
{kind=link}
| Author | Affiliation |
| George Lim, MD | Icahn School of Medicine at Mount Sinai, Department of Emergency Medicine, New York, New York |
| Braden Hexom, MD | Icahn School of Medicine at Mount Sinai, Department of Emergency Medicine, New York, New York |
A 38 year old obese female presented to the emergency department with 1 hour of nausea and blue colored urine. She endorsed recent flatus and bowel movement but denied abdominal pain, dysuria, fevers, or toxic ingestions. She presented a urine cup on arrival with obviously blue tinged urine (Figure). Her exam revealed a comfortable appearing female with no abdominal or costovertebral tenderness. She reported having an OrberaTM intragastric balloon placement 15 months prior in Brazil (Apollo Endosurgery, Inc., Austin, TX). The patient was admitted to the hospital for urgent endoscopic retrieval. However, as the device is not approved for use in the U.S., attempts to find a local physician familiar with the procedure or the appropriate retrieval equipment were unsuccessful. Open surgical removal was offered to the patient, who declined and instead returned to Brazil for removal there. The patient was lost to follow up.
DISCUSSION
Obesity is a prevalent disease with treatment options including diet, behavioral modification, medication and surgery. Patients, who are not candidates for more traditional bariatric surgeries may benefit from endoscopically placed intragastric balloons (IGB).1 Once in the stomach, the balloon is filled with 500-700mL of saline and 10mL of methylene blue (to identify leakage or rupture). The balloon displaces stomach volume which produces a sense of early satiety when eating.2 Severe adverse complications include gastric perforation (more likely in those with previous upper GI surgeries), gastric obstruction, gastric ulcer, esophagitis, and esophageal perforation.3 IGBs are only designed to remain in the stomach for a maximum of 6 months, while this patient had her device for several more months than is recommended. Increased balloon rupture and displacement with occasional intestinal obstruction are associated with patients who retain IGBs for more than 6 months.4 Treatment for ruptured and displaced IGBs is endoscopic retrieval using proprietary equipment, or possible laparotomy.
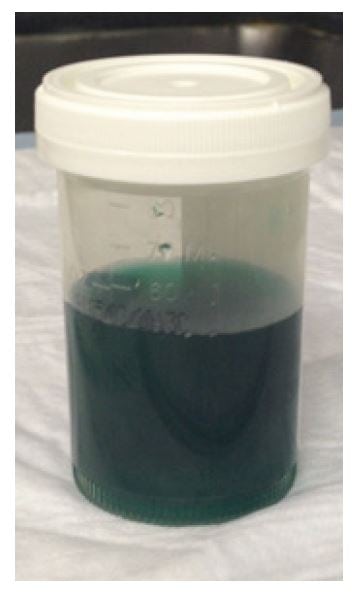
Figure. Patient’s blue urine after intragastric balloon rupture.
Footnotes
Supervising Section Editor: Sean O. Henderson, MD
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: George Lim, MD, Mount Sinai Medical Center, Dept. of Emergency Medicine, 1 Gustave L. Place, Box 1149, New York, NY 10029. Email: georgelim3@gmail.com.
Submission history: Submitted August 18, 2014; Accepted August 28, 2014
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
- Nijhof HW, Steenvoorde P, Tollenaar RA. Perforation of the esophagus caused by the insertion of an intragastric balloon for the treatment of obesity. Obes Surg. 2006;16(5):667-70.
- Genco A, Bruni T, Doldi SB, et al. BioEnterics Intragastric Balloon: The Italian Experience with 2,515 Patients. Obes Surg. 2005;15(8):1161-4.
- Koutelidakis I, Dragoumis D, Papaziogas B, et al. Gastric perforation and death after the insertion of an intragastric balloon. Obes Surg. 2009;19(3):393-6.
- Evans JD, Scott MH. Intragastric balloon in the treatment of patients with morbid obesity. Br J Surg. 2001;88(9):1245-8.