
{kind=link}
| Author | Affiliation |
|---|---|
| Kieron Barkataki, DO | Kern Medical, Department of Emergency Medicine, Bakersfield, California |
| Nathan Wang, MD | Kern Medical, Department of Emergency Medicine, Bakersfield, California |
| Daniel Quesada, MD | Kern Medical, Department of Emergency Medicine, Bakersfield, California; LAC+USC Medical Center, Department of Emergency Medicine, Los Angeles, California |
| Rachell O’Donnell, MD | Kern Medical, Department of Emergency Medicine, Bakersfield, California |
| James W. Rosbrugh, MD | Kern Medical, Department of Emergency Medicine, Bakersfield, California |
| Phillip Aguìñiga-Navarrete, RA | Kern Medical, Department of Emergency Medicine, Bakersfield, California |
CASE PRESENTATION
A 39-year-old male with no past history presented with three months of left inguinal pain and a left groin lump that became progressively larger and more painful. He was seen at another hospital over one month prior where they were unable to manually reduce the lump. He could not recall the computed tomography (CT) findings, and no surgery was performed. Since then, he has experienced persistent left inguinal pain and nausea. He denied fever, vomiting, dysuria, hematuria, penile discharge, testicular pain, or history of sexually transmitted diseases.
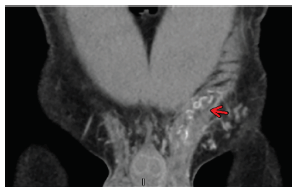
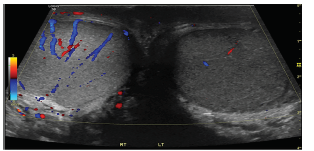
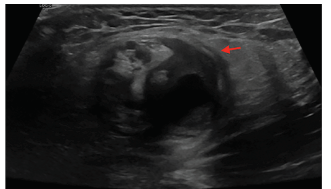
Physical exam revealed a firm, tender, and non-reducible mass in the left inguinal canal and along the spermatic cord. Remainder of examination was normal. Complete blood count, basic metabolic panel, lactate, urinalysis and urine culture were normal. CT of the abdomen and pelvis was suggestive of pampiniform plexus thrombosis (Image 1). Formal ultrasound images revealed diminished Doppler vascular flow (Image 2) within the left testicle and prominent, heterogeneous vascular structures seen in the left inguinal canal (Image 3) that correlated with the CT, indicating pampiniform plexus thrombosis as well.
DISCUSSION
Pampiniform plexus thrombosis is a rare cause of inguinal pain, which is often misdiagnosed as hernia or orchitis. Accurate diagnosis can prevent unnecessary treatment including surgical intervention. There are limited references in the literature to this condition, and there are no evidence-based approaches to management. The majority of reported cases involved the left venous plexus, and most were diagnosed intra-operatively for pre-operative diagnoses of incarcerated inguinal hernia or orchitis.1 A work-up for hypercoagulability is recommended.2 Management has ranged from conservative treatment with nonsteroidal anti-inflammatory drugs to surgical excision of the thrombosed vessels.3
CPC-EM Capsule
What do we already know about this clinical entity?
Pampinifom plexus thrombosis is a rare cause of inguinal pain. There is little consensus about the appropriate treatment at this time.
What is the major impact of the image(s)?
This disease process is often mistaken for incarcerated inguinal hernia. Multiple cases were not accurately diagnosed until the patient was on the operating table.
How might this improve emergency medicine practice?
This case reminds physicians of rare clinical entities and may help avoid unnecessary surgery.
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
Address for Correspondence: Kieron Barkataki, DO, Kern Medical, Department of Emergency Medicine,1700 Mount Vernon Avenue, Bakersfield, CA 93306. Email: kieron20@gmail.com. 3:170 – 171
Submission history: Revision received October 10, 2018; Submitted January 4, 2019; Accepted January 12, 2019
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Kamel K, Gassen S, Mohamed M, et al. Bilateral spontaneous thrombosis of the pampiniform plexus; a rare etiology of acute scrotal pain: a case report and review of literature. Afr J Urol. 2018;24(1):14-8.
2. Tanner R, Twomey M, Maher MM, et al. A rare cause of testicular pain: thrombosis of the pampiniform plexus. Ir Med J. 2016;109(1):347-8.
3. Ouanes Y, Sellami A, Chaker K, et al. Thrombosis of the pampiniform plexus: About a case report. Urol Case Rep. 2018;20:28-9.