Many factors contribute to the survival of out-of-hospital cardiac arrest (OHCA). Consequently, we sought to develop a model describing the likelihood of return of spontaneous circulation (ROSC) as a function of paramedic cumulative OHCA experience.
Air-medical critical care providers are frequently called upon to provide advanced airway management to our critically ill patients. The majority of these cases involve the transport of patients who have been intubated with standard endotracheal tubes (ETT).
The number of community paramedic (CP) programs has expanded to mitigate the impact of increased patient usage on emergency services. However, it has not been determined to what extent emergency medical services (EMS) professionals would be willing to participate in this model of care. With this project, we sought to evaluate the perceptions of EMS professionals toward the concept of a CP program.
Emergency medical services (EMS) agencies transport a significant majority of patients with low acuity and non-emergent conditions to local emergency departments (ED), affecting the entire emergency care system’s capacity and performance.
Endotracheal intubation is a common intervention in critical care patients undergoing helicopter emergency medical services (HEMS) transportation. Measurement of endotracheal tube (ETT) cuff pressures is not common practice in patients referred to our service. Animal studies have demonstrated an association between the pressure of the ETT cuff on the tracheal mucosa and decreased blood flow leading to mucosal ischemia and scarring. Cuff pressures greater than 30 cmH2O impede mucosal capillary blood flow.
A Comparison of Chest Compression Quality Delivered During On-Scene and Ground Transport Cardiopulmonary Resuscitation
Christopher S. Russi, DO et al.
The 2010 American Heart Association (AHA)/International Liaison Committee on Resuscitation (ILCOR) Cardiopulmonary Resuscitation (CPR) Guidelines call for a minimum chest compression rate of 100 to 120 compressions per minute and a minimum chest compression depth of 1.5 to 2 inches (3.75–5 cm).1 Two clinical studies have reported the quality of chest compressions delivered before emergency medical services (EMS) transport and the quality of those delivered during transport.2,3 Further evidence has suggested that visual, automated CPR feedback improves CPR quality.
Determinants of Success and Failure in Prehospital Endotracheal Intubation
Lucas A. Myers, BAH et al.
Endotracheal intubation (ETI) performance by emergency medical services (EMS) personnel remains a heavily examined and debated issue for medical directors and prehospital care providers. Research on success rates in adults has demonstrated ranges from 77.2% to 98.5%.1-4 Unfortunately, opportunities for clinical intubation are infrequent.5 EMS educational programs have highlighted the need for greater frequency of ETI performance through clinical opportunities such as the operating suite.6 Given the relatively few opportunities for practicing the procedure in some EMS systems, detailed patient selection and guideline criteria aimed at limiting difficult intubation attempts may increase the relative proportion of success.
Prehospital Lactate Measurement by Emergency Medical Services in Patients Meeting Sepsis Criteria
Lori L. Boland, MPH et al.
We aimed to pilot test the delivery of sepsis education to emergency medical services (EMS) providers and the feasibility of equipping them with temporal artery thermometers (TATs) and handheld lactate meters to aid in the prehospital recognition of sepsis.
Geospatial Analysis of Pediatric EMS Run Density and Endotracheal Intubation
Matthew Hansen, MD, MCR et al.
The association between geographic factors, including transport distance, and pediatric emergency medical services (EMS) run clustering on out-of-hospital pediatric endotracheal intubation is unclear. The objective of this study was to determine if endotracheal intubation procedures are more likely to occur at greater distances from the hospital and near clusters of pediatric calls.
The Medical Duty Officer: An Attempt to Mitigate the Ambulance At-Hospital Interval
Megan H. Halliday, MSIII, BS et al.
A lack of coordination between emergency medical services (EMS), emergency departments (ED) and systemwide management has contributed to extended ambulance at-hospital times at local EDs. In an effort to improve communication within the local EMS system, the Baltimore City Fire Department (BCFD) placed a medical duty officer (MDO) in the fire communications bureau. It was hypothesized that any real-time intervention suggested by the MDO would be manifested in a decrease in the EMS at-hospital time.
Volume 17, Issue 4, July 2016
Michael M. Neeki, DO, MS, et al.
Mobilization of trauma resources has the potential to cause ripple effects throughout hospital operations. One major factor affecting efficient utilization of trauma resources is a discrepancy between the prehospital estimated time of arrival (ETA) as communicated by emergency medical services (EMS) personnel and their actual time of arrival (TOA). The current study aimed to assess the accuracy of the perceived prehospital estimated arrival time by EMS personnel in comparison to their actual arrival time at a Level II trauma center in San Bernardino County, California.
Volume 17, Issue 4, July 2016
Michael Smyth, MSc, et al.
