
{kind=link}
| Author | Affiliation |
|---|---|
| Christy L. Hopkins, MD | Department of Surgery, Division of Emergency Medicine, University of Utah School of Medicine, Salt Lake City, Utah |
| Troy Madsen, MD | Department of Surgery, Division of Emergency Medicine, University of Utah School of Medicine, Salt Lake City, Utah |
| Zachary Foy, MD | Department of Surgery, Division of Emergency Medicine, University of Utah School of Medicine, Salt Lake City, Utah |
| Michielle Reina, MS | Department of Surgery, Division of Emergency Medicine, University of Utah School of Medicine, Salt Lake City, Utah |
| Erik Barton, MD, MBA | Department of Surgery, Division of Emergency Medicine, University of Utah School of Medicine, Salt Lake City, Utah |
ABSTRACT
Introduction:
The purpose of this study was to examine the impact on emergency department (ED) length of stay (LOS) of a new protocol for intravenous (IV)-contrast only abdominal/pelvic computed tomography (ABCT) compared to historical controls.
Methods:
This was a retrospective case-controlled study performed at a single academic medical center. Patients ≥ 18 undergoing ABCT imaging for non-traumatic abdominal pain were included in the study. We compared ED LOS between historical controls undergoing ABCT imaging with PO/IV contrast and study patients undergoing an IV-contrast-only protocol. Imaging indications were the same for both groups and included patients with clinical suspicion for appendicitis, diverticulitis, small bowel obstruction, or perforation. We identified all patients from the hospital’s electronic storehouse (imaging code, ordering department, imaging times), and we abstracted ED LOS and disposition from electronic medical records.
Results:
Two hundred and eleven patients who underwent PO/IV ABCT prep were compared to 184 patients undergoing IV-contrast only ABCT prep. ED LOS was shorter for patients imaged with the IV-contrast only protocol (4:35 hrs vs. 6:39 hrs, p < 0.0001).
Conclusion:
Implementation of an IV-contrast only ABCT prep for select ED patients presenting for evaluation of acute abdominal pain significantly decreased ED LOS.
INTRODUCTION
Abdominal pain is one of the most common presenting complaints to United States emergency departments (ED), comprising up to 6.5% of all presenting complaints.1 The use of computed tomography (CT) is common in the initial evaluation of patients with abdominal pain acutely presenting to the ED in order to rule out intra-abdominal pathology.
Several improvements in CT imaging technology have transpired, including more rapid image acquisition, which is now possible with helical scanning, and multi-detector CTs. The rapid image acquisition limits the artifact seen from respiratory and peristaltic motion, decreasing the amount of image degradation noted with earlier generation scanners.2
Due to these recent advances in imaging, there is a growing body of literature which suggests that oral contrast does not improve the accuracy of CTAB scans when evaluating patients with CT for appendicitis2–4,5–9 or other common disorders like diverticulitis and small bowel obstruction (SBO).10,11 The use of intravenous (IV) contrast alone is typically easier for patients to tolerate than PO contrasted exams. In addition, IV-contrast only exams do not require the protracted preparation time associated with many IV/PO contrast protocols. The use of IV contrast may increase the sensitivity for diagnosis of appendicitis and recognition of the complications of common causes of abdominal pain, such as bowel ischemia, when compared to non-contrast enhanced CTs.12–14
ED length of stay (LOS) times have been documented to be as much as 60 minutes shorter with alternate bowel preps (i.e. rectal),15 and 240 minutes shorter for unenhanced CT.16The impact of ED LOS for IV-contrast only CT exams was examined in one study to date, which showed a median decrease of ED LOS of 30 minutes for patients with undifferentiated abdominal pain.17
The objective of this study was to quantify the impact of a new IV-contrast only CT protocol on ED LOS as compared to historical controls receiving both IV/PO contrasted studies for a select group of patients clinically suspected of having appendicitis, diverticulitis, SBO or intra-abdominal free air.
METHODS
This study was performed at the University of Utah Medical Center ED, an academic emergency department with an annual census of 38,000, and an emergency medicine residency training program. All attending physicians working in this department were board-certified/prepared by the American Board of Emergency Medicine during the study period. The study was approved by the hospital’s institutional review board. The institution initiated a new CT protocol in which IV-contrast only exams were approved for use in ED patients with a high clinical suspicion for appendicitis, SBO, diverticulitis, or free air. Previously, the IV-contrast only study had been used solely for patients undergoing evaluation for traumatic injuries. Historically, all evaluations for non-traumatic abdominal pain had been evaluated using both PO and IV contrasted exams, unless contraindications to contrast material existed.
