
{kind=link}
| Author | Affiliation |
|---|---|
| Pankaj B. Patel, MD | Department of Emergency Medicine, The Permanente Medical Group, Kaiser Permanente Medical Centers, Sacramento and Roseville, California |
| Hannah Elise Anderson, | Department of Emergency Medicine, The Permanente Medical Group, Kaiser Permanente Medical Centers, Sacramento and Roseville, California |
| Lisa D. Keenly, MD | Department of Emergency Medicine, The Permanente Medical Group, Kaiser Permanente Medical Centers, Sacramento and Roseville, California |
| David R. Vinson, MD | Department of Emergency Medicine, The Permanente Medical Group, Kaiser Permanente Medical Centers, Sacramento and Roseville, California |
Introduction
Materials and methods
Results
Limitations
Discussion
ABSTRACT
Introduction: Informed consent is a required process for procedures performed in the emergency department (ED), though it is not clear how often or adequately it is obtained by emergency physicians. Incomplete performance and documentation of informed consent can lead to patient complaints, medico-legal risk, and inadequate education for the patient/guardian about the procedure. We undertook this study to quantify the incidence of informed consent documentation in the ED setting for lumbar puncture (LP) and to compare rates between pediatric (<18 years) and adult patients.
Methods: In this retrospective cohort study, we reviewed the ED electronic health records (EHR) for all patients who underwent successful LPs in 3 EDs between April 2010 and June 2012. Specific elements of informed consent documentation were reviewed. These elements included the presence of general ED and LP-specific consent forms, signatures of patient/guardian, witness, and physician, documentation of purpose, risks, benefits, alternatives, and explanation of the LP. We also reviewed the use of educational material about the LP and LP-specific discharge information.
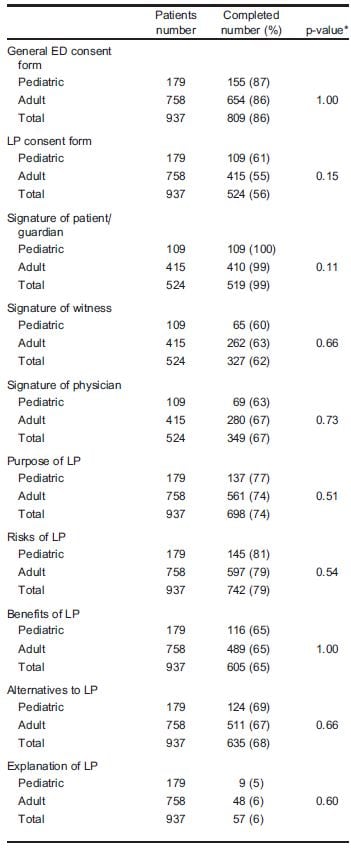
Results: Our cohort included 937 patients; 179 (19.1%) were pediatric. A signed general ED consent form was present in the EHR for 809 (86%) patients. A consent form for the LP was present for 524 (56%) patients, with signatures from 519 (99%) patients/guardians, 327 (62%) witnesses, and 349 (67%) physicians. Documentation rates in the EHR were as follows: purpose (698; 74%), risks (742; 79%), benefits (605; 65%), alternatives (635; 68%), and explanation for the LP (57; 6%). Educational material about the LP was not documented as having been given to any of the patients and LP-specific discharge information was documented as given to 21 (2%) patients. No significant differences were observed in the documentation of informed consent elements between pediatric and adult patients.
Conclusion: General ED consent was obtained in the vast majority of patients, but use of a specific LP consent form and documentation of the elements of informed consent for LP in the ED were suboptimal, though comparable between pediatric and adult patients. There is significant opportunity for improvement in many aspects of documenting informed consent for LP in the ED. [West J Emerg Med. 2014;15(3):318–324.]
