
{kind=link}
| Author | Affiliation |
|---|---|
| Sheryl M Strasser, PhD, MPH, MSW | Georgia State University, Institute of Public Health, Atlanta, Georgia |
| Megan Smith, MPH, BA | Georgia State University, Institute of Public Health, Atlanta, Georgia |
| Danielle Pendrick-Denney, MPH, BA | Georgia State University, Institute of Public Health, Atlanta, Georgia |
| Sarah Boos-Beddington, MPH, BS | Georgia State University, Institute of Public Health, Atlanta, Georgia |
| Ken Chen, MPH, MBA, MS | Centers for Disease Control, Financial Management Office, Atlanta, Georgia |
| Frances McCarty, PhD | Georgia State University, Institute of Public Health, Atlanta, Georgia |
ABSTRACT
Intimate Partner Violence (IPV) is a major public health issue occurring in the United States and globally. While little is known in general about IPV, understanding about the prevalence of physical IPV among gay men is even more obscure. There is a clear disparity in violence research attention focused on this vulnerable segment of society. This cross-sectional survey study was conducted to examine the feasibility of enrolling 100 gay men from Atlanta into an IPV survey study. The survey was administered via Facebook. Ninety-nine usable surveys were collected. Chi-square tests reveal that minority ethnic status, illicit drug use, and non-disclosed orientation status were all significantly associated with positive IPV reports–in terms of both victimization as well as perpetration. Overall, the majority of the study sample indicated that they believe IPV is a health problem in the Atlanta gay community. These findings bear importance for the Atlanta gay community and public health professionals who must address this nearly invisible yet increasing public health issue.
INTRODUCTION
Intimate partner violence (IPV) among same-sex couples is getting increasing attention, although researchers concur that the subject is still poorly understood.1–3 IPV falls under the overarching umbrella of domestic violence (DV) and is defined as “violence between two people in close relationship which includes current and former spouses and dating partners.”4 The World Health Organization further elaborated on the definition to include “acts of physical aggression, psychological abuse, forced intercourse and other forms of sexual coercion, and various controlling behaviors, such as isolating a person from family and friends or restricting access to information and assistance.” 5
Overall, IPV among both heterosexual and homosexual couples accounts for 7.7 million physical assaults and rapes each year, 62% among women and 38% among men, yet many incidents go unreported.6 Following HIV/AIDS and substance abuse, IPV has been described as the third largest public health issue facing gay men.7 Men in same-sex relationships experience abuse rates similar to those of women, an estimated 25 to 33%, yet men in same-sex relationships are twice as likely to suffer abuse as men in heterosexual relationships.7–8 A study of men who have sex with men (MSM) revealed that 34% of the study sample (N=2,881) suffered psychological battery, 22% had been victims of physical battery and 5% had been sexually battered, rates substantially higher than those of heterosexual men.9 More recently, results of a random sample of 284 gay and bisexual men residing in British Columbia indicated that nearly all respondents had been psychologically abused, over one-third had been physically abused, and 10% of respondents reported having been forced or coerced into unwanted sexual activity.10
Health Outcomes
A significant body of evidence cites positive correlations between IPV and poor physical and mental health outcomes, although the majority of research has focused on women.10–12 Immediate and long-term negative health outcomes of IPV include physical injury, chronic pain syndromes, gastrointestinal disorders, and depression or suicidal behaviors, as well as substance use and chronic mental and physical illness.5,11 Abused men in same-sex relationships are more likely to report health issues such as hypertension, obesity, depression, smoking-related illness, sexually transmitted infections; additionally, men in abusive relationships are more likely to engage in unprotected sex and substance abuse. 3
The nature of IPV and lack of useful resources and guidance have discouraged victims from reporting abuse, and widespread ignorance and misconceptions about same-sex IPV have created barriers for treatment services among victims. Recent studies have shown that victims of same-sex IPV are more likely to seek help from informal sources, such as friends, because available formal sources, such as battered women’s services, were perceived as unhelpful.13,14 Additionally, shelters for victims of battery are predominately unequipped to serve men of any sexual orientation.13,14 Recent research of IPV failed to find any significant difference in the number of medical visits between abused and non-abused men, which may suggest that cultural and/or institutional barriers prevent abused men from obtaining assistance.3
Correlates of IPV Among Gay Men
Many correlates of same-sex male IPV have been identified in the literature, including age, education, income, HIV status, risky sexual behaviors, alcohol/drug use, disclosed status and childhood abuse/family violence, although results are mixed. Greenwood et al15 found that younger age (<40) was the strongest demographic correlate of all forms of psychological, physical, and sexual battery. Merrill and Woolfe13 reported that the majority of gay and bisexual male survey respondents were between the ages of 25 and 50; 26- to 35year-olds represented 54% of respondents. However, a 2008 study examining correlates of IPV failed to find a significant association with age.9
Income and educational attainment have been found to be inversely associated with both perpetration and receipt of abuse.9 Similarly, Houston and McKirnan3 reported that higher socioeconomic status (SES) provided some degree of protection from same-sex IPV, as compared to low and middle SES. Problem-solving skills, such as negotiating or compromising obtained through education or personal experience, may provide a buffer.16,17 To the contrary, Stall et al18 did not find significant associations between IPV and education or income level.