Sepsis is a common and potentially life-threatening response to an infection. There are an estimated 150,000 cases of severe sepsis resulting in more than 44,000 deaths each year in the United Kingdom (UK). It has been reported that over 70% of sepsis cases stem from the community with one study suggesting two-thirds of severe sepsis cases are initially seen in the emergency department (ED).2 Approximately half of all ED sepsis patients will arrive via emergency medical services (EMS). Sepsis patients transported to the ED by EMS are likely to be sicker than those arriving by other means, with up to 80% of severe sepsis patients admitted to intensive care from the ED having been transported by EMS.
Volume 16, Issue 7, December 2015.
P. Brian Savino, MD
Introduction: In the United States, emergency medical services (EMS) protocols vary widely across
jurisdictions. We sought to develop evidence-based recommendations for the prehospital evaluation
and treatment of chest pain of suspected cardiac origin and to compare these recommendations
against the current protocols used by the 33 EMS agencies in the state of California.
Methods: We performed a literature review of the current evidence in the prehospital treatment
of chest pain and augmented this review with guidelines from various national and international
societies to create our evidence-based recommendations. We then compared the chest pain
protocols of each of the 33 EMS agencies for consistency with these recommendations. The
specific protocol components that we analyzed were use of supplemental oxygen, aspirin, nitrates,
opiates, 12-lead electrocardiogram (ECG), ST segment elevation myocardial infarction (STEMI)
regionalization systems, prehospital fibrinolysis and β-blockers.
Results: The protocols varied widely in terms of medication and dosing choices, as well as listed
contraindications to treatments. Every agency uses oxygen with 54% recommending titrated
dosing. All agencies use aspirin (64% recommending 325mg, 24% recommending 162mg and 15%
recommending either), as well as nitroglycerin and opiates (58% choosing morphine). Prehospital 12-
Lead ECGs are used in 97% of agencies, and all but one agency has some form of regionalized care
for their STEMI patients. No agency is currently employing prehospital fibrinolysis or β-blocker use.
Conclusion: Protocols for chest pain of suspected cardiac origin vary widely across California. The
evidence-based recommendations that we present for the prehospital diagnosis and treatment of this
condition may be useful for EMS medical directors tasked with creating and revising these protocols.
Volume 16, Issue 5, September 2015.
Bucher, MD, et al.
Introduction: Hand hygiene is an important component of infection control efforts. Our primary and
secondary goals were to determine the reported rates of hand washing and stethoscope cleaning in
emergency medical services (EMS) workers, respectively.
Methods: We designed a survey about hand hygiene practices. The survey was distributed to
various national EMS organizations through e-mail. Descriptive statistics were calculated for
survey items (responses on a Likert scale) and subpopulations of survey respondents to identify
relationships between variables. We used analysis of variance to test differences in means between
the subgroups.
Results: There were 1,494 responses. Overall, reported hand hygiene practices were poor among
pre-hospital providers in all clinical situations. Women reported that they washed their hands more
frequently than men overall, although the differences were unlikely to be clinically significant.
Hygiene after invasive procedures was reported to be poor. The presence of available hand sanitizer
in the ambulance did not improve reported hygiene rates but improved reported rates of cleaning
the stethoscope (absolute difference 0.4, p=0.0003). Providers who brought their own sanitizer were
more likely to clean their hands.
Conclusion: Reported hand hygiene is poor amongst pre-hospital providers. There is a need for
future intervention to improve reported performance in pre-hospital provider hand washing.
Volume 16, Issue 5, September 2015.
John Sutter, BS, et al.
Introduction: Out-of-hospital cardiac arrest (OHCA) is a leading cause of death. The 2010
American Heart Association Emergency Cardiovascular Care (ECC) Guidelines recognize
emergency dispatch as an integral component of emergency medical service response to OHCA
and call for all dispatchers to be trained to provide telephone cardiopulmonary resuscitation
(T-CPR) pre-arrival instructions. To begin to measure and improve this critical intervention, this
study describes a nationwide survey of public safety answering points (PSAPs) focusing on the
current practices and resources available to provide T-CPR to callers with the overall goal of
improving survival from OHCA.
Methods: We conducted this survey in 2010, identifying 5,686 PSAPs; 3,555 had valid e-mail
addresses and were contacted. Each received a preliminary e-mail announcing the survey, an e-mail
with a link to the survey, and up to three follow-up e-mails for non-responders. The survey contained
23 primary questions with sub-questions depending on the response selected.