INTRODUCTION
Background
Consent for medical treatment has had an interesting history, from Hippocrates’ advice to physicians to conceal medical information from their patients1,2 to the current consensus that physicians have a legal and moral obligation to provide patients with all necessary information to make informed decisions.3,4 Following the unethical experimentation on prisoners by Nazis and the Nuremberg trials from World War II, simple consent to medical treatment became well-established in the United States.5,6 A 1957 court decision in which a patient sued his physicians for their failure to inform him of the risk of paralysis after a translumbar arteriogram articulated the need for more comprehensive consent,1–3,7–9 moving from simple consent, i.e., “did the patient agree to be treated?”, to informed consent, i.e., “did the physician provide the patient with an adequate amount of information?”10
Informed consent consists of various basic features: the principle of autonomy (the patient’s right to self-determination), disclosure of information through a process that is understandable (including diagnosis, purpose, risks/benefits, and alternatives), patient understanding of the information provided, an opportunity to ask questions, and voluntary decision-making such that a patient is not coerced into making a decision.2,4,5,10–14
Importance
The American Medical Association has published principles of medical ethics with guidelines for physicians to seek informed consent for specific medical interventions and to disclose all relevant medical information to their patients, which include risks and benefits of treatment options.15–17 In efforts to comply with such guidelines, most hospitals have used consent forms, but there is no standardized approach to providing informed consent.
Informed consent has several benefits. Incorporating informed consent training for healthcare professionals upholds ethical and legal rights for patients.18 Informed consent discussions can foster the patient’s trust in the physician. The therapeutic value of obtaining informed consent can enhance satisfaction of both the physician and patient in the professional relationship.11 An informed patient or guardian who actively participates in decision-making will also have a better appreciation of the strengths and limitations of their medical care.19,20 Moreover, the improvements in relationship and knowledge can result in the reduction of liability occurrence.21
Goals of This Investigation
Though documentation of informed consent is recommended, compliance with the process of informed consent is inconsistent.22,23 Most informed consent procedures are incomplete, with deficiencies in one or more of the various elements that are required for a complete informed consent process.23 To evaluate our own informed consent compliance, we reviewed the electronic health records (EHR) of all patients who underwent successful lumbar puncture (LP) in 3 emergency departments (ED). Medical records for all 3 EDs are electronic, with no paper charting (consent forms are scanned into the EHR). Medical information is entered into the EHR in various ways by emergency physicians (EP), including free text, templates, and/or speech recognition software. Our primary objective was to compare the rates of documentation for various elements of informed consent for LP in pediatric and adult patients. The consent process differs for pediatric versus adult patients, as pediatric patients are not competent to provide consent and their parents/guardians have the responsibility to provide that consent.20 When the welfare of a child is at stake, we suspected that physicians would be more attentive in explaining the procedure to allay fears of the parents/guardians and to answer their questions. We hypothesized that EPs would be more thorough in their documentation of the informed consent process when the procedure involved a child. We also wanted to ascertain how often a consent form for the LP was in the EHR and the rate at which signatures were obtained from the patient/guardian, physician, and witness. Finally, we sought to identify future opportunities to improve our informed consent process by assessing the educational resources that were used by our physicians in our current consent process.
MATERIALS AND METHODS
Study Design
This was a retrospective cohort study undertaken from April 2010 through June 2012.
Setting and Selection of Participants
We identified all pediatric (<18 years) and adult ED patients who underwent a successful LP through a laboratory database of cases undergoing cerebrospinal fluid (CSF) analysis. The study was performed at 3 hospitals within Kaiser Permanente (KP) Northern California, a large integrated healthcare delivery system serving approximately 3.4 million members at 21 hospitals and more than 160 medical offices. The 3 EDs are staffed by approximately 150 board-certified or board-prepared EPs along with emergency medicine residents (at 2 of the 3 EDs) and serve a broad spectrum of patients that includes pediatric and obstetric patients. While all EPs in this study belong to the same medical group, one subgroup covers 2 of the 3 EDs, while a separate subgroup staffs the third ED. Each ED had an annual census during the study period of approximately 75,000 patients. The Kaiser Permanente Northern California Health Services Institutional Review Board reviewed this study and granted it an exemption.