During the study period, abdominal scanning was performed using a 128-Multidectector CT scanner (Siemens Definition 128). Portal venous phase CT images were acquired from the diaphragm to the greater trochanters with the following parameters: slice thickness, 5 mm; reconstruction interval, 5 mm; pitch, 1.0; noise factor, 19 (Care Dose modulation); and rotation time, 1 second. The direct multiplanar reformation function was used to generate coronal reformations with a slice thickness of 3 mm and a reconstruction interval of 3 mm. All patients received 140 mL of Isovue (Optiray 300 mg I/mL, Mallinckrodt Imaging) administered via power injection through an IV cannula located in an antecubital or hand vein at a rate of 3 mL/s. A dual-syringe power injector (Stellant CT Injection System, Medrad) was used to administer a 50-mL normal saline chasing bolus immediately after the injection of IV contrast material. The saline bolus was injected at 3 mL/s. The acquisition of portal venous phase images started 70 seconds after the initiation of the injection of IV contrast material. At the study institution, oral contrast was administered for 90 minutes with barium sulfate oral contrast bowel prep (900 mL of 2.2% barium sulfate suspension [Medescan barium sulfate, Lafayette Pharmaceuticals]).
The IV-contrast only abdominal/pelvic computed tomography (ABCT) protocol, initiated in November 2008, was suggested for patients with a clinical history and physical exam suggestive of appendicitis, diverticulitis, SBO, or intra-abdominal free air. In contrast, an ABCT with IV/PO contrast was recommended for patients who did not meet the IV-only protocol indications (for example, those patients with conditions or presenting complaints of undifferentiated abdominal pain, post-operative imaging, or patients with complex underlying medical issues). We did not include imaging performed for the evaluation of traumatic injuries in the data analysis. We also excluded pregnant patients and patients under the age of 18 from the study.
The study group consisted of all consecutive IV-contrast only ABCT scans specifically performed to evaluate patients for acute appendicitis, diverticulitis, SBO, or free air (February 2009 through May 2009). We used historical controls from a period pre-dating the implementation of the new IV-contrast only CT protocol (April 2008 through September 2008). Only patients whose indications for CT were similar to the study patients (acute appendicitis, diverticulitis, SBO, or free air) were chosen for historical controls.
We identified cases using the hospital’s electronic data storehouse, which records the date, patient visit number, ordering physician, ordering department, radiology study code, the order indication, and the radiology read turnaround time (TAT) for all imaging requests in the hospital. We downloaded all data into an Excel 2008 spreadsheet, version 12.2.3 (Microsoft, Redmond, CA).
Chart review was performed by an emergency medicine resident (ZF) and a trained medical student (MR) using a standardized abstraction form with standard definitions for all variables. Both were familiar with the electronic medical system, and abstractors were trained beforehand in data abstraction methods and data interpretation. The principal investigator provided regular feedback to the data abstractors regarding any errors or discrepancies in data collection. The abstractors were aware of the general aims of the study (the evaluation of pre- and post-CT protocol changes) but were not aware of the specific hypotheses to be evaluated in the study. One data abstractor performed review on all of the charts from the period prior to implementation of the protocol, while the other performed data review on all the charts from the period after the protocol implementation. Quality assurance review of the data was performed on 10% of the charts by the principal investigator (CH), with a kappa score of 0.976.
We abstracted ED length of stay (LOS) from ED charts and defined LOS as the interval between the time the patient was placed in an ED room until the time the patient was physically discharged from the ED (to home, to the operating room, to an inpatient unit, or to the ED observation unit [EDOBS]). These times were abstracted from the ED nursing flow sheet, which specifically details both of these times. The indication for exam and patient disposition (home, operating room, EDOBS, or admission) was abstracted from the ED physician electronic medical record (EMR). We identified radiology-read TAT as the interval between the time from completion of imaging to the time a preliminary read was electronically available. Radiological interpretation was abstracted from the hospital’s EMR as were surgical pathology results, when available.
