Intro: Our objective was to compare the ability of SI, individual vital signs, and the systemic inflammatory response syndrome (SIRS) criteria to predict the primary outcome of hyperlactatemia (serum lactate ≥ 4.0 mmol/L) as a surrogate for disease severity, and the secondary outcome of 28-day mortality.
Conclusion: In this cohort, SI ≥ 0.7 performed as well as SIRS in NPV and was the most sensitive screening test for hyperlactatemia and 28-day mortality. SI ≥ 1.0 was the most specific predictor of both outcomes.
Primary meningococcal arthritis (PMA) is a rare infectious disease that occurs in as little as 1% of meningococcal infections. PMA is arthritis without meningitis, fever, rash, and hemodynamic instability. It is usually preceded by an upper respiratory infection in 50–55% of presentations, and patients may appear nontoxic, afebrile, and polyarthralgic. Despite definition they may have a rash.
A 15-year-old female presented to the emergency department (ED) with a 1-week history of fevers, vomiting, back pain and dysuria. Her primary care physician started her on cefdinir for a urinary tract infection. On initial evaluation she was febrile, tachycardic, and had an exam notable for tenderness of both the left costovertebral angle and suprapubic region.
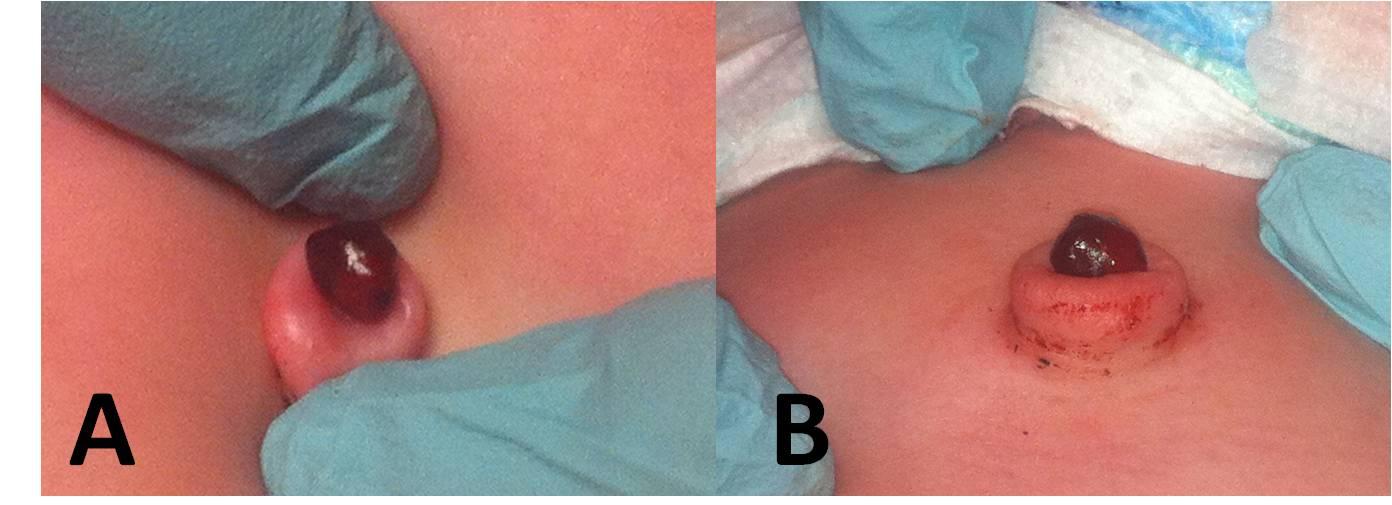
A 41-day-old girl presented to the emergency department with a new dark red mass protruding from the umbilicus noted 3.5 hours prior to presentation. The patient’s mother reported the umbilical stump fell off at 4 days of life, but the patient continued to have intermittent clear green drainage from a small mass at the base of the umbilicus. The patient was born full-term with an otherwise unremarkable medical history.