The prevalence of experiencing violence in childhood has also been cited as a correlate of IPV. A study of African-American MSM found that those who readily disclosed having male sex partners reported significantly higher rates of early physical abuse, sexual abuse, and lifetime abuse when compared with non-MSM. Further, all MSM who experienced early abuse were more likely to be victims or perpetrators of IPV later in life.19 Craft and Serovich20 reported that experiencing parental abuse during childhood was positively correlated with perpetration of physical assault and both perpetration and receipt of sexual coercion. Similarly, a study of Puerto Rican gay men reported that those who reported violence in their relationships also reported experiencing violence in their childhood home.21
The prevalence of alcohol and drug use has also been found to be higher among cases of same-sex IPV.22,23 McClennen et al14 reported that substance abuse was significantly associated with IPV among both gay men and lesbians. Higher substance use rates among same sex couples were thought to have been a coping mechanism for dealing with stress experienced as a result of societal homophobia and by internalized homophobia.22,24
IPV has also been associated with public disclosure of sexual orientation. Bartholemew et al9 reported that disclosure was positively associated with being the recipient of physical abuse. However, it is possible that those who remain undisclosed and fear being “outed” by their partners are more likely to remain in abusive relationships.
Same Sex Relationships in Atlanta, Georgia
According to United States Census Population Estimates Program, in the year 2000 unmarried same-sex partners constituted 2.7% (11,402) of households in Atlanta, Georgia.25 Atlanta has almost twice as many cohabitating same-sex partners than the national average.26 The Center for Positive Aging has identified 13% of Atlanta’s population as Lesbian Gay Bisexual Transgender [LGBT].27 Additionally, the Williams Institute ranked Atlanta 5th with respect to cities having the highest percentage of gays, lesbians, and bisexuals.28
Atlanta’s high number of same-sex couples makes it an appropriate location for a feasibility study of IPV using social media to examine sociodemographic factors as they relate to this issue. The purpose of this study was to 1) determine if social media, specifically Facebook, is a feasible method of recruiting a substantial study sample for survey participation; 2) measure the prevalence of physical IPV victimization and perpetration among the study sample; and 3) determine if the following variables were associated with positive reports of physical IPV among the study population: age, ethnicity, education level, drug and alcohol use, risky sexual behavior, and disclosure status.
METHODS
We used an anonymous, cross-sectional survey design to conduct this study. Given the exploratory nature of conducting IPV research on a relatively unknown study group, this study was developed to assess the feasibility of recruiting 100 participants who met the eligibility criteria. We created and administered the survey instrument using a licensed Psychdata account. The approved Institutional Review Board application for an expedited study was uploaded into the survey. We added a hyper-text link to the survey as an ‘event’ entitled Feasibility Study of Gay Intimate Partner Violence in Atlanta to a Facebook group dedicated to the gay male community living in Atlanta. Then, the researcher sent a mass e-mail to all members of this Facebook group to explore the new event. The event explained the nature of the survey, and individuals, if interested, were to click on the link. If the survey link was selected, a potential study participant viewed the informed consent document. The content of the informed consent document detailed the overarching research question, the number of survey items, and where to direct questions about the study, as well as resources that provided information and services focusing on IPV in Atlanta. The e-mail invitation also encouraged participants to forward the invitation to other potential candidates; therefore, we also employed a snowball methodology of recruiting study participants. Study eligibility criteria were identified as being a gay men currently residing in Atlanta, Georgia.