We analyzed the data using chi-square and Mann-Whitney U test (SPSS v. 15.0, SPSS Inc., Chicago, IL) to compare ED LOS, time from completion of imaging to time radiology report available to the provider, and baseline patient characteristics between the two patient groups.
RESULTS
Of the 590 ABCT exams performed during the four-month (February 2009 through May 2009) post protocol study period for the evaluation of non-traumatic abdominal pain, 348 were performed with IV and PO contrast, and 242 were performed with IV-contrast only. One hundred and eighty-four of the IV-contrast only exams were specifically performed to evaluate for acute appendicitis, diverticulitis, SBO, or free air.
A total of 467 ABCT exams were performed for non-traumatic abdominal pain during the 6 month historical control period (April 2008 to September 2008). Of these, 211 ABCTs were performed to specifically evaluate for acute appendicitis, diverticulitis, SBO, or free air.
Baseline characteristics for both groups are shown in Table 1. The patients in the IV-contrast only group were a median of 4 years younger when compared to the historical control group. Gender distribution was similar between the groups. During the study period, the average number of ED patient visits per day was, on average, 2 patients per day more for the IV-contrast only group (105 pts/day vs. 107 pts/day). Both groups had a similar distribution for the four main study indications. The rescan rate between the two groups was also similar. Prior to the implementation of the new protocol, the ABCT rate was 5.8 ABCT/100 patients. The rate post protocol implementation was 6.7 ABCT/100 patients.
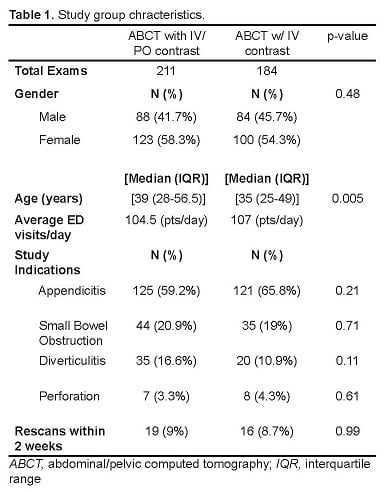
Study group chracteristics.
The total ED LOS was significantly shorter for patients in the IV-contrast only group. The median ED LOS for those in the IV-contrast only group was 4:35 hours, while average ED LOS for the IV/PO group was 6:39 hours, (p<0.0001). We observed the shorter LOS in patients discharged to home, as well as in patients taken directly to the OR, or admitted to the hospital (Table 2). The radiology-read TAT was not significantly different between the two groups (Table 2). The median time from test scheduled to time the test was completed was 126 minutes for studies with PO/IV contrast and 52 minutes for studies with IV-contrast only (a difference of 74 minutes).
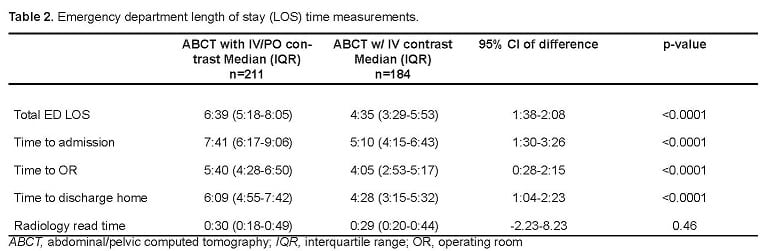
Emergency department length of stay (LOS) time measurements.
In the IV-contrast only group, 100 of the 184 patients (54.3%) scanned had a new abnormality by CT. Forty-three (23.4%) patients had an exam that revealed an alternative diagnosis other than the clinical indication recorded for the exam, and 82 (44.6%) had exams that were normal or showed no new changes. Of the remaining patients, one had a missed appendicitis (diagnosed 2 days later), and one was diagnosed with chronic appendicitis by CT (observed in the hospital, then sent home).
In the control group (IV/PO contrast), 141 (66.8%) patients had a new abnormality by CT. Fifty-seven (27%) had an exam that revealed an alternative diagnosis other than the clinical indication recorded for the exam, and 70 patients (33.2%) had studies that were normal or showed no new changes. Three patients diagnosed with acute appendicitis by CT were observed and discharged home by surgery without going to the operating room (OR); a fourth patient with appendicitis by CT was taken to the OR and had no appendicitis by pathology.
