Volume 17, Issue 3, May 2016
Kristi L. Koenig, MD et al.
First isolated in 1947 from a monkey in the Zika forest in Uganda, and from mosquitoes in the same forest the following year, Zika virus has gained international attention due to concerns for infection in pregnant women potentially causing fetal microcephaly. More than one million people have been infected since the appearance of the virus in Brazil in 2015. Approximately 80% of infected patients are asymptomatic. An association with microcephaly and other birth defects as well as Guillain-Barre Syndrome has led to a World Health Organization declaration of Zika virus as a Public Health Emergency of International Concern in February 2016. Zika virus is a vector-borne disease transmitted primarily by the Aedes aegypti mosquito. Male to female sexual transmission has been reported and there is potential for transmission via blood transfusions. After an incubation period of 2–7 days, symptomatic patients develop rapid onset fever, maculopapular rash, arthralgia, and conjunctivitis, often associated with headache and myalgias. Emergency department (ED) personnel must be prepared to address concerns from patients presenting with symptoms consistent with acute Zika virus infection, especially those who are pregnant or planning travel to Zika-endemic regions, as well as those women planning to become pregnant and their partners. The identify-isolate-inform (3I) tool, originally conceived for initial detection and management of Ebola virus disease patients in the ED, and later adjusted for measles and Middle East Respiratory Syndrome, can be adapted for real-time use for any emerging infectious disease. This paper reports a modification of the 3I tool for initial detection and management of patients under investigation for Zika virus. Following an assessment of epidemiologic risk, including travel to countries with mosquitoes that transmit Zika virus, patients are further investigated if clinically indicated. If after a rapid evaluation, Zika or other arthropod-borne diseases are the only concern, isolation (contact, droplet, airborne) is unnecessary. Zika is a reportable disease and thus appropriate health authorities must be notified. The modified 3I tool will facilitate rapid analysis and triggering of appropriate actions for patients presenting to the ED at risk for Zika.
Volume 16, Issue 5, September 2015.
Kristi L. Koenig, MD.
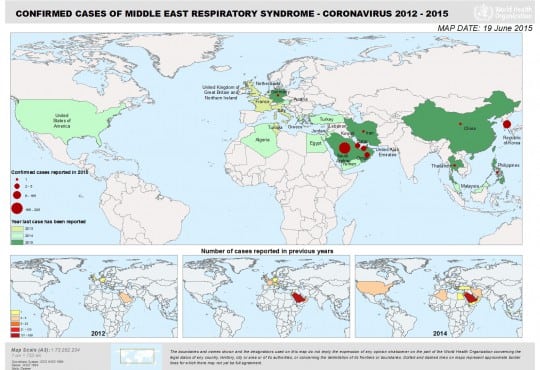
Middle East respiratory syndrome (MERS) is a novel infectious disease caused by a coronavirus
(MERS-CoV) first reported in Saudi Arabia in September 2012. MERS later spread to other countries
in the Arabian Peninsula, followed by an outbreak in South Korea in 2015. At least 26 countries
have reported MERS cases, and these numbers may increase over time. Due to international
travel opportunities, all countries are at risk of imported cases of MERS, even if outbreaks do not
spread globally. Therefore, it is essential for emergency department (ED) personnel to be able to
rapidly assess MERS risk and take immediate actions if indicated. The Identify-Isolate-Inform (3I)
tool, originally conceived for initial detection and management of Ebola virus disease patients in the
ED and later adjusted for measles, can be adapted for real-time use for any emerging infectious
disease. This paper reports a modification of the 3I tool for use in initial detection and management
of patients under investigation for MERS. Following an assessment of epidemiologic risk factors,
including travel to countries with current MERS transmission and contact with patients with confirmed
MERS within 14 days, patients are risk stratified by type of exposure coupled with symptoms of fever
and respiratory illness. If criteria are met, patients must be immediately placed into airborne infection
isolation (or a private room until this type of isolation is available) and the emergency practitioner
must alert the hospital infection prevention and control team and the local public health department.
The 3I tool will facilitate rapid categorization and triggering of appropriate time-sensitive actions for
patients presenting to the ED at risk for MERS.
Volume 16, Issue 2, March 2015
Kristi L. Koenig, MD et al.
Measles (rubeola) is a highly contagious airborne disease that was declared eliminated in the U.S. in the year 2000. Only sporadic U.S. cases and minor outbreaks occurred until the larger outbreak beginning in 2014 that has become a public health emergency. The “Identify-Isolate-Inform” tool will assist emergency physicians to be better prepared to detect and manage measles patients presenting to the emergency department. Measles typically presents with a prodrome of high fever, and cough/coryza/conjunctivitis, sometimes accompanied by the pathognomonic Koplik spots. Two to four days later, an erythematous maculopapular rash begins on the face and spreads down the body. Suspect patients must be immediately isolated with airborne precautions while awaiting laboratory confirmation of disease. Emergency physicians must rapidly inform the local public health department and hospital infection control personnel of suspected measles cases.
{kind=link}