
{kind=link}
| Author | Affiliation |
| Brent Felton, DO | Michigan State University, Sparrow Health System, Department of Emergency Medicine, Lansing, Michigan |
| Tam Dao, MD | Michigan State University, Sparrow Health System, Department of Emergency Medicine, Lansing, Michigan |
| Brett Gerstner, DO | Michigan State University, Sparrow Health System, Department of Emergency Medicine, Lansing, Michigan |
| Shawn Letarte, MD | Michigan State University, Sparrow Health System, Department of Emergency Medicine, Lansing, Michigan |
A 57-year-old male with a history of diabetes mellitus, hepatitis C, and intravenous drug abuse presented to the emergency department complaining of abdominal pain of three months duration that had worsened in the week prior to presentation. Review of systems was significant for back pain, nausea, and fever. The patient’s physical examination demonstrated a diffusely tender abdomen in addition to bilateral costo-vertebral angle tenderness, bilateral lower extremity weakness, and decreased rectal tone. An acute abdominal series was ordered to evaluate for bowel perforation (Figure). After review of this radiograph, magnetic resonance imaging (MRI) of the thoracic spine was ordered to confirm the suspected diagnosis of epidural abscess (Figure). The patient was transferred to the operating room for successful thoracic hemi-laminectomy and discharged home on post-op day seven.
The incidence of spinal epidural abscess has been estimated to account for 0.2-2.0 per 10,000 admissions, although recent studies report that the incidence is rising owing to increased rates of intravenous drug abuse and spinal surgical instrumentation.1,2 While the utility of plain film radiography is limited in the initial evaluation of suspected epidural abscess, abnormalities suggesting the presence of the disease in the form of end plate erosions or findings suggestive of osteomyelitis should not be ignored as these findings may be present in up to 89% of cases.3-5 In contrast, MRI with gadolinium contrast has a reported sensitivity of 91% with an associated specificity of 100%, rendering it the imaging modality of choice.5-7 Timely diagnosis of this relatively rare condition is paramount as the associated mortality of 5-16% is significant.8,9
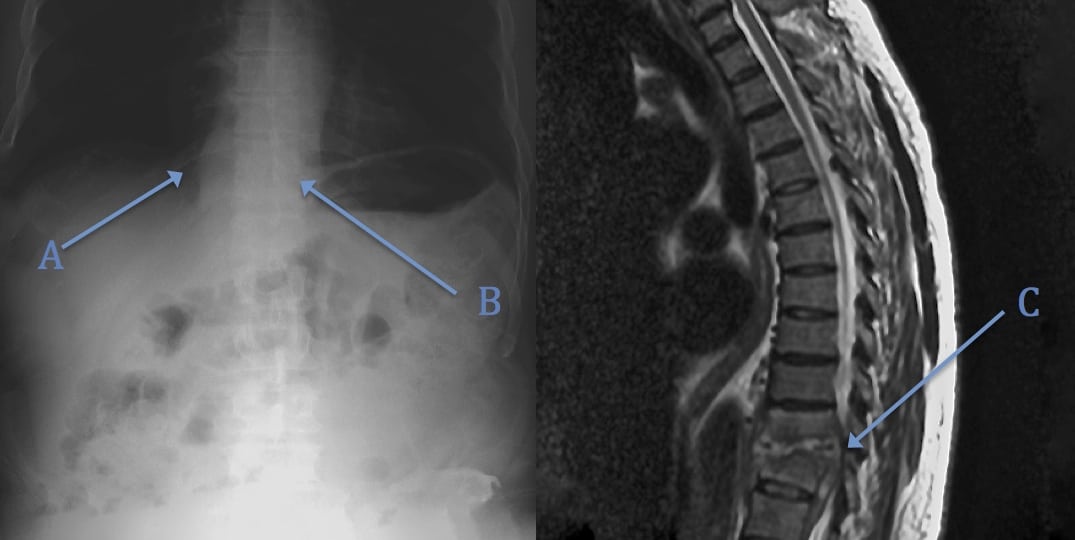
Figure. Magnetic resonance imaging of thoracic spine. Upright abdominal image demonstrating (A) paraspinal soft tissue density at the T10-T11 level worrisome for the possibility of paraspinal abscess, (B) poor visualization of the T10-T11 disc interspace, and (C) MRI demonstrating findings consistent with diskitis and associated sub-ligamentous abscess extending into the spinal canal at T11 and T12 with cord compression and severe central canal stenosis at these levels.
Footnotes
Supervising Section Editor: Sean O. Henderson, MD
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Brent Felton, DO, 2370 Robins Way, Okemos, MI 48864. Email: feltonbr@gmail.com.
Submission history: Submitted May 8, 2014; Revision received June 9, 2014; Accepted August 31, 2014
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
- Baker AS, Ojemann RG, Swartz MN, et al. Spinal Epidural Abscess. N Engl J Med. 1975;293:463-468. [PubMed]
- Hlavin ML, Kaminsky HJ, Ross JS, et al. Spinal Epidural Abscess: a ten-year perspective. Neurosurgery. 1990;27:177-184. [PubMed]
- Baker, CJ. Primary spinal epidural abscess. Am J Dis Child. 1971;121:337-339. [PubMed]
- Russell NA, Vaughan R, Morley TP. Spinal epidural infection. Can J Neurol Sci. 1979;6:325-328. [PubMed]
- Mylona E, Samarkos M, Kakalou E, et al. Pyogenic vertebral osteomyelitis: a systemic review of clinical characteristics. Semin Arthritis Rheum. 2009;39:10-7. [PubMed]
- Rigamonti D, Liem L, Sampath P, et al. Spinal epidural abscess: contemporary trends in etiology, evaluation, and management. Surg Neurol. 1999;52:189-96. [PubMed]
- Tompkins M, Panuncialman I, Lucas P, et al. Spinal epidural abscess. J Emerg Med. 2010;39:384-90. [PubMed]
- Darouiche RO. Spinal Epidural Abscess. N Engl J Med. 2006;355:2012-20. [PubMed]
- Reihsaus E, Waldbaur H, Seeling W. Spinal epidural abscess: a meta-analysis of 915 patients. Neurosurg Rev. 2000;23:175-204. [PubMed]
{kind=link}