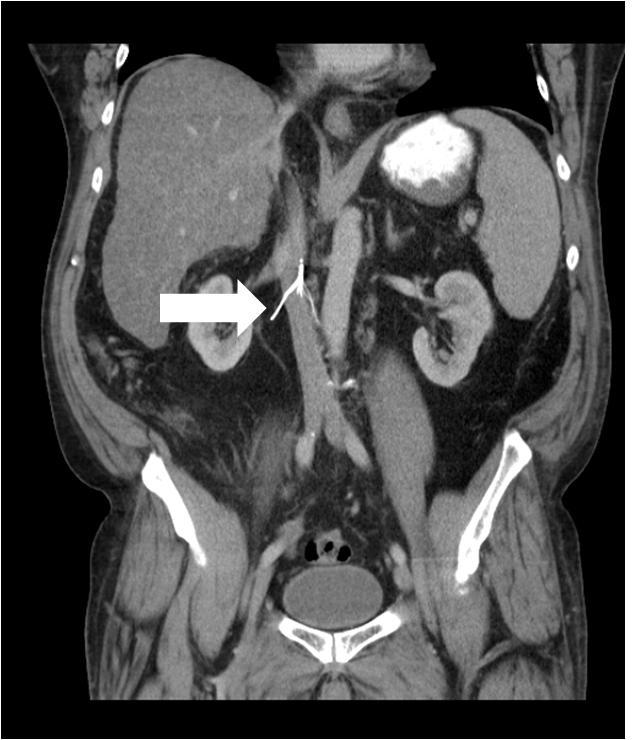
A 46-year-old male with diabetes, hypertension, and a history of pulmonary embolism (status post placement of a retrievable Celect inferior vena cava [IVC] filter) presented to the emergency department with progressively worsening abdominal pain for 1 month.
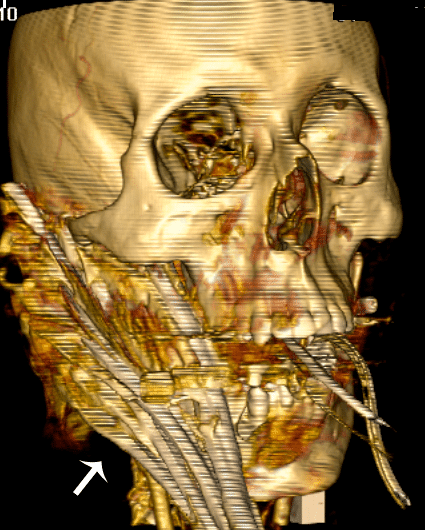
Penetrating injuries to the face or neck can cause difficult airway issues. There is a relative dearth of literature to define the best approach to these patients. Impalement injuries are uncommon, and survivable injuries are most commonly confined to the abdomen or thorax. We report the case of a patient with an obviously difficult airway due to a facial impalement (Jael’s Syndrome) injured at a local construction site.
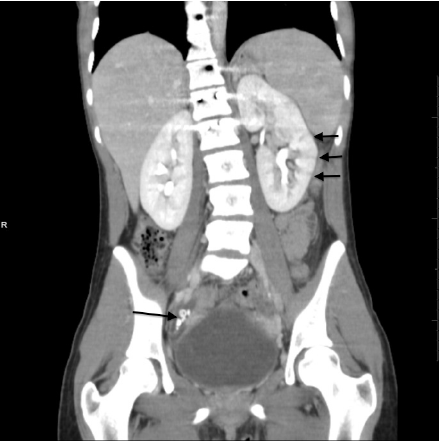
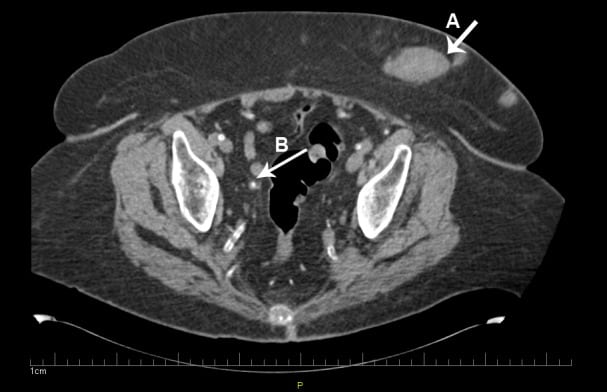
An 81-year-old female with history of end stage renal disease on hemodialysis presented with worsening of abdominal pain of 2 days’ duration. The pain started as a dull ache over the lower abdomen 2 months earlier, diffuse but especially prominent over the lower quadrant, and was unrelieved by analgesic medications.
A 49-year-old man was brought to the emergency department by ambulance after he sustained a stab wound to the chest. He was alert but diaphoretic, with an initial systolic blood pressure of 90 by palpation and a heart rate of 110. A 1 cm laceration was noted at the left lower sternal border. Lung sounds were clear bilaterally, and heart sounds were muted.