Study Instrumentation
The study survey consisted of 49 items. Twenty-five of the survey items were from the Partner Abuse Scale-Physical (PASPH), and the principal investigator (PI) created the remaining 24 items.29 The PASPH is designed to measure the severity of physical abuse in a didactic relationship and asks the survey respondent to answer questions about the types and frequency of abuse they have received from their partners. The instrument was created in 1997 and its psychometric properties indicate that it is a highly reliable scale (reliability coefficient of .9). Scores range from 0 to 100, where higher scores indicate greater amounts of physical abuse.
Sociodemographic items developed by the PI included questions regarding the participants’ race, age, and educational attainment. Additional questions queried participants about their disclosure status (whether or not they are openly gay) and substance use. For the purposes of this survey, items that queried participants’ prescription drug use referred to participants’ use of medications prescribed by a physician; additional questions examined participants’ use of tobacco, alcohol and illicit drugs. Other items developed by the PI asked participants if they believed that IPV was a health issue in the Atlanta gay community, and whether or not they are aware of any gay male relationships (current or past) involving IPV.
In addition to questions about victimization provided by the PASPH, the PI also included 3 questions asking whether or not the survey participant had been the perpetrator of violence against his intimate partner. Victimization of IPV was indicated if a respondent indicated that he had been the recipient of violence or had been threatened with violence by his intimate partner. Perpetration was indicated if the respondent provided any positive report of delivering physical harm or threatening to harm his partner. Therefore, we coded any response, other than “never,” to the 25 PASPH items as positive for IPV victimization, and any affirmative response to the 3 questions regarding perpetration of violence as positive for IPV perpetration.
RESULTS
Once the PI received 100 completed surveys, the survey was officially closed and the online event was removed. Data was downloaded from the Psychdata server and imported into SPSS—the Statistical Package for Social Sciences, Version 18.0 (Chicago, IL, www.spss.com). We ran descriptive statistics to summarize the demographic profile, behaviors, perceptions, and reported abuse among the sample. Chi-square tests were run to identify associations between individual characteristics and reported IPV victimization and perpetration. We dichotomized the variables race, education and age for the purpose of analyses due to insufficient numbers for each category.
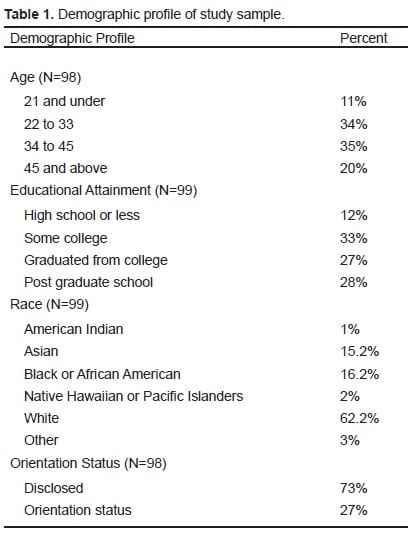
The PI was successful in obtaining 100 surveys within a 16-day data collection time frame. The age, race, disclosure status (disclosed v. non-disclosed), and educational attainment distribution of the sample is presented in Table 1. Sixty percent of the study sample believed IPV is a health issue among gay men in Atlanta, and 66% reported that they know other gay couples, currently or in the past, that involve IPV.
Respondents were asked to whom they would report being a victim of IPV and were allowed to select multiple categories. These categories included friends, family, police, professional counselor and other. Respondents were also given the option of selecting that there was no one to whom they would report abuse. The top 3 outlets in descending order, to whom respondents indicated they would report, were friends (n=55), family (n=37) and police (n=33). Only 12 respondents indicated that they would report abuse to a professional counselor and 5 selected “other.” Importantly, 27% of respondents indicated that they would not disclose abuse to anyone.