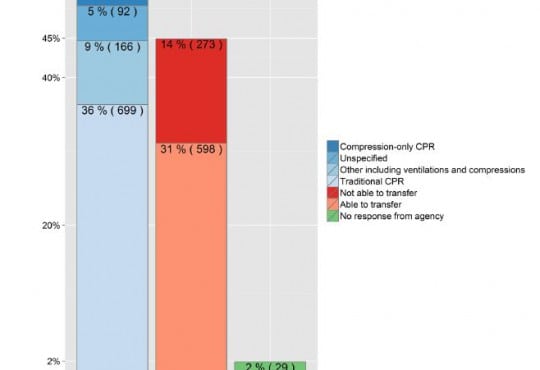
Results: Of the 5,686 identified PSAPs in the United States, 3,555 (63%) received the survey, with
1,924/3,555 (54%) responding. Nearly all were public agencies (n=1,888, 98%). Eight hundred
seventy-eight (46%) responding agencies reported that they provide no instructions for medical
emergencies, and 273 (14%) reported that they are unable to transfer callers to another facility
to provide T-CPR. Of the 1,924 respondents, 975 (51%) reported that they provide pre-arrival
instructions for OHCA: 67 (3%) provide compression-only CPR instructions, 699 (36%) reported
traditional CPR instructions (chest compressions with rescue breathing), 166 (9%) reported some
other instructions incorporating ventilations and compressions, and 92 (5%) did not specify the type
of instructions provided. A validation follow up showed no substantial difference in the provision of
instructions for OHCA by non-responders to the survey.
Conclusion: This is the first large-scale, nationwide assessment of the practices of PSAPs in
the United States regarding T-CPR for OHCA. These data showing that nearly half of the nation’s
PSAPs do not provide T-CPR for OHCA, and very few PSAPs provide compression-only instructions,
suggest that there is significant potential to improve the implementation of this critical link in the
chain of survival for OHCA.
Volume 16, Issue 5, September 2015.
Nikolay Dimitrov, MS, et al.
Introduction: Comprehensive stroke systems of care include routing to the nearest designated
stroke center hospital, bypassing non-designated hospitals. Routing protocols are implemented
at the state or county level and vary in qualification criteria and determination of destination
hospital. We surveyed all counties in the state of California for presence and characteristics of their
prehospital stroke routing protocols.
Methods: Each county’s local emergency medical services agency (LEMSA) was queried for the
presence of a stroke routing protocol. We reviewed these protocols for method of stroke identification
and criteria for patient transport to a stroke center.
Results: Thirty-three LEMSAs serve 58 counties in California with populations ranging from 1,175
to nearly 10 million. Fifteen LEMSAs (45%) had stroke routing protocols, covering 23 counties (40%)
and 68% of the state population. Counties with protocols had higher population density (1,500
vs. 140 persons per square mile). In the six counties without designated stroke centers, patients
meeting criteria were transported out of county. Stroke identification in the field was achieved using
the Cincinnati Prehospital Stroke Screen in 72%, Los Angeles Prehospital Stroke Screen in 7% and
a county-specific protocol in 22%.
Conclusion: California EMS prehospital acute stroke routing protocols cover 68% of the state
population and vary in characteristics including activation by symptom onset time and destination
facility features, reflecting matching of system design to local geographic resources.
Volume 16, Issue 4, July 2015
Sundeep R. Bhat, MD, et al.
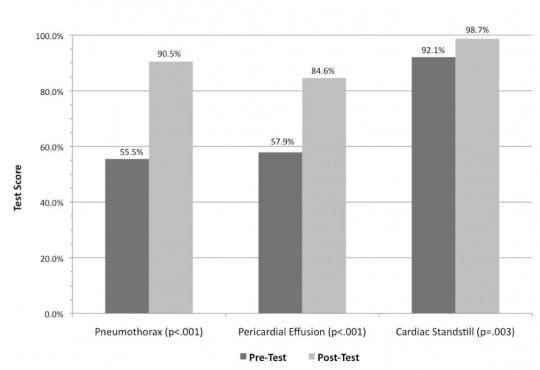
In the United States, there are limited studies regarding use of prehospital ultrasound
(US) by emergency medical service (EMS) providers. Field diagnosis of life-threatening conditions
using US could be of great utility. This study assesses the ability of EMS providers and students to
accurately interpret heart and lung US images.