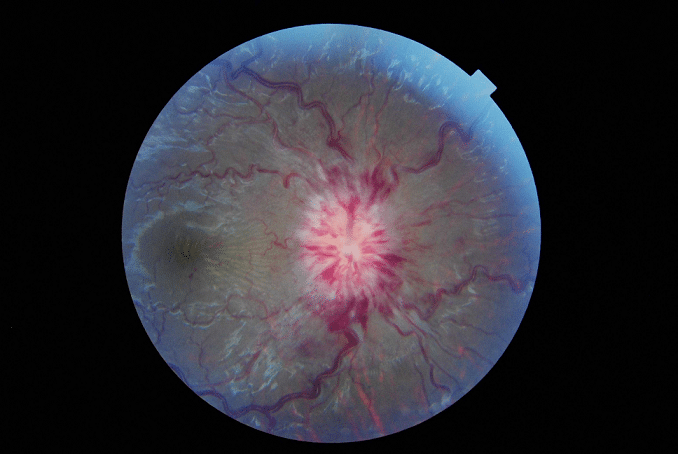
Idiopathic intracranial hypertension (IIH), also known as pseudotumor cerebri, defined as elevated intracranial pressure with no evident cause found on extensive evaluation.
A 40-year-old man with Hepatitis C and a history of cocaine abuse presented with multiple stages of painful rashes on his extremities and ears. On examination, the patient had several areas of purpuric macules and retiform purpura to his legs and ears, as well as large ulcerations with erythematous borders on bilateral lower extremities
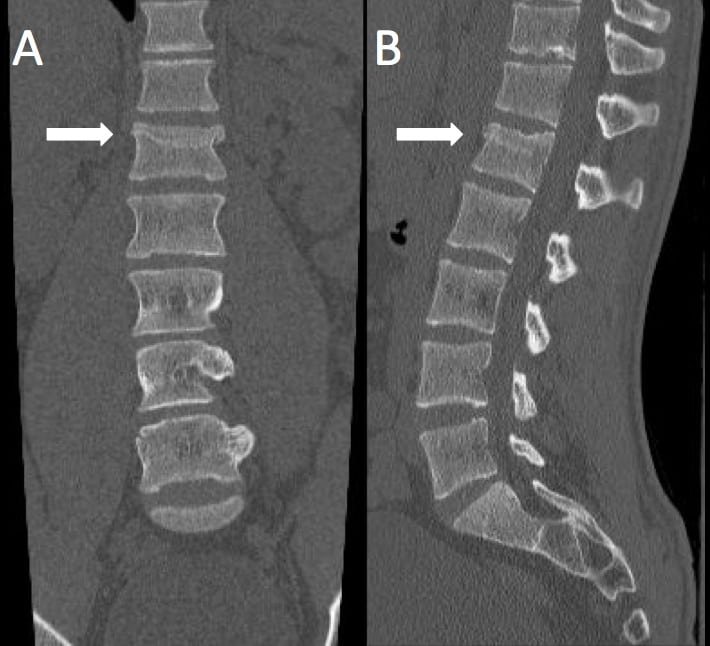
Since the first description of the Chance fracture in 1948, there have been few case reports of unique mechanisms causing this classical flexion-extension injury to the spine in motor vehicle accidents, sports injury, and falls. To our knowledge, this injury has not been reported from a fall with the mechanistic forces acting laterally on the spine and with spinal support in place. We present a 21-year-old male who slid down a flight of stairs onto his side wearing a heavy mountaineering style backpack, subsequently sustaining a Chance fracture of his first lumbar vertebrae.
A 76-year-old man with a history of ankylosing spondylitis presented to the emergency department complaining of neck pain. He stated the pain began when he slipped to the ground from a seated position in his bedroom.
Intro: About 10,000 escalator-related injuries per year result in emergency department treatment in the United States. Since the 1990s, a steady increase has been reported, but few statistics on escalator-related injuries have been published worldwide.
Conclusion: Escalator accidents can result in severe trauma. Significant gender differences in escalator accidents have been observed. Alcohol intoxication and age are significant risk factors in escalator-related accidents and might be possible targets for preventive measures.
Introduction: We tested the effect of a brief disposition process intervention on residents’ time to disposition and emergency department (ED) length of stay (LOS) in high acuity ED patients.
Conclusion: Prompting residents to enter administrative disposition orders in high acuity patients is associated with significant reduction in both time to disposition and ED LOS.