Substance Use
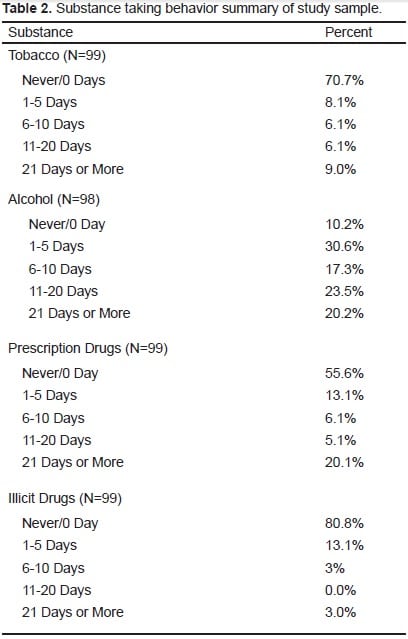
Respondents were asked about their substance use behavior within the past 30 days, which included tobacco, alcohol, prescription and illicit drugs. Table 2 presents a summary of findings related to substance use behaviors among the respondents.
Perpetration
The overall prevalence of perpetration among the study sample was 26.3%. Slightly over 18% of respondents indicated that they had physically harmed their intimate partner and 19% indicated that they had threatened to hurt their intimate partners with use of words, gestures, weapons or other means. Five percent of respondents reported they had forced their intimate partners to have sex.
Victimization
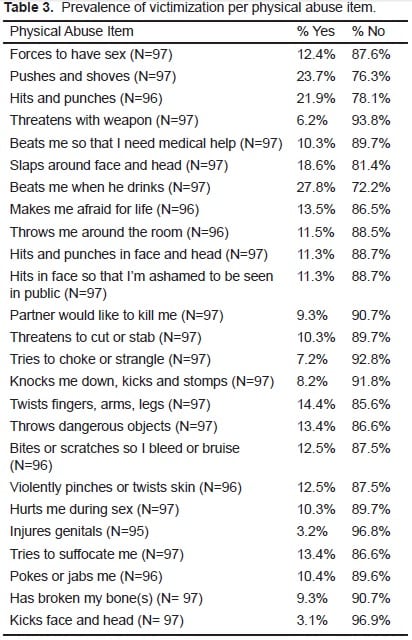
The overall prevalence of victimization among the study sample was 31%. The most commonly reported types of physical IPV reported by victims were “beats me when he drinks” (27.8%), “pushes and shoves me around violently” (23.7%), “hits and punches my arms and body” (21.9%), and “slaps me around my face and head” (22.8%). Table 3 presents the prevalence of victimization for each physical abuse item.
Severity of Victimization
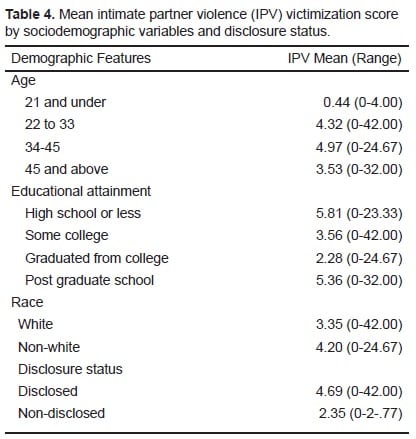
Table 4 presents the mean and range of the severity of IPV victimization scores by age, educational attainment, race, and disclosure status. The calculations of IPV scores are based on the WALMYR Assessment Scales where the higher the score (1–100) indicates more severe abuse.29
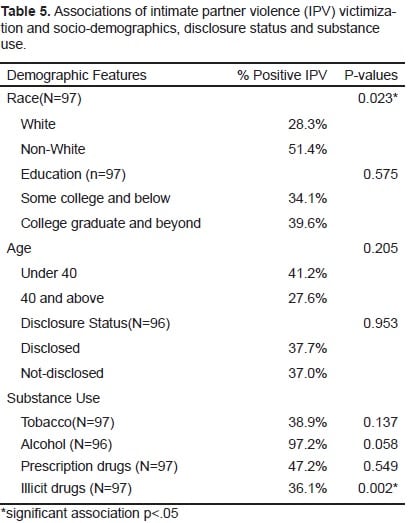
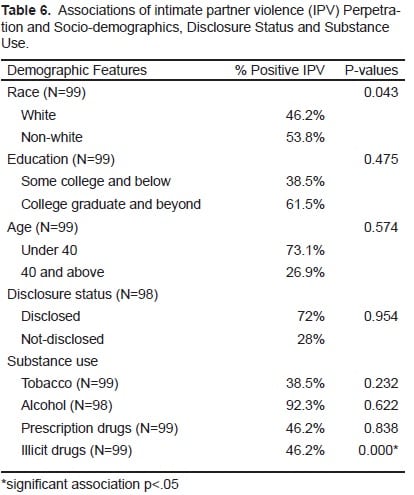
Associations of Victimization and Perpetration
We ran chi-square tests to identify associations between victimization and the following variables: race, education, age, disclosure status and substance use. Victimization was positively associated with illicit substance use (χ2 (1) = 9.923, p=0.002) and non-White race (χ2 (1) = 5.196, p=0.023). We also ran chi-square tests to identify associations between perpetration and race, education, age, disclosure status and substance use. Results indicated that perpetration was also positively associated with illicit substance use (χ2 (1) =16.528, p<0.01) and non-White race (χ2 (1) =4.088, p=0.043). Of the survey sample, 28.3% of Whites had experienced some form of IPV, as compared to 51.4% of non-Whites. Of perpetrators, 46.2% were White and 53.8% were non-White. Among victims of IPV, 36.1% reported illicit drug use while 46.2% of perpetrators reported using illicit drugs. We found no statistically significant associations with regard to age, education or disclosure status.
DISCUSSION
It is only within the last decade that violence prevention programs, specifically those that target the lesbian, gay, bisexual, transgender (LGBT) community, have begun to bring awareness to IPV-related issues. Gay IPV is particularly difficult to identify because of the social stigma associated with homosexuality. Although this study measured physical and sexual violence, other forms of abuse including psychological abuse and sexual coercion may also exist within our sampled population.