Methods of Measurement
Study investigators abstracted data from the index ED visit EHR using a structured computerized data collection tool. Multiple processes were instituted to enhance the accuracy and reliability of the data abstraction process, following methodologic standards for chart review.24 We identified inclusion criteria in advance of the study. All abstractors received training on the content and coding of each data element, data handling and data transmission procedures, and protocols to handle possible questions or problems during the study. The principal investigator monitored day-to-day data collection activities and answered coding questions. Ambiguous results were arbitrated by discussion with the principal investigator. Two different investigators reviewed random cases to assess interrater reliability for each of the 26 variables measured. Finally, as each of our authors had discussed this research study, it was not feasible to blind our abstractors to the study hypotheses. However, none of the abstractors were invested in any particular outcome, other than to study and identify current practice for informed consent documentation.
Demographic and clinical variables included age, sex, computed tomography or magnetic resonance imaging done in the ED, and hospital admission rates for each of the EDs and groups of patients. Documentation of the elements of informed consent (yes/no) included the following: presence of generalized ED consent form, LP consent form (and signatures for the patient/guardian, physician, and witness), diagnostic purpose for LP (infection, bleeding, brain hypertension, other), risks (headache, bleeding, infection, pain, leg weakness, brain herniation, apnea in patients under 3 years of age, neurological problems), benefits, and alternatives. Physicians did not have to document the details of the risks (or other elements of informed consent or education provided) by listing them one by one to be given credit. Simply documenting that these elements were discussed with the patient/guardian was sufficient. Additional documentation variables included an explanation of the procedure, use of LP-specific educational material, use of LP-specific discharge information, and questions solicited and answered. Lastly, we noted the presence of an LP procedure note in the EHR.
Primary Data Analysis
Continuous variables are presented as medians with interquartile ranges. Categorical data are presented as frequencies and proportions. Descriptive statistics were performed with standard software (Microsoft Excel, version 14.0, 2010; Microsoft Corporation, Redmond, WA). We performed comparisons using the two-tailed Fisher’s exact test (GraphPad Software, Inc., 2013 edition; La Jolla, CA). We considered a p-value of less than 0.05 to indicate statistical significance.
RESULTS
During the 27-month study period we identified 937 ED patients who underwent successful LP. Unsuccessful LPs in which CSF did not undergo laboratory analysis were not identified or included in this study. Of the total cohort, 179 (19.1%) were pediatric cases and 758 (80.9%) were adult cases. No patient underwent more than one successful LP in the ED during the study period.
The age range for the entire cohort was 2 days to 93 years. Demographics and resource utilization, both overall and per age-specific populations, are reported in Table 1. Documentation rates for each variable of the total cohort, as well as the age-specific populations, are reported in Table 2. Rates of documentation were not significantly different between pediatric and adult patients.
Table 1.Characteristics of patients receiving lumbar puncture in the emergency department (ED).
![]()
Table 2.Documentation rates for specific elements of the informed consent process.

Table 2. Continued.
Interrater reliability was ascertained for 206 (22%) of the 937 cases. The mean percent agreement for the 26 separate variables was 98% (range 95% – 100%).
LIMITATIONS
Our study cohort of ED patients undergoing an LP is incomplete since we included only patients who had a successful LP and did not include patients whose LP did not yield CSF for analysis. We do not know exactly how many LPs during the study period had failed to obtain any CSF, the rate of which varies widely in the emergency medicine literature, generally from 2% to 15%,25,26 and higher among medical students and residents.27 We cannot say whether physicians with higher rates of unsuccessful LPs, more of whose cases were excluded from this study, might have different patterns of informed consent documentation than physicians with higher rates of procedural success. However, documentation of pre-procedural informed consent processes would not be significantly different in cases where the LP proved to be ultimately unsuccessful. Since the study did not focus on the LP procedure itself (successful or not successful), the nature of the pre-procedure consent would not be altered by the subsequent result of the LP procedure. Of note, inclusion criteria for EHR review were for all LPs done by EPs, excluding LPs that were subsequently performed successfully by other specialists.