Rescan Rate
Rescan rates were comparable between the IV-contrast only and the IV/PO groups. In the IV-contrast only group, 16 (8.7%) patients were rescanned within two weeks of their original CT imaging. Of these patients, 12 were rescanned during their inpatient hospitalization. Eight of the admitted patients had either post-operative exams (5 patients), or a follow-up inpatient exam (3 patients). One patient had repeat imaging with oral contrast the same day as their initial evaluation, which did not change the original CT finding (early appendicitis). Three patients were discharged from an inpatient hospitalization, and then re-presented to the ED and had another CT performed (none had a change in the initial diagnosis).
Four patients were discharged home from the ED and were rescanned within two weeks of discharge. Three of the 4 had no change in the original diagnosis. The last patient had an initial CT read as normal (appendix was not visualized) and had a repeat scan (with oral contrast) 2 days later that showed an acute appendicitis.
Nineteen (9.0%) patients in the control group were rescanned within two weeks of their original scan. Of these, 16 were rescanned during their inpatient hospitalization (10 patients had post-operative exams and 6 patients had follow-up inpatient exams). Three patients were discharged home from the ED and then re-scanned within two weeks of discharge. There was no change in the original diagnosis on the second scan for any of the patients.
DISCUSSION
The use of IV-contrast only for the evaluation of patients presenting to the ED with abdominal pain has been shown to have a high sensitivity and specificity for the diagnosis of common causes of acute abdominal pain, such as acute appendicitis, diverticulitis, and SBO.7,10 One previous study showed a decreased ED LOS for those patients undergoing ABCT with IV-contrast only for undifferentiated abdominal pain, with a median ED LOS decrease of 30 minutes.17
In our series, the use of an IV-contrast only protocol for patients with a high clinical suspicion of appendicitis, diverticulitis, SBO or free air significantly decreased ED LOS. This held true not only for patients discharged home from the ED, but also for those requiring surgery or admission. The impact of limiting PO contrast in such patients not only decreased ED LOS, but also allowed for earlier consultation and definitive treatment for patients with identified pathology, with over 2 hours in time saved for patients requiring operative interventions. In addition, the re-scan rate for patients undergoing the IV-contrast only protocol did not change significantly when compared to historical controls.
In our study, the time test ordered to time test completed was a median of 72 minutes shorter for patients undergoing the IV-contrast only protocol. It would be expected that the decrease in ED LOS would approximate the time saved by not using oral contrast. The additional time saved may have been due to the fact that the patients selected to undergo the IV-contrast only imaging presented with a more straightforward clinical picture, and/or were younger with less complicating medical factors. It is also possible that the addition of a faster CT protocol may have reduced the threshold to order such testing, which may result in testing patients with a lower pre-test probability of disease.
LIMITATIONS
This study had several limitations. Retrospective data abstraction is limited to that which is recorded in the medical record and is subject to additional limitations due to the process of chart abstraction and data interpretation. However, an independent evaluation of 10% of the study patients revealed excellent agreement in abstracted study data (kappa = 0.97).
The patients in the IV-contrast group were, on average, five years younger than the historical control group and had less pathology detected on imaging overall. It is possible that the decreased ED LOS was not only influenced by the decreased prep time for oral contrast; additionally, this imaging may have been preferentially used in patients with straightforward clinical presentations and/or less underlying clinical pathology.
The study institution did see an increase in total ABCT ordered (approximately 1 additional scan/100 patients) post implementation of the new protocol. It is unlikely that this increased volume impacted the total ED LOS for all ED patients; however; we did not specifically measure this in the study. The addition of a faster ABCT protocol may have also lowered the threshold to image patients with a lower pre-test probability of disease.
In our study, the decision of what type of imaging to order was left to the discretion of the treating physician in the ED. Due to the retrospective nature of this study it was difficult to determine which patients may not have met the indications of the IV-contrast only protocol (protocol violations). It is possible that some of the patients who received the IV-contrast only ABCT protocol did not receive oral contrast due to patient inability to tolerate oral contrast, time constraints, or unfamiliarity with the protocol indications.
This study was performed at a single center. Some of the patients initially evaluated and imaged at our institution could have been re-evaluated or re-imaged at another facility, thus affecting the reported re-scan rate noted in our study. No attempt was made to determine if patients went to another facility for follow-up. This limits the quality of the re-scan rates reported in this study.
CONCLUSION
Initiation of an IV-contrast only protocol for select ED patients decreased the patients overall ED LOS by approximately 2 hours.