The overall prevalence of perpetration among the study sample was 26.3%, and victimization was 31%. Study results highlight significant associations between both race and illicit drug use, findings that may be useful in addressing this problem and reducing disparities in violence. As previously mentioned, this population experiences extreme forms of societal stress, and using substances is one mechanism of coping. These study findings align with the previous research that indicates substance abuse among the gay population is prevalent and linked to a range of unhealthy conditions, including violence.
IPV is a complex and multi-layered issue. This study clearly does not begin to understand the complexities surrounding it. Since this study focused primarily on physical violence, future research may expand upon psychological and sexual abuse or coercion among intimate partners. Unlike physical violence, which may be visible, psychological and sexual abuse or coercion may be more traumatic and less obvious. Psychological abuse can have long-term and short-term effects. Victims may not realize the damage of short-term abuse (believing he will change and disregarding any future occurrences) until long-term harm has been done (inability to form healthy relationships with someone else in the future). Further study should also measure the intensity of IPV. The duration and frequency of the episodes may provide additional insight to IPV dynamics. Additionally, qualitative research can provide greater depth of understanding to issues of gay IPV. For example, a person who identified himself as a victim may also be a perpetrator at another time. The perpetrator may have retaliated as a means of self-defense. The parties may have dual roles, but this can only be clarified with an interview. Formal interviews of former victims/perpetrators can provide a different perspective on why the episode occurred in the past.
IPV continues to be a major public health issue. Violence research in marginalized populations, such as in the LGBT community, lags behind IPV research focusing on heterosexual couples. Although this study used one of the most prominent social network websites, Facebook, it captures a mere fraction of the greater MSM population in Atlanta, Georgia. However, the finding that most participants agree that IPV is a real public health threat in the Atlanta gay community warrants further attention. More astoundingly, a majority of the participants knew other people engaged in IPV. Raising awareness and implementing evidence-based interventions will be key in addressing IPV within the gay community.