Documentation of informed consent in the EHR may not accurately reflect the actual physician/patient conversation that preceded the procedure. Documentation could well err in both directions of under- and over-reporting. With regard to underreporting, physicians may fail to document all the elements that were communicated in dialogue with patients and their parents/guardians. On the other hand, over-reporting is made easier with the availability of EHR templates. In either case, the documentation should reflect the details of the informed consent conversation as it actually transpired and remains the only basis on which the quality and completeness of the process can be judged after the fact.
We selected 3 EDs in our local area to identify the documentation practices for LP consent. Though there is significant variability among these EDs and their patient populations, our results may not be generalizable to all EDs across the U.S.
During the study period, 2 of the 3 EDs had emergency medicine residents who worked with assigned attending physicians for the LP procedure. Attending physicians ultimately had the primary responsibility for assuring that LP consent was obtained and documented in the medical record.
The patients’ conditions, urgency of the LP, and the mental status of patients/guardians could all impact the type of discussion and subsequent documentation that occurred. Patients who present to the ED and require LPs are deemed to be urgent or emergent, addressing this issue of the patient’s condition and urgency of the procedure. Yet the competency/capability to provide informed consent was documented in only 1% of all patients for this study. Further, this issue was not addressed for the parents/guardians of any pediatric patient in this study, something that could impact the type of discussion/documentation about procedures done in the ED, raising an opportunity for future research.
Documentation of informed consent may not be a reliable evaluation of what actually took place prior to the LP. However, the current standard of care in this area is to obtain a signed consent form, with documentation about the discussion of the purpose, risks, benefits, and alternatives to the procedure. Our only avenue for obtaining informed consent is what this study reviews, i.e., a signed consent form with documentation of the relevant items.
DISCUSSION
Our data showed that generalized ED consent is obtained in the vast majority of ED patients who had an LP performed but just over one-half of these patients had a specific LP consent form in the EHR. Documentation of purpose, risks, benefits, and alternatives for the LP was noted in approximately 70% of the cases. Our data also showed that the rates of documentation for pediatric patients were not superior to their adult counterparts. Documentation of the educational component of the informed consent process, as measured by documentation of an explanation of the LP, the use of educational material, and LP-specific discharge information, was rarely found in the EHR. Our study of informed consent for lumbar puncture in the ED for all patients (adults and pediatrics) is the first of its kind to our knowledge. Despite the expectation for a signed informed consent in every chart, the data showed that this is not always achieved.
Generalized ED consent was obtained for the vast majority of patients who presented to the ED during the study period. The presence of this generalized consent may have been deemed by EPs to be adequate for procedures like an LP, leading to no further effort to obtain informed consent through the use of an LP-specific consent form. Variables that decrease the perceived need for seeking LP-specific informed consent by physicians in the ED setting could include the following: patients’ very presence in the ED often indicates an urgent or emergent medical condition;28 similar to other emergent procedures like paracentesis and thoracentesis, there are limited alternative options to an LP, which is usually needed emergently and has a high benefit-to-risk profile;20 ED patients are in a stressful medical situation that may affect their decision-making.12 In these situations, an additional LP specific form does not provide liability protection by itself,6,29 nor does it meet the true spirit of the informed consent process, which may further reduce the likelihood of use by physicians.
Our overall compliance for documenting the various aspects of informed consent (purpose, risk, benefits, and alternatives) was found to be similar to prior studies performed in different settings: purpose (our study 74%; other studies 92% to 94%); risks (our study 79%; other studies 59% to 88%), benefits (our study 65%; other studies 36% to 59%); alternatives (our study 68%; other studies 13% to 62%).30,31 In a study reviewing 1,057 audiotaped patient encounters, purpose was noted in 84%, risks/benefits (pros and cons) were noted in 26%, and alternatives were noted in 30%.32 From these data, we conclude that inadequate compliance with informed consent documentation is a prevalent issue. The use of a standardized form to obtain consent could help improve compliance, though a review of 157 hospitals nationwide found that the content of 540 informed consent forms for procedures in those hospitals was inadequate for addressing the standards for informed consent.33 Even when consent forms are provided, many patients or their parents/guardians do not take the time to carefully read them, believing that the forms are there to protect the physician.34 Also, comprehension of the informed consent information can be very challenging for the patient or parent/guardian.35 As a result, a full review of informed consent may not occur, which is then reflected in a lack of documentation of the various aspects of informed consent.
