Healthcare systems often expose patients to significant, preventable harm causing an estimated 44,000 to 98,000 deaths or more annually. This has propelled patient safety to the forefront, with reporting systems allowing for the review of local events to determine their root causes. As residents engage in a substantial amount of patient care in academic emergency departments, it is critical to use these safety event reports for resident-focused interventions and educational initiatives. This study analyzes reports from the Virginia Commonwealth University Health System to understand how the reports are categorized and how it relates to opportunities for resident education.
Delays in identification and treatment of acute stroke contribute to significant morbidity and mortality. Multiple clinical factors have been associated with delays in acute stroke care. We aimed to determine the relationship between emergency department (ED) crowding and the delivery of timely emergency stroke care.
Droperidol carries a boxed warning from the United States Food and Drug Administration for QT prolongation and torsades des pointes (TdP). After a six-year hiatus, droperidol again became widely available in the US in early 2019. With its return, clinicians must again make decisions regarding the boxed warning. Thus, the objective of this study was to report the incidence of QT prolongation or TdP in patients receiving droperidol in the ED.
Crowding in the emergency department (ED) impacts a number of important quality and safety metrics. We studied ED crowding measures associated with adverse events (AE) resulting from central venous catheters (CVC) inserted in the ED, as well as the relationship between crowding and the frequency of CVC insertions in an ED cohort admitted to the intensive care unit (ICU).
Procedural sedation and analgesia (PSA) provides safe and effective relief for pain, anxiety and discomfort during procedures performed in the emergency department (ED). Our objective was to identify hospital-level factors associated with routine PSA capnography use in the ED.
Many patients with atrial fibrillation or atrial flutter (AF/FL) who are high risk for ischemic stroke are not receiving evidence-based thromboprophylaxis. We examined anticoagulant prescribing within 30 days of receiving dysrhythmia care for non-valvular AF/FL in the emergency department (ED).
In this issue of WestJEM, Smith and colleagues present a prospective observational evaluation of anticoagulation prescribing practices in non-valvular AF. Patients presenting to one of seven Northern California EDs with AF at high risk for stroke were eligible unless admitted, not part of Kaiser Permanente of Northern California (KPNC), or already prescribed anticoagulation
This is an ambispective, observational, cohort study to determine variance in failure rates between femoral and radial arterial lines. This study took place from 2012 to 2016 and included all arterial lines placed in adult patients at a single institution.
Miscommunication during inter-unit handoffs between emergency and internal medicine physicians may jeopardize patient safety. Our goal was to evaluate the impact of a structured communication strategy on the quality of admission handoffs.
Computerized decision support decreases the number of computed tomography pulmonary angiograms (CTPA) for pulmonary embolism (PE) ordered in emergency departments, but it is not always well accepted by emergency physicians. We studied a department-endorsed, evidence-based clinical protocol that included the PE rule-out criteria (PERC) rule, multi-modal education using principles of knowledge translation (KT), and clinical decision support embedded in our order entry system, to decrease the number of unnecessary CTPA ordered.
Many patients meeting criteria for severe sepsis are not given a sepsis-related diagnosis by emergency physicians (EP). This study 1) compares emergency department (ED) interventions and in-hospital outcomes among patients with severe sepsis, based on the presence or absence of sepsis-related diagnosis, and 2) assesses how adverse outcomes relate to three-hour sepsis bundle completion among patients fulfilling severe sepsis criteria but not given a sepsis-related diagnosis.
There are established and validated clinical decision tools for cervical spine clearance. Almost all the rules include spinal tenderness on exam as an indication for imaging. Our goal was to apply GLASS, a previously derived clinical decision tool for cervical spine clearance, to thoracolumbar injuries. GLass intact Assures Safe Spine (GLASS) is a simple, objective method to evaluate those patients involved in motor vehicle collisions and determine which are at low risk for thoracolumbar injuries.
Pneumonia impacts over four million people annually and is the leading cause of infectious disease-related hospitalization and mortality in the United States. Appropriate empiric antimicrobial therapy decreases hospital length of stay and improves mortality. The objective of our study was to test the hypothesis that the presence of an emergency medicine (EM) clinical pharmacist improves the timing and appropriateness of empiric antimicrobial therapy for community-acquired pneumonia (CAP) and healthcare-associated pneumonia (HCAP).