LIMITATIONS
This study used a snowball convenience sample and is therefore subject to selection bias. The ultimate research question about whether or not it would be feasible to recruit 100 participants from an underrepresented population via Facebook to provide data on a sensitive topic (IPV) was demonstrated. The ability to generalize these study results to a greater population of MSM is not possible, as the sample likely features characteristics that are different from the overall MSM population, such as generation issues and Internet access.
Results are further limited in that the sample represents only 100 individuals. While the size of the study sample is adequate for reasonable statistical testing of relationships between risk factors and IPV, a more sophisticated sampling methodology and larger sample size would enhance the study power. This pilot study reveals that there are patterns in the data that must be further explored. This pilot demonstrated the feasibility of recruiting study subjects (without any incentive for doing so) from the MSM population regarding IPV research.
A final limitation of this study is that all variables were based on self-reported data, possibly resulting in inaccuracies and skewing the reliability and validity of results. Due to the size of the respective samples, the analyses of race, age, and educational attainment were constrained to dichotomous variables. Although this study used a prominent social network website, it only captured a small portion of the population in Atlanta, Georgia. However, this methodology illustrated the role social networking can play as a viable recruitment technique. Our findings illustrate that IPV among gay males is a significant issue with far-reaching health implications and stresses the importance of assessing IPV when addressing other health issues. Our findings provide insight into IPV among a highly invisible and vulnerable population that suffers health disparities, lack of resources and equal protection under the law.
CONCLUSION
Despite the fact that IPV among gay male couples occurs at similar or higher rates than heterosexual couples, few studies have focused on abuse in same-sex male relationships. This lack of attention occurs despite mounting evidence that IPV among the gay male population poses a significant threat to short- and long-term health outcomes. Given the correlation found between illicit substance use and IPV, further research is needed to understand the rates, patterns, motivations, and contexts of substance use in order to develop strategies to prevent initiation and reduce ongoing use of these substances. Results from this study can help inform future research studies so that better screening and detection systems can be developed. It is likely that gay IPV victims will present in emergency department settings, but if front line staff are not aware of signs and factors that may be associated with IPV the cycle of violence will continue. It is imperative that public health researchers and healthcare providers collaborate in advancing the understanding of IPV within gay communities. It is an imperative associated with grave, yet preventable, health inequities.
Footnotes
Supervising Section Editor: Abigail Hankin, MD, MPH
Submission history: Submitted January 17, 2012; Revision received March 14, 2012; Accepted March 14, 2012
Reprints available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2012.3.11783
Address for Correspondence: Sheryl M Strasser, PhD, MPH, MSW
Georgia State University, Institute of Public Health, Atlanta, Georgia
Email: sstrasser@gsu.edu
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Stanley J, Bartholomew K, Taylor T, et al. Intimate violence in male same-sex relationships. Journal of Family Violence. 2006;21(1):31–41.
2. Brown C. Gender-role implications on same-sex intimate partner abuse. Journal of Family Violence.2008;23:457–462.
3. Houston E, McKirnan D. Intimate partner abuse among gay and bisexual men: risk correlates and health outcomes. Journal of Urban Health. 2007;84(5):681–690. [PMC free article] [PubMed]
4. Centers for Disease Control and Prevention Understanding intimate partner violence fact sheet. Available at: http://www.cdc.gov/violenceprevention/pdf/IPV_factsheeta.pdf. 2009. Accessed October 10, 2010.
5. World Health Organization Intimate Partner Violence Facts. Available at :http://www.who.int/violence_injury_prevention/violence/global_campaign/en/ipvfacts.pdf. 2002. Accessed October 12, 2010.
6. Tjaden P, Thoennes N. Full report of the prevalence, incidence, and consequences of violence against women. Washington, DC: National Center for Justice; 2000.
7. Peterman B, Dixon G. Intimate partner abuse between same sex partners: implication for counseling.Journal of Counseling and Development. 2003;81:40–59.
8. Tjaden P, Thoennes N. Extent, nature, and consequences of intimate partner violence: findings from the National Violence Against Women Survey. Washington (DC): Department of Justice (US); Publication No. NCJ 181867. 2000. www.ojp.usdoj.gov/nij/pubssum/181867.htm. Accessed October 12, 2010.