Volume 16, Issue 3, May 2015
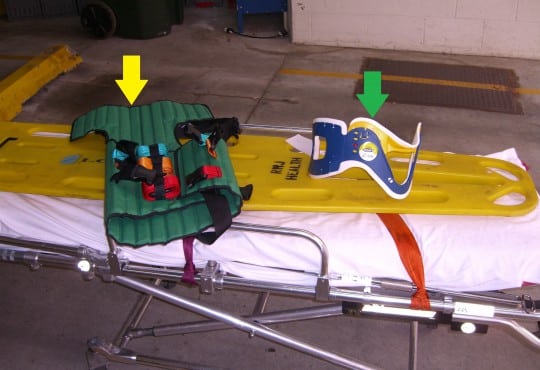
Joshua Bucher, MD, et al.
This is a small experiment that showed decreased patient neck movement using a KED versus RE but resulted in increased patient movement in obese patients. Further studies are needed to determine if the KED improves any meaningful patient outcomes in the era of increased evidence-based medicine in emergency medical services.
No recent data describes the frequency of physical or verbal assaults or which providers have increased fear for their safety. This information may help to guide interventions to improve safety. Our objective was to describe self-reported abuse and perceptions of safety and to determine if there are differences between gender, shift, and years of experience in a busy two-tiered, third service urban EMS system.
Volume 16, Issue 3, May 2015
Justin C. Stowens, MD, et al.
Brief, early notification of STEMI by paramedics through 9-1-1 dispatchers achieves earlier CCL activation in a hospital system already using EMS-directed CCL activation. This practice significantly decreased DTB and yielded a higher percentage of patients meeting the DTB≤60 minutes quality metric.
Volume 16, Issue 3, May 2015
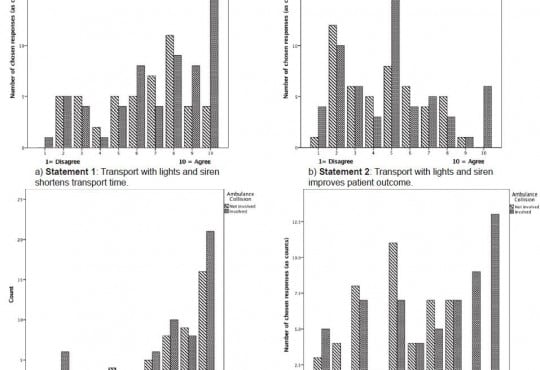
Joseph Tennyson, MD, et al.