Our data showed that the compliance rate for documenting informed consent for pediatric patients undergoing an LP was not superior to that for adult patients. Informed consent for the pediatric population has some unique challenges. While competent adult patients have a right to refuse treatment for any reason, the parent/guardian of a pediatric patient may not have the same absolute right to refuse treatment for their child.20 Specific issues related to obtaining adequate parental consent for patients younger than 16 years of age resulted in the suspension of a pediatric study until such issues could be resolved through federal regulations.36 With respect to the pediatric population, we hypothesized that our physicians might seek more specific documentation compliance for this patient group compared with adult patients. However, our results did not support our hypothesis.
Our pediatric results are generally consistent with reports from other facilities. In a Chicago Children’s Memorial Hospital Pediatric ED study, informed consent documentation for an LP was deemed to be inadequate.30 Comparing their findings with our study data for pediatric patients, they had higher rates of documentation of purpose (94% vs. 74%), risks (88% vs. 81%), and use of a consent form (88% vs. 61%), but a lower rate of documentation of benefits (36% vs. 65%) and alternatives (13% vs. 69%). Further work is needed to improve the documentation rates of informed consent for pediatric, as well as adult, patients.
Documentation of various aspects of patient education with regard to the LP was also found to be inadequate in our study. Our EDs have not used educational tools for an LP, as have been implemented in other settings for improving informed consent. These tools include supplemental written educational forms, video tools, or computer-based education.23 The lack of educational material usage in our study represents a significant opportunity for future work to improve the informed consent process for an LP. Research suggests that a minority of patients fully read informed consent information, ask questions, or accept a copy of the consent document.12 However, if an educational model were developed for providing informed consent that is simple and accessible, and geared toward an appropriate grade level of understanding, patients may increase their engagement with the process. Improved patient participation in the informed consent process would lead to a greater sense of control, improved compliance, and perhaps even improved healthcare outcomes. Patient education may also reduce medical errors,37 as the process allows the patient to not just be a passive observer, but an active participant in the LP procedure. Sharing information with the patient or parent/guardian improves communication and cooperation and assures better understanding of the procedure by the patient.3 Such communications may strengthen the doctor-patient relationship by enhancing mutual trust and cooperation.29
In conclusion, we found that documentation of informed consent for the general ED visit was excellent. There was room for improvement, however, in obtaining LP-specific informed consent. There was little difference in documentation compliance for informed consent between pediatric and adult patients. Educational material was rarely used and documentation of an explanation of the LP to patients rarely occurred. There are significant opportunities to improve the overall informed consent process for an LP in the ED that begins with education for physicians about informed consent. We would like to undertake a future study to identify how to improve the informed consent process for LP and assess what patients actually understood about the procedure, using a checklist that includes pre-LP educational materials for the patient/guardian, LP-specific discharge instructions for the patient/guardian, and follow-up contact with the patient or guardian to directly assess their knowledge about the LP after this new informed consent process is implemented.
Footnotes
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
Supervising Section Editor: Erik Barton, MD, MS, MBA
Address for Correspondence: Pankaj Patel, MD. 1600 Eureka Road, Roseville, CA 95661. Email: pankaj.patel@kp.org. 5 / 2014; 15:318 – 324
Submission history: Revision received August 22, 2013; Submitted January 2, 2014; Accepted January 7, 2014
Full text available through open access at http://escholarship.org/uc/uciem_westjem
REFERENCES
1. Katz J. Informed consent in the therapeutic relationship: Legal and ethical aspects. In: Reich WT, editor.Encyclopedia of Bioethics (vol 2) New York, NY: Free Press; 1978. pp. 770–778. In. (ed)