
{kind=link}
| Author | Affiliation |
|---|---|
| Mauro Gallitelli, MD | Hospital “SS. Giovanni e Paolo,” Emergency Department, Venice, Italy |
| Pasquale De Chirico, MD | Hospital “Dimiccoli,” Radiology Department, Barletta, Italy |
ABSTRACT
Although pneumomediastinum (PM) is a cause of chest pain, which can be diagnosed on a plain chest radiograph, emergency physicians frequently miss the diagnosis. As follows a description of findings of PM on a chest radiograph.
A 16-year-old boy presented to the emergency department (ED) with complaints of severe (7 of 10), sudden onset of central chest pain radiating to the neck. The patient also reported difficulty in controlling his asthma symptoms with salbutamol inhalers over the last few days. Physical examination was unremarkable.
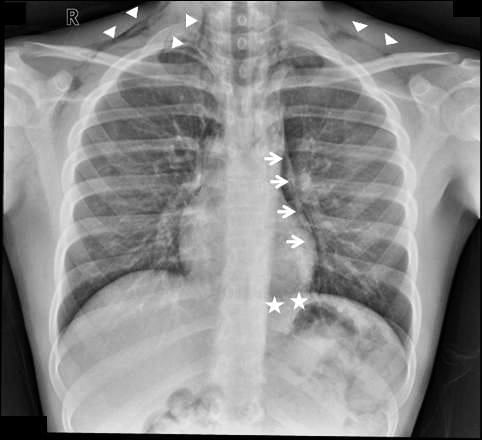
The chest radiograph showed a pneumomediastinum (PM).
Findings of PM1 on the chest radiograph (Figure) include the following: (1) detachment of the parietal pleura from the major mediastinal vessels and the pericardium (Figure, arrows), (2) the continuous diaphragm sign (Figure, stars) due to infiltration of air between the pericardium and diaphragm, (3) air lines in the mediastinum and in the subcutaneous tissues of the neck which, despite being easily detected, are not a constant finding (Figure, arrowheads). Other findings, though not observed in this case, are the Naclero V sign—which appears as a radiolucent V in the space between the descending aorta and the diaphragm on the chest radiograph, due to the infiltration of air in this space—and the ring around the artery sign, which can be observed in the lateral projection (normally not performed in the ED) owing to air infiltration of the right pulmonary artery.
The patient was discharged home on the advice that he should return at the onset of any worrying symptoms. At the follow-up appointment 4 days later, he was completely asymptomatic (pain ceased 2 days after the ED visit).
Spontaneous PM is believed to originate from alveolar rupture and air dissecting through the lung tissues (following vascular branches) into the mediastinum (Macklin effect).2 All the conditions causing an increase in alveolar pressure can facilitate this process (eg, exacerbation of asthma or chronic obstructive pulmonary disease, blunt chest trauma, mechanical ventilation). These conditions are similarly involved in the etiology of a pneumothorax, though it is not always known why a PM occurs.2
The clinical course of PM is rarely life threatening per se (although cases of tense PM have been described3) and largely depends on the underlying causes; for example, when PM arises from the rupture of the tracheobronchial tree or of the esophagus, prognosis can be much worse.4
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted January 24, 2011; Revision received February 25, 2011; Accepted February 25, 2011
Reprints available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2011.2.2209
Address for Correspondence: Mauro Gallitelli, MD
Hospital ‘‘SS. Giovanni e Paolo,’’ Emergency Department, Castello 6777, 30122 Venice, Italy
E-mail: mauro.gallitelli@libero.it
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Zylak CM, Standen JR, Barnes GR, et al. Pneumomediastinum revisited. Radiographics.2000;;20:1043–1057. [PubMed]
2. Iyer VN, Joshi AY, Ryu JH. Spontaneous pneumomediastinum: analysis of 62 consecutive adult patients. Mayo Clin Proc. 2009;;84:417–421. [PMC free article] [PubMed]
3. Paluszkiewicz P, Bartosinski J, Rajewska-Durda K, et al. Cardiac arrest caused by tension pneumomediastinum in a Boerhaave syndrome patient. Ann Thorac Surg. 2009;;87:1257–1258.[PubMed]
4. Smith BA, Ferguson DB. Disposition of spontaneous pneumomediastinum. Am J Emerg Med.1991;;9:256–259. [PubMed]
{kind=link}