The use of warning lights and siren (WLS) increases the risk of ambulance collisions. Multiple studies have failed to demonstrate a clinical benefit to the patients. We sought to investigate the degree to which providers understand the data and incorporate it into their practice.
Volume 15, Issue 7, November 2014
Ling Tiah, MBBS, MPH et al.
Endotracheal intubation (ETI) is currently considered superior to supraglottic airway devices (SGA) for survival and other outcomes among adults with non-traumatic out-of-hospital cardiac arrest (OHCA).
Volume 15, Issue 7, November 2014
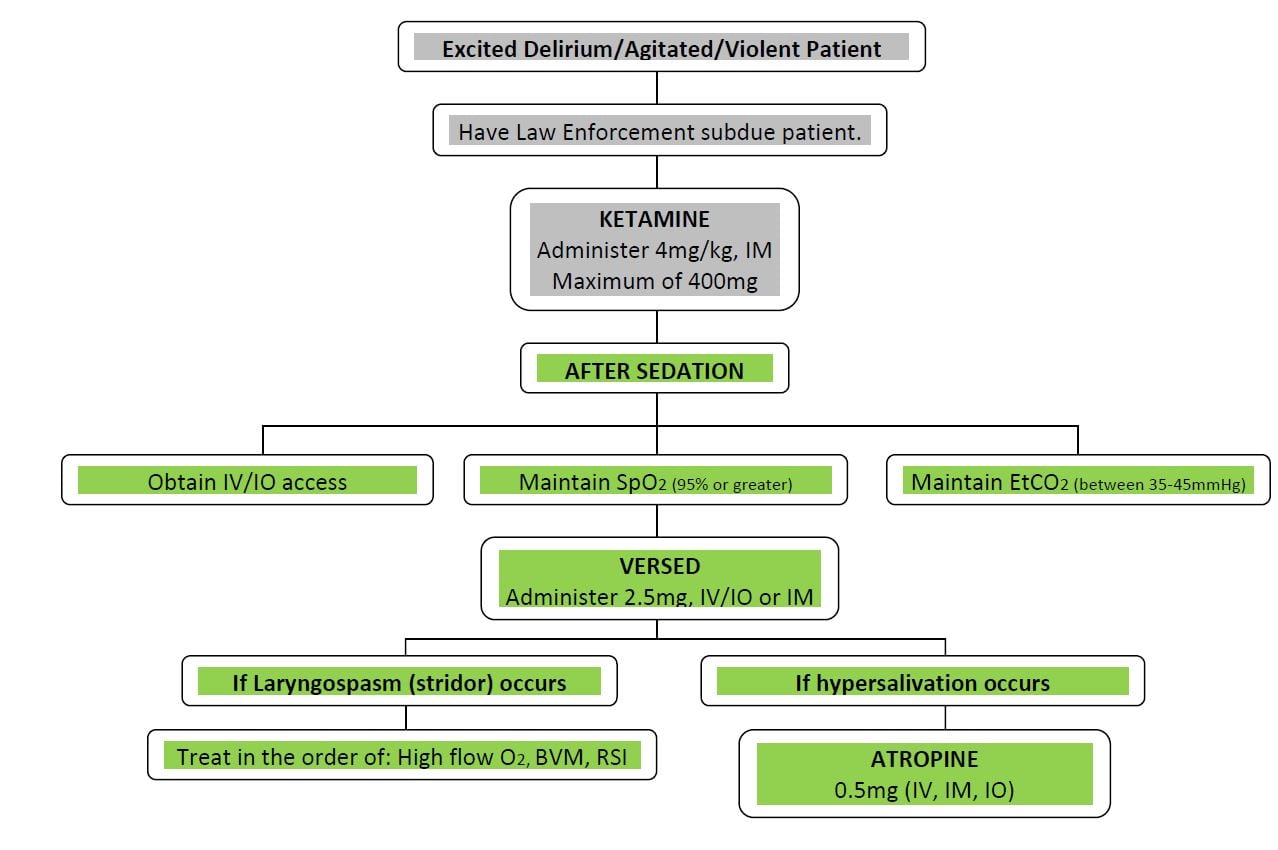
Kenneth A. Scheppke, MD et al.
Violent and agitated patients pose a serious challenge for emergency medical services (EMS) personnel. Rapid control of these patients is paramount to successful prehospital evaluation and also for the safety of both the patient and crew.
Volume 15, Issue 7, November 2014
Carl H. Schultz, MD
Providing acute medical care to severely agitated patients in the pre-hospital setting is a significant challenge. These patients often pose a serious safety threat to themselves and emergency medical services (EMS) providers.
Volume 15, Issue 7, November 2014
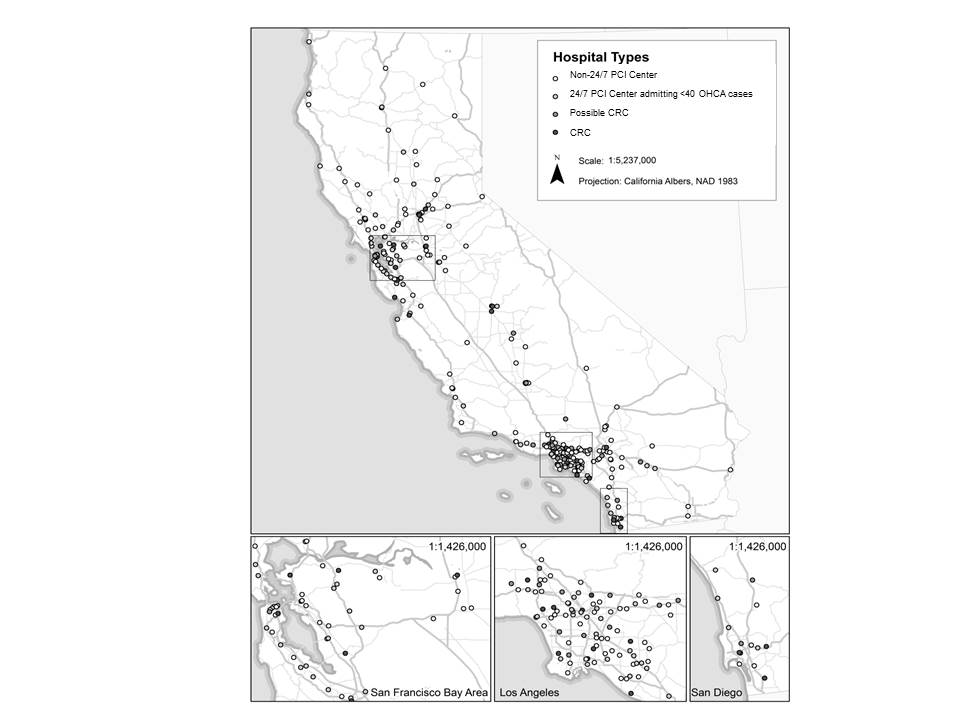
Bryn E. Mumma, MD, MAS et al.
The American Heart Association (AHA) recommends regionalized care following out-of-hospital cardiac arrest (OHCA) at cardiac resuscitation centers (CRCs).
{kind=link}