Footnotes
Supervising Section Editor: Michael Menchine, MD, MPH
Submission history: Submitted March 21, 2011; Revision received September 1, 2011; Accepted December 15, 2011
Full text available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2011.12.6748
Address for Correspondence: Christy Hopkins, MD, Department of Surgery, Division of Emergency Medicine, University Health Care, 150 North Medical Drive, Room 1C026, Salt Lake City, UT 84132
Email: Christy.mccowan@hsc.utah.edu
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Centers for Disease Control and Prevention CDC releases latest data on emergency department visits. Available from:http://www.cdc.gov/nchs/pressroom/04facts/emergencydept.htm. Accessed April 5, 2010.
2. Hlibczuk V, Dattaro JA, Jin Z, et al. Diagnostic Accuracy of Noncontrast Computed Tomography for Appendicitis in Adults: A Systematic Review. Ann Emerg Med.2010;55:51–59. [PubMed]
3. Anderson B, Salem L, Flum D. A systematic review of whether oral contrast is necessary for the computed tomography diagnosis of appendicitis in adults. Am J Surg.2005;190:474–478. [PubMed]
4. Ege G, Akman H, Sahin A, et al. Diagnostic value of unenhanced helical CT in adult patients with suspected acute appendicitis. Br J Radio.l. 2002;75:721–725.
5. in’t Hof KH, van Lankeren W, Krestin GP, et al. Surgical validation of unenhanced helical computed tomography in acute appendicitis. Br J Surg. 2004;91:1641–1645.[PubMed]
6. Lane MJ, Liu DM, Huynh MD, et al. Suspected acute appendicitis: nonenhanced helical CT in 300 consecutive patients. Radiology. 1999;213:341–346. [PubMed]
7. Mun S, Ernst RD, Chen K, et al. Rapid CT diagnosis of acute appendicitis with IV contrast material. Emerg Radiol. 2006;12:99–102. [PubMed]
8. Stacher R, Portugaller H, Preidler KW, et al. Acute appendicitis in non-contrast spiral CT: a diagnostic luxury or benefit? Rofo. 1999;171:26–31. [PubMed]
9. Tamburrini S, Brunetti A, Brown M, et al. Acute appendicitis: diagnostic value of nonenhanced CT with selective use of contrast in routine clinical settings. Eur Radiol.2006;17:2055–2061. [PubMed]
10. Anderson SW, Soto JA, Lucey BC, et al. Abdominal 64-MDCT for Suspected Appendicitis: The Use of Oral and IV Contrast Material Versus IV Contrast Material Only.Am J Roentgenol. 2009;193:1282–1288. [PubMed]
11. Lee SY, Coughlin B, Wolfe JM, et al. Prospective comparison of helical CT of the abdomen and pelvis without and with oral contrast in assessing acute abdominal pain in adult Emergency Department patients. Emerg Radiol. 2006;12:150–157. [PubMed]
12. Jacobs JE, Birnbaum BA, Macari M, et al. Acute appendicitis: comparison of helical CT diagnosis focused technique with oral contrast material versus nonfocused technique with oral and intravenous contrast material. Radiology. 2001;220:683–690. [PubMed]
13. Chou CK, Wu RH, Mak C, et al. Clinical significance of poor CT enhancement of the thickened small-bowel wall in patients with acute abdominal pain. Am J Roentgenol.2006;186:491–498. [PubMed]
14. Sheedy SP, Earnest F, Fletcher JG, et al. CT of small-bowel ischemia associated with obstruction in emergency department patients: diagnostic performance evaluation.Radiology. 2006;241:729–736. [PubMed]
15. Berg ER, Mehta SD, Mitchell P, et al. Length of stay by route of contrast administration for diagnosis of appendicitis by computed-tomography scan. Acad Emerg Med.2006;13:1040–1045. [PubMed]
16. Huynh LN, Coughlin BF, Wolfe J, et al. Patient encounter time intervals in the evaluation of emergency department patients requiring abdominopelvic CT: oral contrast versus no contrast. Emerg Radiol. 2004;10:310–313. [PubMed]
17. Jeremiah D, Schuur JD, Grant C, Sucov A. Effect of oral contrast for abdominal computed tomography on emergency department length of stay. Emerg Radiol.2010;17:267–273. [PubMed]