
{kind=link}
| Author | Affiliation |
| David E. Hogan, DO, MPH | Oklahoma State University, Department of Emergency Medicine, Oklahoma City, Oklahoma |
| Travis Brown, DO | Duncan Regional Hospital, Department of Emergency Medicine, Duncan, Oklahoma |
Introduction
Methods
Results
Discussion
Limitations
Conclusion
INTRODUCTION
The triage of patients during a mass casualty – disaster (MCD) event presents the emergency healthcare provider with a complex and difficult issue. The task of evaluating casualties rapidly, using primarily the skills of physical examination, while still accurately identifying casualties likely to have critical injury or illness, may be impossible to achieve in practice. Yet at the same time it is known that accurate triage under MCD conditions improves outcomes not only for the individual critically ill casualty, but also for the entire cohort of casualties presenting for care.1,2
To improve the accuracy of MCD triage, further scientific investigations must be conducted to determine what elements of the physical examination (determining specific anatomic and physiologic factors) correlate best with the probability of critical injury and illness. These investigations should be – when possible – carried out under conditions that closely approximate the MCD environment. In addition, studies must be carried out as to the utility of new technologies that may be applied to the MCD triage process to improve and extend the ability of the triage officer in rapidly determining the condition of the casualty. Some recent studies have reported on data collected under actual MCD conditions, as well as using computer simulation to approximate the conditions of the MCD environment.3,4 These studies are encouraging and hopefully represent an emerging area of research into this area of emergency healthcare.
One question frequently posed is that of the utility of vital signs, or specific physiologic parameters reflective of formal vital signs, in the performance of MCD triage. Study of this question has been hampered by multiple factors, including the difficulty in collecting such detailed data under actual MCD conditions.1 This paper provides an analysis of the potential impact of abnormal vital signs on clinical triage categorization in comparison to triage categorization derived from actual dispositions of casualties from two separate MCD events.
METHODS
This is a protocol-driven cohort study of data from two separate local institutional review board- (IRB) approved studies of casualties during mass casualty – disaster (MCD) conditions (a terrorist bombing and an F-5 tornado).5,6 Additional approval of a protocol to study the two anonymous database collections was granted from the local facility IRB. We queried the database collections for cases with complete data points to include: initial clinical triage category, initial vital sign documentation, emergency department (ED) diagnosis, and final patient disposition.
Clinical triage categorization is defined as the initial triage category assigned to the casualty by the triage officer at the level of the ED and documented in the medical record. To assess the agreement of the clinical triage categorization with a standard, we applied a revised triage category to each case. This revised category is termed disposition triage category, and is based on ED disposition as an indicator of the severity of injury/illness for the case as utilized in previous studies.5-7 This does not relate to the level of documentation found in the chart but rather to individual decisions of admission vs discharge. In addition, decisions as to where the casualty is admitted (taken to the operating room, intensive care unit, ward bed, etc.) are well preserved in most medical records after MCD event and are thought to relate directly with the level of casualty injury or illness. Under this protocol the ED disposition relates with disposition triage categorization as follows:
Category I (Immediate)-Operating Room or Critical Care Admission; Category II (Delayed)-Noncritical Care Admission; Category III (Minimal)-Discharge Home; Category IV (Expectant)-Excluded From Analysis.
The disposition triage category is used as a standard for calculation of overtriage (OT) and undertriage (UT) rates of the clinical triage category assignment.
Recorded vital signs are scored as normal or abnormal using the standard adult and age-adjusted vital signs for children as recommended in Steadman’s Medical Dictionary.8 The Glasgow Coma Score (GCS) is recorded in the database as a total score without scoring of the individual parameters. Any score less than 15 is considered abnormal.
Because the triage data thus obtained are ordinal (ranked) in nature, agreement between clinical and disposition triage categories is assessed using the weighted kappa test and is reported as raw agreement, κ with the 95% confidence interval and probability. In addition, agreement using the Kendall tau statistic is performed and reported as τ and probability. Linear regression is also performed using first the clinical triage categories as the dependent variable then the disposition-adjusted triage categories against the independent variables of Glasgow Coma Score, pulse, respiration, and systolic blood pressure. The results of correlation are reported as r with 95% confidence interval and probability. We performed statistical analysis with Microsoft Office Excel® (version 11.5612.5606) and the statistical add-on package Analyze-it® (version 2.05).
