
{kind=link}
| Author | Affiliation |
|---|---|
| Linda Joseph, MD | St. Luke’s University Hospital and Health Network, Bethlehem, Pennsylvania |
| Rebecca K. Jeanmonod, MD | St. Luke’s University Hospital and Health Network, Bethlehem, Pennsylvania |
ABSTRACT
Deep sternal wound infections (DSWI) are infections of the sternum, mediastinum, or the muscle, fascia and soft tissue that overlie the sternum, typically occurring within a month of cardiac surgery. They are infrequent though severe complications of cardiac surgery. Diagnosis is made by the clinical presentation of fever, chest pain, or sternal instability in the setting of wound drainage, positive wound cultures, or chest radiographic findings. We describe the case of an elderly man presenting 6 months after cardiac surgery with DSWI. Due to the atypical nature of such a late presentation, definitive therapy was delayed. Given a severely ill patient with multiple risk factors for poor wound healing, the clinician must maintain a high index of suspicion for DSWI despite a delayed presentation.
A 77-year-old male presented to the emergency department (ED) with 4 days of worsening substernal chest pain radiating to the left shoulder. The patient reported a growing mass at the superior aspect of his sternum, which was first noted several months earlier as “a small lump,” but had been increasing in size over the preceding week. Review of systems was otherwise negative.
The patient’s medical history was significant for aortic valve replacement (AVR) 6 months prior with an associated chronic pericardial effusion. He additionally had hypertension, peripheral vascular disease, non-insulin dependent diabetes mellitus, chronic foot ulcers, cirrhosis, chronic renal insufficiency, and chronic obstructive pulmonary disease (COPD) on steroid therapy.
On examination, the patient was afebrile, tachycardic at 112 with a blood pressure of 96/60 mmHg. His heart was irregularly irregular with no murmurs. He had a tender crepitant fluctuant soft tissue mass at the sternal notch, superior to a healed sternotomy scar, which extended into the anterior neck. Remainder of exam was unremarkable.
Laboratory findings were remarkable for a white blood cell count of 6.43×103/uL with 20% bands, chronic thrombocytopenia of 45×103/uL, and acute on chronic renal insufficiency.
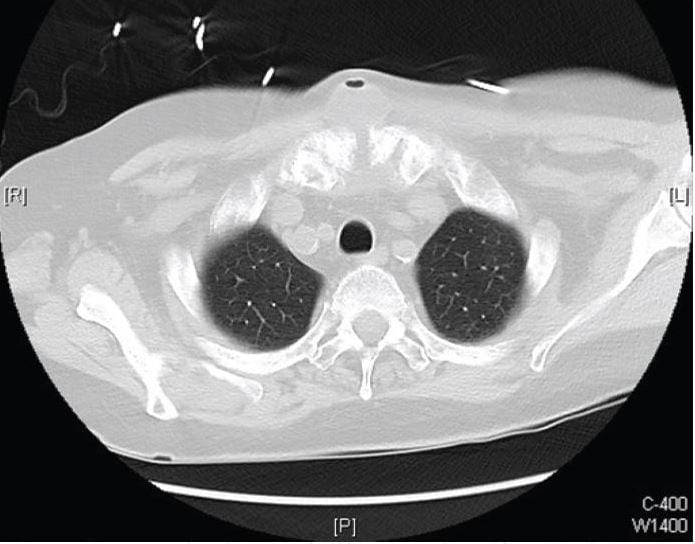
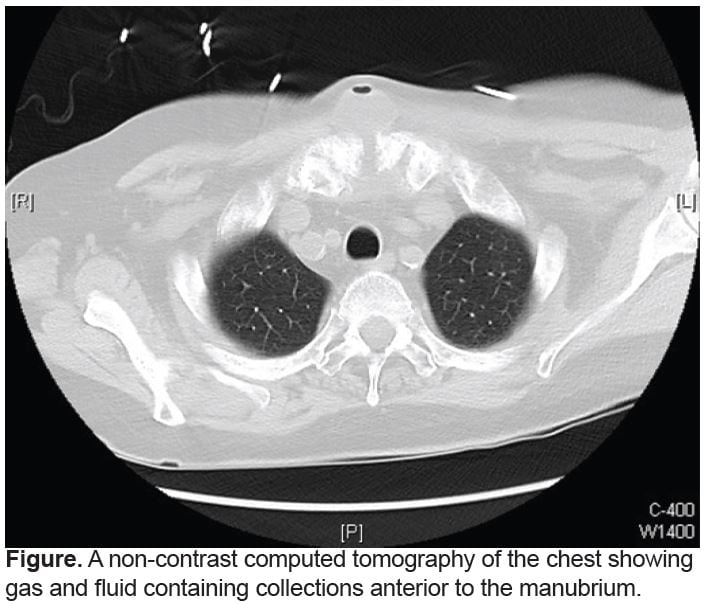
Bedside ultrasound demonstrated areas of discrete fluid collection in the suprasternal mass. Bedside echocardiogram showed normal ejection fraction, normal function of the bioprosthetic aortic valve, no valvular vegetations, and a moderate pericardial effusion similar to past studies. A non-contrast computed tomography of the chest showed gas and fluid containing collections anterior to the manubrium (Figure).
