5):836–9. [PubMed]
2. Azar T, Berger DL. Adult intussusception. Ann Surg. 1997;226:134–8. [PMC free article] [PubMed]
3. Weilbaecher D, et al. Intussusception in adults. Review of 160 cases. Am J Surg. 1971;121:531–5.[PubMed]
4. Begos DG, Sandor A, Modlin IM. The diagnosis and management of adult intussusception. Am J Surg. 1997;173:88–94. [PubMed]
5. Nagorney DM, Sarr MG, McIlrath DC. Surgical management of intussusception in the adult. Ann Surg. 1981;193:230–6. [PMC free article] [PubMed]
6. Takeuchi K, et al. The diagnosis and treatment of adult intussusception. J Clin Gastroenterol.2003;36:18–21. [PubMed]
7. Erbil Y, et al. Ileocolic invagination in adult due to caecal carcinoma. Acta Chir Belg.1997;97:190–1. [PubMed]
8. Farrokh D, Saadaoui H, Hainaux B. Contribution of imaging in intestinal intussusception in the adult. Apropos of a case of ileocolic intussusception secondary to cecal lipoma. Ann Radiol (Paris)1996;39:213–6. [PubMed]
9. Gayer G, et al. Intussusception in adults: CT diagnosis. Clin Radiol. 1998;53:53–7. [PubMed]
10. Marinis A, et al. Intussusception of the bowel in adults: a review. World J Gastroenterol. 2009 Jan 28;15(4):407–11. [PMC free article] [PubMed]
11. Bar-Ziv J, Solomon A. Computed tomography in adult intussusception. Gastrointest Radiol.1991;16:264–6. [PubMed]
12. Tan KY, et al. Adult intussusception: experience in Singapore. ANZ J Surg. 2003;73:1044–7.[PubMed]
13. Warshauer DM, Lee JK. Adult intussusception detected at CT or MR imaging: clinical-imaging correlation. Radiology. 1999;212:853–0. [PubMed]
14. Haas EM, et al. Adult intussusception. Am J Surg. 2003;186:75–6. [PubMed]
15. Stubenbord WT, Thorbjarnarson B. Intussusception in adults. Ann Surg. 1970;172:306–10.[PMC free article] [PubMed]
16. Akcay MN, et al. Tumor-induced ileo-ileal invagination in adults. Am Surg. 1994;60:980–1.[PubMed]
17. Del-Pozo G, Albillos JC, Tejedor D, Calero R, Rasero M, Calle U de la, Lopez-Pacheco U. Intussusception in children: current concepts in diagnosis and enema reduction. Radiographics.1999;19:299–319. [PubMed]
18. Nagorney DM, Sarr MG, McIlrath DC. Surgical management of intussusception in the adult. Ann Surg. 1981;193:230–6. [PMC free article] [PubMed]
19. Cotlar AM, Cohn I., Jr Intussusception in adults. Am J Surg. 1961;101:114–20. [PubMed]
20. Eisen LK, Cunningham JD, Aufses AH., Jr Intussusception in adults: institutional review. J Am Coll Surg. 1999;188:390–5. [PubMed]
21. Cerro P, et al. Sonographic diagnosis of intussusceptions in adults. Abdom Imaging. 2000;25:45–7. [PubMed]
22. Smith DS, et al. The role of abdominal x-rays in the diagnosis and management of intussusception. Pediatr Emerg Care. 1992;8:325–7. [PubMed]
23. Yang ST, Tsai CH, Chen JA. Differential diagnosis between intussusception and gastroenteritis by plain film. Zhonghua Min Guo Xiao Er Ke Yi Xue Hue Za Zhi. 1995;36:170–5.
24. Fujii Y, Taniguchi N, Itoh K. Intussusception induced by villous tumor of the colon: sonographic findings. J Clin Ultrasound. 2002;30:48–51. [PubMed]
25. Boyle MJ, Arkell LJ, Williams JT. Ultrasonic diagnosis of adult intussusception. Am J Gastroenterol. 1993;88:617–8. [PubMed]
26. Weissberg DL, Scheible W, Leopold GR. Ultrasonographic appearance of adult intussusception.Radiology. 1977;124:791–2. [PubMed]
27. Byrne AT, et al. The imaging of intussusception. Clinical Radiology. 2005;60:39–46. [PubMed]
28. Martin-Lorenzo JG, et al. Intestinal invagination in adults: preoperative diagnosis and management. Int J Colorectal Dis. 2004;19:68–72. [PubMed]
29. Khan MN, Agrawal A, Strauss P. Ileocolic Intussusception – A rare cause of acute intestinal obstruction in adults; Case report and literature review. World J Emerg Surg. 2008;3:26.[PMC free article] [PubMed]