
{kind=link}
| Author | Affiliation |
| Jeffrey L. Wiswell, MD | University of California Davis, Sacramento, California |
| Benjamin J. Sandefur, MD | Mayo Clinic, Rochester, Minnesota |
ABSTRACT
A 33 year-old female presented to the emergency department (ED) with of two weeks of diffuse abdominal pain, right flank pain, and a slowly enlarging right inguinal mass. She had no associated fever, chills, nausea, vomiting, or diarrhea. She was evaluated by her primary care physician, and an inguinal ultrasound was obtained prior to referral to the ED. On arrival in the ED, her vital signs were unremarkable, and she was afebrile. On exam, there was no abdominal tenderness, and a 2cm x 2cm non-reducible, mildly tender right inguinal mass was noted. A bedside ultrasound (Figures 1 and 2) was performed in the ED.
DIAGNOSIS
Amyand’s Hernia: Named for Claudius Amyand, sergeant-surgeon to King George II of England, Amyand’s Hernia is an appendix within an inguinal hernia.1 In the index case, he is credited with performing the first successful appendectomy in 1735, on an eleven year-old boy with this condition.2 Although relatively rare, (0.13% of cases of acute appendicitis occur in external hernias),3 it is important to consider this diagnosis in the setting of abdominal pain with an associated inguinal mass. In addition, Amyand’s Hernia may mimic an acute scrotum in cases of appendiceal rupture after a period of incarceration.2 In this particular case, bedside ultrasound demonstrated a non-compressible 7.4 mm tubular structure within a hernia sack (Figures 1 and 2), representing the appendix. The patient was taken to the operating room for open appendectomy and femoral hernia repair. She was discharged without any complications the following day.

Figure 1. Long axis view ultrasound of an inguinal mass.
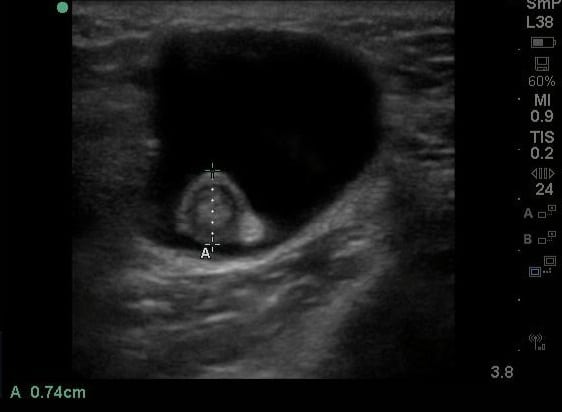
Figure 2. Short axis view ultrasound of an inguinal mass.
Footnotes
Supervising Section Editor: Rick McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Jeffrey L. Wiswell, MD, Department of Emergency Medicne, 200 First Street SW, Rochester, MN 55905. Email: wiswell.jeffrey@mayo.edu.
Submission history: Submitted March 17, 2014;Revision received May 20, 2014; Accepted August 20, 2014
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
- Malayeri A, Siegelman S. Amyand’s Hernia–Images in clinical medicine. N Engl J Med. 2011;364(22):2147.
- Doyle G, McCowan C. Amyand hernia: a case of an unusual inguinal herniace. Am J Emerg Med. 2008;26(5):637.e5-637.e6.
- Ryan WJ. Hernia of the vermiform appendix. Ann Surg. 1937;106:135-139.
{kind=link}