Introduction: The purpose of this study was to evaluate a multi-media education intervention as a method for informing independently living elders about ED care. The program delivered messages categorically as, the number of tests, providers, decisions and disposition decision making.
Conclusion: A short video with graphic side-bar information is an effective educational strategy to improve elder understanding of expectations during a hypothetical ED encounter following calling 911.
A 61-year-old male with a 1-year history of bilateral lower extremity swelling and a chronic cough was referred to the emergency department (ED) for an abnormal echocardiogram. The patient also reported experiencing intermittent episodes of chest pressure. He stated that he was referred from his doctor after he received a cardiac echocardiography examination that showed possible mitral valve vegetations. On review of systems, he also admitted to intermittent chest palpitations.
This case study describes a patient who suffered blunt force trauma to the scrotum. Use of bedside emergency ultrasound facilitated early diagnosis of a ruptured testicle and allowed for prompt urological consultation and timely surgical repair. The utility of bedside emergency ultrasound in the evaluation of testicular trauma, as well as the outcome of our case, is discussed here.
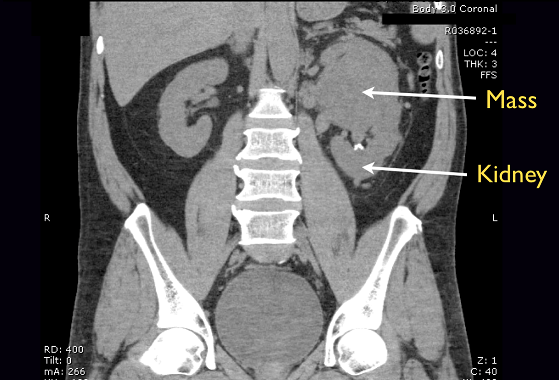
Flank pain with hematuria is a common chief complaint in the emergency department (ED). Patients are often diagnosed with renal calculi or pyelonephritis and discharged with analgesics or antibiotics and follow-up. This case study describes a patient who presented to the ED with a 1 week history of flank pain and hematuria and was subsequently found to have a large renal mass on bedside ultrasound.
A 32 year-old female presented to the emergency department (ED) with complaints of mild vaginal spotting accompanied by uterine cramping. She was referred to the ED for an “abnormal pregnancy.” She was a G1P0 and her last menstrual period was 7 weeks 5 days prior. Physical examination demonstrated a well appearing female with normal vital signs.
A 36-year-old male presented to the emergency department (ED) complaining of “lumps in my penis.” The patient described 2 firm, raised areas on the dorsum of his penis that had been present 1 week. He had no pain at rest or with palpation but mild discomfort with erection. He denied trauma, dysuria, hematuria, or discharge. He had no prior medical history and took no medications.
Introduction: There is limited literature on the effect of computerized physician order entry (CPOE) on mortality. The objective of our study was to determine if there was a change in mortality among critically ill patients presenting to the emergency department (ED) after the implementation of a CPOE system.
Conclusion: The implementation of CPOE was not associated with a change in mortality of critically ill ED patients, but was associated with a decrease in proportion of patients discharged to home after hospitalization.
Hepatic abscess is an uncommon occurrence in North America, but can be a diagnostic challenge for emergency department physicians. The clinical signs and symptoms may vary, leading to delays in diagnosis and higher morbidity. We present a case of a 35-year old male with a hepatic abscess initially misdiagnosed as pneumonia. On subsequent return to the ED for back pain complaints, a bedside ultrasound led to the appropriate diagnosis. This case report and discussion will attempt to review the literature on the etiology, diagnosis and treatment of hepatic abscess for the emergency physician.
Introduction: The adoption of electronic medical records (EMRs) in emergency departments (EDs) has changed the way that healthcare information is collected, charted, and stored. A challenge for researchers is to determine how EMRs may be leveraged to facilitate study data collection efforts. Our objective is to describe the use of a unique data collection system leveraging EMR technology and to compare data entry error rates to traditional paper data collection.
Conclusion: DP data collection is a feasible means of data collection. DP data forms maintain all study data within the secure EMR environment, obviating the need to maintain and collect paper data forms.