{kind=link}
Broad-spectrum antibiotics were started for sepsis, and cardiology and cardiothoracic surgery were consulted. They felt the fluid collection was unlikely infectious in etiology since the patient’s AVR took place 6 months prior to presentation. The patient was admitted for sepsis with the medical team identifying a likely source as a toe ulcer with cellulitis.
During a 3-week hospital course, the patient was found to have methicillin sensitive Staphylococcus aureus bacteremia and remained on parenteral antibiotics. After failing to improve, the sternal mass was aspirated and grew out the same pathogen. He underwent operative sternal wound drainage, debridement, and wound VAC placement. DSWI was confirmed by sternal biopsy and wound culture. After a protracted hospital course, the patient was transported to a long-term care facility. Over the course of several weeks, the sternal wound healed without need for reconstructive surgery.
DISCUSSION
Although uncommon, sternal wound infections are potentially life-threatening complications of cardiac surgery. They are associated with prolonged hospitalizations, increased cost of care, significant morbidity and increased short- and long-term mortality.1,2 Sternal wound infections are described as either superficial, involving only the skin and subcutaneous tissue, or deep, involving the underlying muscle, fascia, bone (sternum), and body spaces (mediastinum).3,4 According to the Centers for Disease Control and Prevention (CDC), DSWI, (osteomyelitis and mediastinitus), are diagnosed by meeting one of the following criteria:
- Positive cultures from mediastinal tissue or fluid obtained during an invasive procedure.
- Evidence of mediastinitis seen during an invasive procedure or histopathologic examination.
- At least 1 of the following signs or symptoms: fever (>38°C), chest pain, or sternal instability and at least 1 of the following:
- Purulent discharge from mediastinal area.
- Organisms cultured from blood or discharge from mediastinal area.
- Mediastinal widening on imaging test.5
The reported incidence of deep sternal wound infections (DSWI) after sternotomy ranges from 0.22% – 4%2–4,6–8 with mortality rates ranging from 9.7% – 23.5%.2,3,7 Risnes et al.9 demonstrated that the risk of death following DSWI remains higher than in uninfected controls for up to 10 years.
Although most literature reports that the mean interval between initial cardiac surgery and diagnosis of DSWI is about 14 days, there have been cases of delayed presentations of DSWI. Sakamoto et al7 conducted a retrospective analysis of 863 patients who underwent cardiac surgery and found the mean interval to be 23.6 +/− 16.0 days, with intervals ranging from 7 to 51 days. Bor et al10 described the time from initial cardiac surgery to diagnosis of DSWI as ranging from 3 to 417 days after surgery, with a median of 7 days and 67% of patients presenting within 14 days.