However, little is known about the field availability or accuracy of information of chronic health conditions or chronic medication treatments in emergent circumstances, especially when the patient cannot serve as an information resource. We evaluated the prehospital availability and accuracy of specific chronic health conditions and medication treatments among out-of-hospital cardiac arrest (OHCA) patients.
Less than half of patients with a chest pain history indicative of acute coronary syndrome have a diagnostic electrocardiogram (ECG) on initial presentation to the emergency department. The physician must dissect the ECG for elusive, but perilous, characteristics that are often missed by machine analysis.
In June 2016, the American College of Emergency Physicians (ACEP) Emergency Quality Network began its Reduce Avoidable Imaging Initiative, designed to “reduce testing and imaging with low risk patients through the implementation of Choosing Wisely recommendations.”
Author Affiliation Nick T. Sawyer, MD, MBA University of California, Davis, Department of Emergency Medicine, Sacramento, California; California American College of Emergency Physicians Board of Directors John D. Coburn, MD The Permanente Medical Group, South Sacramento Kaiser, Department of Emergency Medicine, Sacramento, California; California American College of Emergency Physicians Board of Directors Under-triage is a […]
Emergency physicians (EP) frequently are exposed to promotion for drugs and devices through professional organizations and meetings, journals, and direct-to-consumer pharmaceutical advertising (DTCPA). To provide optimum patient care through evidence-based medicine, it is critical to be aware of the processes that regulate these drugs.
The value of using patient- and physician-identified quality assurance (QA) issues in emergency medicine remains poorly characterized as a marker for emergency department (ED) QA. The objective of this study was to determine whether evaluation of patient and physician concerns is useful for identifying medical errors resulting in either an adverse event or a near-miss event.
Author Affiliation James A. Heilman, MD Oregon Health & Science University, Department of Emergency Medicine, Portland, Oregon Moira Flanigan, BS Oregon Health & Science University, Department of Emergency Medicine, Portland, Oregon Anna Nelson, MD, PhD Oregon Health & Science University, Department of Emergency Medicine, Portland, Oregon Tom Johnson, MD, PhD Oregon Health & Science University, […]
Volume 16, Issue 7, December 2015.
Michael J. Ward, MD, MBA, et al.
Introduction: With the majority of U.S. hospitals not having primary percutaneous coronary intervention
(pPCI) capabilities, the time spent at transferring emergency departments (EDs) is predictive of clinical
outcomes for patients with ST-elevation myocardial infarction (STEMI). Compounding the challenges
of delivering timely emergency care are the known delays caused by ED crowding. However, the
association of ED crowding with timeliness for patients with STEMI is unknown. We sought to examine
the relationship between ED crowding and time spent at transferring EDs for patients with STEMI.
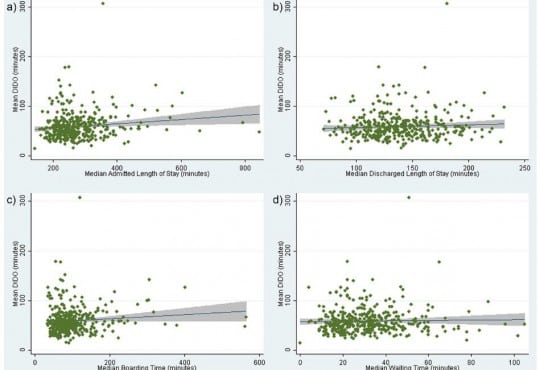
Methods: We analyzed the Centers for Medicare and Medicaid Services (CMS) quality data. The
outcome was time spent at a transferring ED (i.e., door-in-door-out [DIDO]), was CMS measure OP-3b for
hospitals with ≥10 acute myocardial infarction (AMI) cases requiring transfer (i.e., STEMI) annually: Time
to Transfer an AMI Patient for Acute Coronary Intervention. We used four CMS ED timeliness measures
as surrogate measures of ED crowding: admitted length of stay (LOS), discharged LOS, boarding time,
and waiting time. We analyzed bivariate associations between DIDO and ED timeliness measures. We
used a linear multivariable regression to evaluate the contribution of hospital characteristics (academic,
trauma, rural, ED volume) to DIDO.