RESULTS
Out of a total of 535 cases in the two database sets (388 bombing, 147 tornadodo) 103 (19.25%) cases met case criteria; 46 male, 57 female; mean age 35yr (range 86 – 1 years). The clinical triage categories and event sources of cases are demonstrated in Figure 1. There are no significant differences between the cases meeting inclusion criteria and those excluded in age or sex, p=0.765. Three category IV (expectant) cases were excluded from further analysis (all 3 expectant casualties had no signs of life on presentation to the ED) leaving 100 cases fit for analysis, Category I; 23, Category II; 11, Category III; 66. Rates for Undertriage (UT) and Overtriage (OT) comparing the clinical triage categories to disposition triage categories are UT=35% and OT=1%.
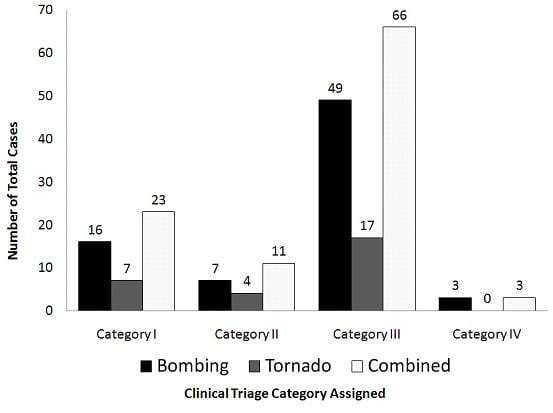
Figure. Distribution of mass casualty-disaster cases by clinical triage category and event type.
Evaluation of agreement between clinical and disposition triage categories provided a raw agreement of 0.540 and κ=0.33 (95% CI: 0.21 to 0.45) p<0.0001 indicating a “fair” level of agreement. Linear regression using the clinical triage categories as the dependent variable and GCS, heart rate, respiratory rate, and systolic blood pressure as the independent variables found a significant but small agreement with GCS: r=0.1425 (95% CI: 0.0937 to 0.1913) p<0.0001. Substitution of the disposition triage categories for y in the same regression demonstrated similar small agreement with both GCS [r=0.06994 (95% CI: 0.01829 to 0.12160) p=0.0085] and systolic blood pressure [r=0.00895 (95% CI: 0.00309 to 0.01481) p=0.0031]. The vital signs of abnormal pulse rate and abnormal respiratory rate are not noted to have significant levels of agreement with disposition triage categories.
DISCUSSION
In general small numbers of cases were found with documentation of clinical triage categorizations and initial vital signs in the two study databases. This is consistent with the usual level of documentation that occurs during MCD events.9 This is one of the issues making the study of the actual process of triage during MCD conditions so difficult. The low numbers can make the impact of any variable such as vital signs on triage categorization more difficult to resolve.
Undertriage, defined as the triage of a critical casualty as noncritical and overtriage, defined as the triage of a noncritical casualty as critical, are consistent problems encountered in MCD triage.1 Overtriage has been reported to have an adverse impact on the outcomes of critical casualty cohort due to a misdirection and dilution of critical care resources away from truly critical casualties.2,10 Undertriage primarily impacts the individual casualty by delaying his/her critical care interventions. Undertriage rates of 5% or less and overtriage rates of up to 50% have been generally agreed to be acceptable in prior publications.10-13 The difficulties of studying activities of triage during MCD conditions are multiple and persistent.1,14 The nature of these difficulties makes it even more challenging to evaluate the MCD triage process for the impacts of individual process elements (such as physiologic parameters). To our knowledge, this study includes some of the only data reported regarding a potential impact of vital signs on triage categorization collected under actual MCD conditions. As such, even with generally low numbers, there is value in their analysis, as long as that value is taken in the context of the study limitations.
Improvement of the MCD triage process is an important goal of emergency healthcare providers. The process of triage must obtain sufficient information regarding the anatomic and physiologic state of the casualty to avoid high levels of mistriage, which are known to adversely impact the entire cohort of injured/ill casualties.2 At the same time the triage evaluation itself must remain nimble and abbreviated to prevent a bogging down of the process. As such, any elements of evaluation included in a “standardized” triage process should be validated as much as possible scientifically.
The data of this study demonstrate a small but significant level of agreement with increasing severity of triage categorization for mental status (based on the GCS) and systolic blood pressure. This suggests that a rapid mental status evaluation (such as the Mental status Alert, responsive to Verbal or Painful Stimuli or Unresponsive method or GCS) as well as an evaluation for a radial pulse (as a surrogate for systolic blood pressure measurement) may be useful in improving the accuracy of MCD triage.
The presence of a radial pulse (as well as the strength and character of a radial pulse) has been
{kind=link}