9. Bartholomew K, Regan KV, Oram D, et al. Correlates of partner abuse in male same-sex relationships. Violence and Victims. 2008;23(3):344–60. [PubMed]
10. Resnick HS, Acierno R, Kilpatrick DG. Health impact of interpersonal violence. 2: Medical and mental health outcomes. Behavioral Medicine. 1997 Summer;23(2):65–78. [PubMed]
11. Coker L, Davis E, Arias I, et al. Physical and mental health effects of intimate partner violence for men and women. American Journal of Preventive Medicine. 2002;23(4):260–268. [PubMed]
12. Elsberg M, Jansen HA, Heise L, et al. Intimate partner violence and women’s physical and mental health in the WHO multi-country study on women’s health and domestic violence: an observational study. Lancet. 2008 Apr 5;371(9619):1165–72. [PubMed]
13. Merrill GS, Wolfe VA. Battered gay men: an exploration of abuse, help seeking, and why they stay.Journal of Homosexuality. 2000;39(2):1–30. [PubMed]
14. McClennen C, Summers B, Vaughan C. Gay men’s domestic violence: dynamics, helpseeking behaviors, and correlates. Journal of Gay and Lesbian Social Services. 2002;14(1):23–49.
15. Greenwood L, Relf V, Huang B, et al. Battering victimization among a probability-based sample of men who have sex with men. American Journal of Public Health. 2002;92(12):1964–1969.[PMC free article] [PubMed]
16. Kurdek A. What do we know about gay and lesbian couples? Current Directions in Psychological Science. 2005;14:251–254.
17. Peplau L, Fingerhut A. The close relationships of lesbian and gay men. Annual Review of Psychology. 2007;58:405–424.
18. Stall R, Mills C, Williamson, et al. Association of co-occurring psychosocial health problems and increased vulnerability to HIV/AIDS among urban men who have sex with men. American Journal of Public Health. 2003;93(6):939–942. [PMC free article] [PubMed]
19. Welles SL, Corbin TJ, Rich JA, et al. Intimate partner violence among men having sex with men, women, or both: early-life sexual and physical abuse as antecedents. Journal of Community Health.2011 Jun;36(3):477–85. [PubMed]
20. Craft, Serovich Family-of origin factors and partner violence in the intimate relationships of gay men who are HIV positive. Journal of Interpersonal Violence. 2005;20(7):777–791. [PMC free article][PubMed]
21. Toro-Alfonso J, Rodriguez-Madera S. Domestic violence in Puerto Rican gay male couples: perceived prevalence, intergenerational violence, addictive behaviors, and conflict resolution skills. Journal of Interpersonal Violence. 2004;19:639. [PubMed]
22. Schilit L, Montagne M. Substance use as a correlate of violence in intimate lesbian relationships.Journal of Homosexuality. 1990;19:51–65. [PubMed]
23. Bradford J, Ryan C, Rothblum D. National lesbian health care survey: implications for mental health care. Journal of Consulting and Clinical Psychology. 1994;62:228–242. [PubMed]
24. Archer J. Male Violence. New York: Routledge; 1994. Power and male violence; pp. 310–332.
25. State & County QuickFacts: Atlanta, Georgia. US Bureau of the Census. Available at:http://quickfacts.census.gov/qfd/states/13/1304000.html. 2010. Accessed: November 22, 2010.
26. Gates G. About the gay index: Atlanta, Georgia. Urban Institute Research of Record. Available at:http://www.epodunk.com/cgi-bin/gayInfo.php?locIndex=7786. Accessed November 10, 2010.
27. Center for Positive Aging LGBT (Lesbian Gay Bisexual Transgender) Resources. Available at:http://www.centerforpositiveaging.org/LGBT.html.2010. Accessed: October 30, 2010.
28. Romero A, Rosky C, Badgett L, et al. Census Snapshop: Georgia. The Williams Institute, UCLA School of Law, UC Los Angeles. Available at: http://escholarship.org/uc/item/71r8t687.2008. Accessed: November 13, 2010.
29. Hudson W. The WALMYR Assessment Scales Scoring Manual. Tempe, AZ: WALMYR Publishing Co; 1992.