
{kind=link}
| Author | Affiliation |
|---|---|
| Jeri K. Rose, DO | JPS Health Network, Department of Emergency Medicine, Fort Worth, Texas |
| Daniel Roberts, MD | CHRISTUS Spohn Hospital-Memorial, Department of Emergency Medicine Corpus Christi, Texas |
| Michael Simmons, MD | CHRISTUS Spohn Hospital-Memorial, Department of Emergency Medicine Corpus Christi, Texas |
A 63-year-old female with a past medical history of hepatitis C and cirrhosis presented to the emergency department with a four-month history of increased swelling and tenderness to the right clavicle. The patient was afebrile with a firm, warm area measuring 6 cm x 4.5 cm x 2 cm, located over the medial right clavicle. The patient had a remote history of minor trauma that resulted in no fractures and required no interventions. She was diagnosed with sternoclavicular (SC) septic arthritis, with underlying osteomyelitis of the clavicle and sternum noted on plain radiographs and confirmed bycomputed tomography (CT).
Septic arthritis of the SC joint accounts for only 1% of all septic arthritis in the general population, but up to 17% in intravenous (IV) drug users. Common risk factors include IV drug use, distant site of infection, diabetes mellitus, and thoracic central venous line (CVL) placement. Less common predisposing conditions include minor trauma, cellulitis, cirrhosis, and immunocompromised states. Unlike the acute presentation of other septic joints, SC septic arthritis usually develops more slowly over 14 days.1,2
Patients suspected of having SC joint septic arthritis require either CT (83% sensitive) or magnetic resonance imaging (nearly 100% sensitive) to identify SC joint infections.2Blood and wound cultures guide antibiotic treatments; wound cultures may be obtained by simple incision and drainage, but usually require CT-guided needle aspiration. 3,4
Patients with radiologic evidence of SC joint infection should be treated aggressively with IV anti-staphylococcal antibiotics, based on local sensitivities. Gram-negative coverage should be added in IV drug users, immunocompromised, and patients with CVL infections.3 Antibiotic coverage should then be tailored based on blood and aspiration cultures of the affected SC joint. The majority of SC joint infections will require surgical debridement.4

Photograph of patient’s wound when she presented to the emergency department.
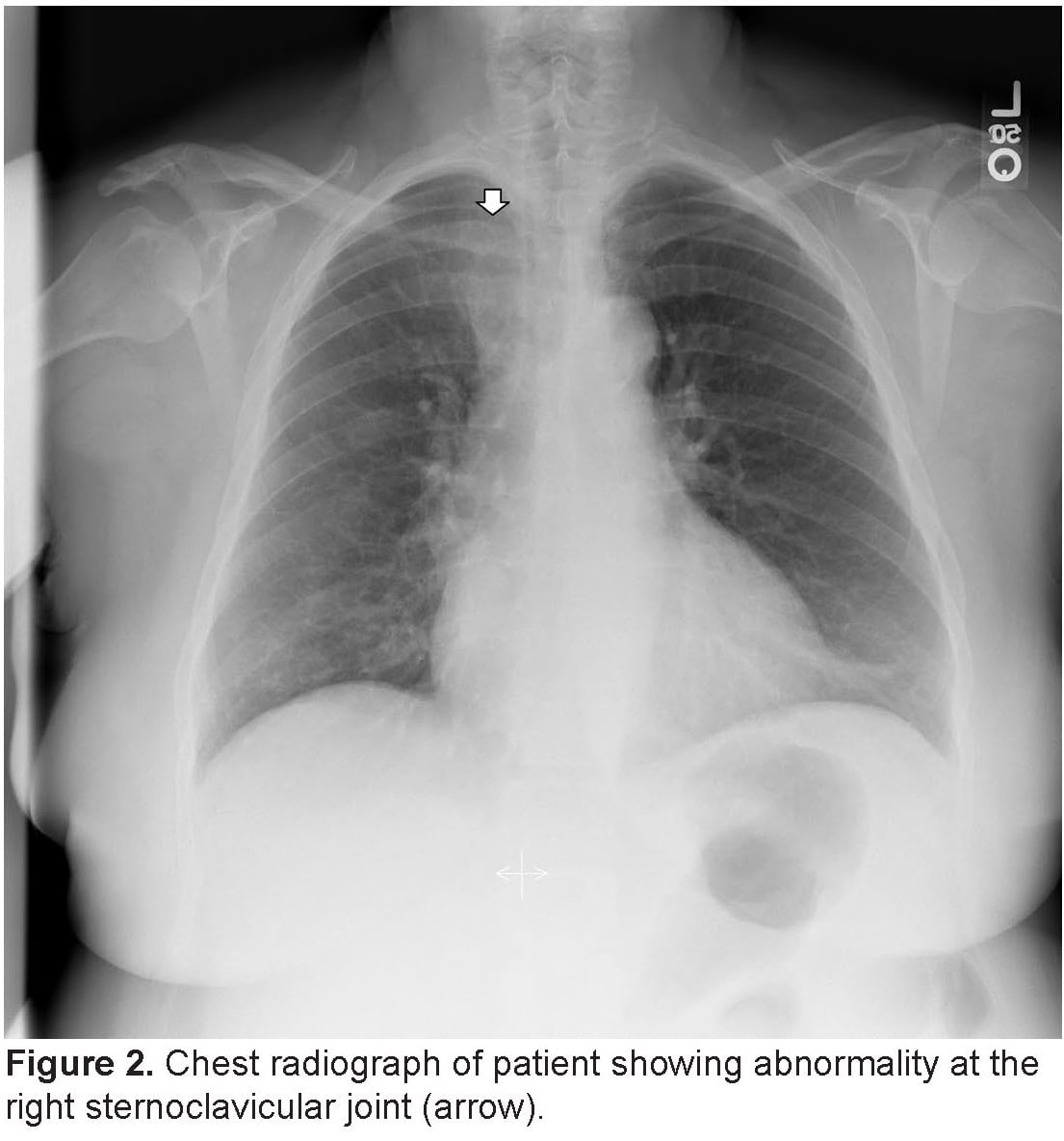
Chest radiograph of patient showing abnormality at the right sternoclavicular joint (arrow).
 with overlying soft tissue swelling (arrow head).")
Non-contrast computed tomography of chest showing erosion of the right medial clavicle (arrow) with overlying soft tissue swelling (arrow head).
Footnotes
Supervising Section Editor: Sean O. Henderson, MD
Submission history: Submitted February 27, 2012; Accepted March 8, 2012
Full text available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2012.3.11973
Address for Correspondence: Jeri K Rose, DO. JPS Health Network, Departement of Emergency Medicine, 1575 S. Main, Fort Worth, Texas
Email: jkrose360@gmail.com
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Ross JJ, Shamsuddin H. Sternoclavicular Septic Arthritis: review of 180 cases.Medicine. 2004;83:139–148. [PubMed]
2. Fordham S, Cope S, Sach M. Optimal management of sternoclavicular septic arthritis.Eur J Emerg Med. 2009;16:219–220. [PubMed]
3. Moyer HR, Ghazi B, Feliciano DV. Sternoclavicular Joint Infection: a case report.Thorac Cardiov Surg. 2009;57:500–501.
4. Bar-Natan M, Salai M, Sidi Y, et al. Sternoclavicular Infectious Arthritis in Previously Healthy Adults. Semin Arthritis Rheum. 2002;32:189–195. [PubMed]
{kind=link}