Results: Data were available for 405 out of 4,129 hospitals for the CMS DIDO measure. These facilities
were primarily non-academic (99.0%), non-trauma centers (65.4%), and in urban locations (68.5%). Median
DIDO was 54.0 minutes (IQR 42.0,68.0). Increased DIDO time was associated with longer admitted
LOS and boarding times. After adjusting for hospital characteristics, a one-minute increase in ED LOS at
transferring facilities was associated with DIDO (coefficient, 0.084 [95% CI [0.049,0.119]]; p<0.001). This
translates into a five-minute increase in DIDO for every one-hour increase in ED LOS for admitted patients.
Conclusion: Among patients with STEMI presenting to U.S. EDs, we found that ED crowding has a
small but operationally insignificant effect on time spent at the transferring ED.
Volume 16, Issue 7, December 2015.
Nnaemeka G. Okafor, MD, MS, et al.
Introduction: Medical errors are frequently under-reported, yet their appropriate analysis, coupled
with remediation, is essential for continuous quality improvement. The emergency department (ED) is
recognized as a complex and chaotic environment prone to errors. In this paper, we describe the design
and implementation of a web-based ED-specific incident reporting system using an iterative process.
Methods: A web-based, password-protected tool was developed by members of a quality assurance
committee for ED providers to report incidents that they believe could impact patient safety.
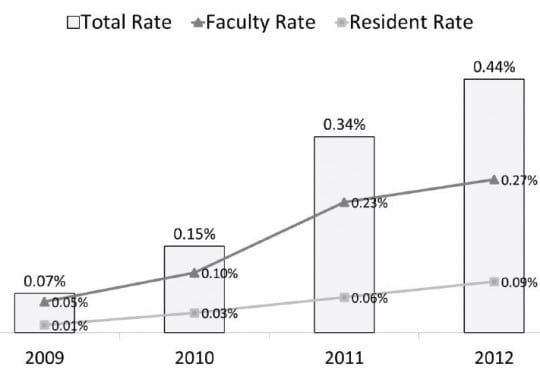
Results: The utilization of this system in one residency program with two academic sites resulted
in an increase from 81 reported incidents in 2009, the first year of use, to 561 reported incidents
in 2012. This is an increase in rate of reported events from 0.07% of all ED visits to 0.44% of all
ED visits. In 2012, faculty reported 60% of all incidents, while residents and midlevel providers
reported 24% and 16% respectively. The most commonly reported incidents were delays in care and
management concerns.
Conclusion: Error reporting frequency can be dramatically improved by using a web-based, user friendly,
voluntary, and non-punitive reporting system.
Volume 16, Issue 5, September 2015.
Daniel Cabrera, MD, et al.
Introduction: Current cognitive sciences describe decision-making using the dual-process theory,
where a System 1 is intuitive and a System 2 decision is hypothetico-deductive. We aim to compare
the performance of these systems in determining patient acuity, disposition and diagnosis.
Methods: Prospective observational study of emergency physicians assessing patients in the
emergency department of an academic center. Physicians were provided the patient’s chief
complaint and vital signs and allowed to observe the patient briefly. They were then asked to predict
acuity, final disposition (home, intensive care unit (ICU), non-ICU bed) and diagnosis. A patient was
classified as sick by the investigators using previously published objective criteria.
Results: We obtained 662 observations from 289 patients. For acuity, the observers had a sensitivity
of 73.9% (95% CI [67.7-79.5%]), specificity 83.3% (95% CI [79.5-86.7%]), positive predictive value
70.3% (95% CI [64.1-75.9%]) and negative predictive value 85.7% (95% CI [82.0-88.9%]). For final
disposition, the observers made a correct prediction in 80.8% (95% CI [76.1-85.0%]) of the cases.
For ICU admission, emergency physicians had a sensitivity of 33.9% (95% CI [22.1-47.4%]) and a
specificity of 96.9% (95% CI [94.0-98.7%]). The correct diagnosis was made 54% of the time with
the limited data available.
Conclusion: System 1 decision-making based on limited information had a sensitivity close to 80%
for acuity and disposition prediction, but the performance was lower for predicting ICU admission
and diagnosis. System 1 decision-making appears insufficient for final decisions in these domains
but likely provides a cognitive framework for System 2 decision-making.
{kind=link}