There are several well-cited preoperative, operative, and postoperative risk factors for DSWI. Preoperative factors include advanced age, diabetes, male gender, COPD, obesity, hypertension, peripheral vascular disease, cigarette smoking, need for preoperative use of intra-aortic balloon pump, and preoperative use of inotropes.3,7,11 These factors contribute to poor wound healing and wound dehiscence. They also reflect the general poor health and compromised immune system of the patient population undergoing sternotomy and cardiac surgery. Operative factors include emergent operations, coronary artery bypass grafting (CABG), bilateral internal thoracic artery use, use of inotropic agents, prolonged operation time (> 5–8hrs), blood transfusions, combined CABG and valve or aortic surgery. Postoperative factors include use of postoperative IABP, re-exploration, postoperative hyperglycemia, prolonged placement of drainage tubes and prolonged intensive care unit stays.7
DSWI should be suspected in the setting of known sternotomy with a clinical presentation of fever, chest pain, sternal instability, systemic toxicity, or wound drainage. As per CDC guidelines, diagnosis is eventually confirmed by these symptoms in the setting of a widened mediastinum on chest radiograph, presence of fluid drainage, or positive blood or wound cultures.5 Given significant morbidity and mortality, patients with suspected DSWI presenting to the ED should be immediately started on broad-spectrum antibiotics with eventual narrowing of coverage based on wound culture. In the setting of a severally ill patient with signs and symptoms of DSWI, DSWI should not be excluded on the basis of time course alone. Most patients should be taken to the operating room urgently for wound exploration and debridement of nonviable or infected tissue.12 Afterwards, based upon the severity of the patient’s illness and operative findings, the sternum can be closed immediately or after a period of open wound management. Some patients will require reconstructive surgery with muscular flaps to achieve adequate wound closure and healing.7,12
CONCLUSION
DSWI typically presents within a few weeks, but can present remotely from cardiac surgery. In an ill-appearing patient with a history of compromised immune system, frequent skin infections, and poor wound healing, DSWI should remain high on the differential, even if cardiac surgery occurred several months prior to presentation. Antibiotics should be started as soon as possible and surgical consultation should be acquired for emergent operative wound exploration, drainage, debridement, and closure.
Footnotes
Address for Correspondence: Linda Joseph, MD, St. Luke’s University Hospital 801 Ostrum St. Bethlehem, PA 18015, Email: Linda.Joseph@sluhn.org 3 / 2014; 15:134 – 136
Submission history: Revision received August 21, 2013; Accepted November 12, 2013
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Toumpoulis IK, Anagnostopoulos CE, DeRose JJ. Impact of deep sternal wound infection on long term survival after coronary artery bypass grafting. Chest. 2005;127:464-471.
2. Filsoufi F, Castillo JG, Rahmanian PB, et al. Epidemiology of deep sternal wound infection in cardiac surgery. J Cardiothorac Vasc Anesth. 2009;23(4):488-494.
3. Omran AS, Karimi A, Ahmadi SH, et al. Superficial and deep sternal wound infection after more than 9000 coronary artery bypass graft (CABG): incidence, risk factors and mortality. BMC Infection Diseases. 2007;7:112.
4. Bryan CS, Yarbrough WM. Prevention of Deep Wound Infection after Coronary Artery Bypass Grafting: a review. Tex Heart Inst J. 2013;40(2):125-139.
5. CDC/NHSN Surveillance Definition of Healthcare-Associated Infection and Criteria for Specific Types of Infections in the Acute Care Setting. 2013;Available at: http://www.cdc.gov/nhsn/pdfs/pscmanual/17pscnosinfdef_current.pdf.
6. Kubota H, Miyata H, Motomura N, et al. Deep sternal wound infection after cardiac surgery. J Cardiothorac Surg. 2013;8:132.
7. Sakamoto H, Fukuda I, Oosaka M, et al. Risk factors and treatment of deep sternal wound infection after cardiac operation. Ann Thorac Cardiovasc Surg. 2003;9(4):226-232.
8. Ferris TG, Torchiana DF. Public release of clinical outcomes data-online CABG report cards. N Engl J Med. 2010; 363(17):1593-1595
9. Risnes I, Abdelnoor M, Almdahl SM, et al. Mediastinitis after coronary artery bypass grafting risk factors and long-term survival. Ann Thorac Surg. 2010;89:1502.
10. Bor DH, Rose RM, Modlin JF, et al. Mediastinitis after cardiovascular surgery. Rev Infect Dis. 1983;5:885.
11. Loop FD, Lytle BW, Cosgrove DM, et al. J. Maxwell Chamberlain memorial paper. Sternal wound complications after isolated coronary artery bypass grafting: early and late mortality, morbidity, and cost of care. Ann Thorac Surg. 1990;49:179.
12. El Oakley RM, Wright JE. Postoperative mediastinitis: classification and management. Ann Thorac Surg. 1996;61:1030.
{kind=link}