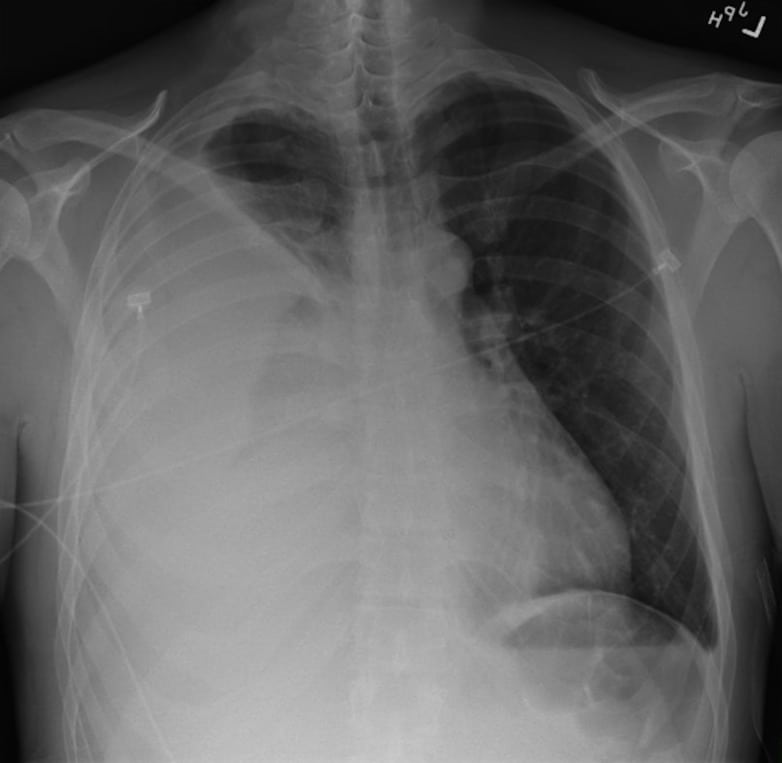
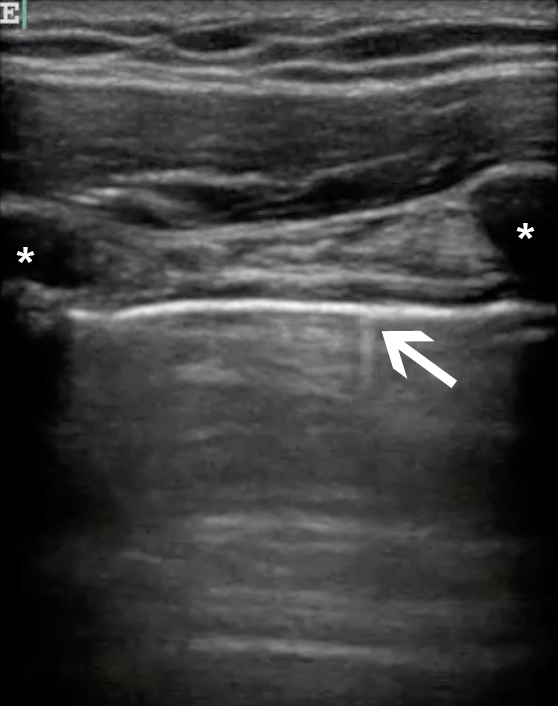
Intro: Prior studies have reported conflicting results regarding the utility of ultrasound in the diagnosis of traumatic pneumothorax (PTX) because they have used sonologists with extensive experience. This study evaluates the characteristics of ultrasound for PTX for a large cohort of trauma and emergency physicians.
Conclusion: In a large heterogenous group of clinicians who typically care for trauma patients, the sonographic evaluation for pneumothorax was as accurate as supine chest radiography. Thoracic ultrasound may be helpful in the initial evaluation of patients with truncal trauma.
Introduction: In a 2001 quality improvement (QI) study, we demonstrated improvement in paramedic knowledge, perceptions, and management of pain. This follow-up study examines the impact of this QI program, repeated educational intervention (EI), and effectiveness of a new pain management standard operating procedure.
Conclusion: In this follow up study, paramedics’ baseline knowledge, perceptions, and management of pain have all improved from 6 years ago.
Introduction: The boarding of admitted patients in the emergency department (ED) is a major cause of crowding and access block. One solution is boarding admitted patients in inpatient ward (W) hallways.
Conclusion: Inpatient nurses and those who have never worked in the ED are more opposed to inpatient boarding than ED nurses and nurses who have worked previously in the ED. Primary nursing concerns about boarding are lack of monitoring and privacy in hallway beds. Nurses admitted as patients seemed to prefer not being boarded where they work.
{kind=link}