
{kind=link}
| Author | Affiliation |
|---|---|
| Thomas M. Nappe, DO | Lehigh Valley Hospital, Department of Emergency Medicine, Allentown, Pennsylvania |
| Shawn M. Quinn, DO | Lehigh Valley Hospital, Department of Emergency Medicine, Allentown, Pennsylvania |
An 18-year-old female presented to the emergency department with three days of worsening left flank pain. Past medical history included asymptomatic bacteriuria. She denied prior similar episodes or inciting events, and was currently being treated with trimethoprim sulfamethoxazole by an urgent care center for a urinary tract infection, although she denied having any urinary symptoms. Upon evaluation, she was found to be in severe pain, refractory to multiple doses of opioids. Her examination revealed fever, mild tachycardia and tachypnea, and clear lungs, with significant tenderness to palpation on her left flank. Initial laboratory evaluation showed a leukocytosis and bacteriuria.
A computed tomography of the abdomen and pelvis was ordered with intravenous contrast to rule out pyelonephritis and infected renal calculus. It revealed Figure 1, which shows an inflamed pulmonary sequestration in the posteromedial left lung base, with a surrounding pleural effusion. An independent arterial blood supply branching off of the descending thoracic aorta was later confirmed with angiography, shown in Figure 2, which further revealed infarction secondary to torsion.

Figure 1. Computed tomography image of thorax with pulmonary sequestration present at left base.
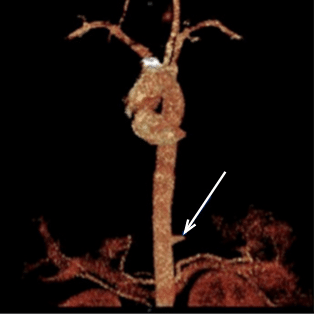
Figure 2. Angiography showing arterial blood supply to pulmonary sequestration with abrupt lack of flow due to torsion.
A pulmonary sequestration is a congenital malformation of independent, nonfunctioning, pulmonary tissue that does not communicate with the tracheobronchial tree and often has its own independent systemic blood supply.1-4 Both the location and associated effusion in this image indicate an extralobular pulmonary sequestration, which is defined by the presence of its own pleura.1,2,5 Presentation can occur at various ages and can include recurrent pneumonia, hemoptysis and pain, and persistent or severe symptoms may indicate surgical resection.5,6
Footnotes
Section Editor: Sean O. Henderson, MD
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Lehigh Valley Health Network, LVH-M-5th floor EM Residency Suite, 2545 Schoenersville Rd., Bethlehem, PA 18017. Email: Thoms_M.Nappe@LVHN.org. 3 / 2015; 16:314 – 315
Submission history: Revision received December 16, 2014; Accepted January 13, 2015
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Azizkhan RG, Cromblehome TM. Congenital cystic lung disease: contemporary antenatal and postnatal management. Pediatr Surg Int. 2008;24:643-57.
2. Nakamura CT. Pulmonary sequestration. Radiology Cases in Ped Emerg Med. 1996;5. Avaiable at: https://www.hawaii.edu/medicine/pediatrics/pemxray/v5c14.html.
3. Platon A, Poletti PA. Images in clinical medicine. Pulmonary sequestration. N Eng J Med. 2005;353:e18.
4. Gupta S, Kim S. Images in clinical medicine. Pulmonary sequestration. N Eng J Med. 2013;368:e6.
5. Ruan SY, Yang CY, Yu CJ. Cystic form of pulmonary sequestration. CMAJ. 2011;183:1050.
6. Conran RM, Stocker JT. Extralobar sequestration with frequently associated congenital cystic adenomatoid malformation, type 2: report of 50 cases. Pediatr Dev Pathol. 1999(2):454-63.
{kind=link}