
{kind=link}
| Author | Affiliation |
|---|---|
| Tareg Bey, MD | University of California, Irvine School of Medicine |
| Brian Ostick, MD | Christiana Care Emergency Medicine, Newark, Delaware |
ABSTRACT
A controversial term first described by Saunders and Harbaugh1 in 1984, Second Impact Syndrome (SIS) consists of two events. Typically, it involves an athlete suffering post-concussive symptoms following a head injury.2 If, within several weeks, the athlete returns to play and sustains a second head injury, diffuse cerebral swelling, brain herniation, and death can occur. SIS can occur with any two events involving head trauma. While rare, it is devastating in that young, healthy patients may die within a few minutes. Emergency physicians should be aware of this syndrome and counsel patients and their parents concerning when to allow an athlete to return to play. Furthermore, we present guidelines for appropriate follow up and evaluation by a specialist when necessary.
INTRODUCTION
Controversy surrounds Second Impact Syndrome (SIS), a condition so rare that even the frequency of its occurrence is in question. From 1980 to 1993 the National Center for Catastrophic Sports Injury Research in Chapel Hill, NC, identified 35 probable cases among American football players.2 However, this incidence is called into question by the lack of similar reports from Australian football, despite the high participation rate and a concussive injury rate approximately eight times that of American football. Furthermore, there are no similar reports from the European literature. However, a July 2007 eMedicine report summarizing an article in the American Journal of Sports Medicinenoted:
“A study of American high school and college football players demonstrated 94 catastrophic head injuries (significant intracranial bleeding or edema) over a 13-year period.3 Of these, only two occurred at the college level. Seventy-one percent of high school players suffering such injuries had a previous concussion in the same season, with 39% playing with residual symptoms.”4
Ropper and Gorson5 define concussion as an immediate and transient loss of consciousness accompanied by a brief period of amnesia after a blow to the head. Both anterograde and retrograde amnesia accompany the event.6 Retrograde amnesia can extend from moments to several days before the head trauma. The extent and period of anterograde memory loss tends to be shorter than retrograde.5
SIS is based on rare and mostly disputed cases in which a second mild head injury in children caused massive cerebral edema. McCrory7 points out that SIS is more likely a condition representing “diffuse cerebral swelling,” a consequence of traumatic brain injury with diffuse brain swelling that is well recognized in children. While there is argument over the incidence of SIS, many authors agree that the syndrome is rare.7,8While this may be comforting to emergency physicians (EPs), SIS must still be taken seriously as the consequences could be grave.
Epidemiology
The Centers for Disease Control and Prevention estimates about 1.1 million patients with nonfatal traumatic brain injury (TBI) are treated and released from U.S. hospital emergency departments (EDs) annually.9 An estimated 300,000 TBIs are mild to moderate10 and some 235,000 require hospitalization.9 Concussion is not uncommon, affecting about 128 people per 100,000 in the United States yearly. Young children have the highest rates of concussion, with sports and bicycle accidents accounting for the majority of cases in the 5–14 age group. Falls and vehicular accidents are the most common causes of concussion in adults.5 There is little epidemiological data about SIS. Most of the information comes from case reports or series.8 The overall incidence of secondary concussion and hence SIS is unknown. One reason for the lack of systematic epidemiological data comes from the controversy regarding the definition of SIS.4,5
Concussion
The word “concussion” comes from the Latin verb concutere (“to shake violently”).11 A concussion is defined as an immediate and transient loss of consciousness (LOC) accompanied by a brief period of amnesia after a blow to the head. In post-concussive syndrome, up to three symptoms arise within less than four weeks from the initial LOC.5These include headache, dizziness, fatigue, insomnia, irritability and alcohol intolerance, and other symptoms, such as subjective concentration, memory, or intellectual difficulties without neuropsychological evidence of marked impairment.5 In an article summarizing the Second International Conference on Concussion in Sport (Prague 2004), McCrory et al.12 differentiate between simple and complex concussions. A simple concussion is an athletic injury that resolves without complications within ten days, whereas a complex one involves persistent symptoms beyond ten days, or additional symptoms of seizures, cognitive impairment or exertional headache or confusion.
The extent of concussive amnesia roughly correlates with the duration of loss of consciousness and the severity of the head injury. Anterograde amnesia is the inability to retain new information. Retrograde amnesia is the inability to remember events preceding a traumatic injury. In some rare cases amnesia can extend backward for several days or longer.5 Content experts agree that all concussions mandate evaluation by a physician.12 Repeated brain injuries, including concussions occurring over an extended period of weeks to years, can result in neurologic and cognitive deficit, especially in boxers.10,13
Cognitive domain scores are often calculated from executive, attention and memory testing. Newer high technology methods include Diffusion Tensor Imaging (DTI), which is a more recent method of assessing axonal integrity in vivo. DTI characterizes white matter integrity.14 In a review of 18 cases of young athletes who sustained a second head injury before the first one had resolved Mori et al.8 found, that ten of the 18 did not lose consciousness. However, after the second traumatic brain injury, eight had a cranial CT scan revealing a subdural hematoma.8 The symptoms and ED presentation of severe concussion can be identical to SIS. The EP is rarely aware of a preceding concussion days to weeks earlier. Therefore, the evaluation and treatment of these two entities follow the same algorithm.
Pathophysiology of Second Impact Syndrome
A patient who sustains an initial concussion may develop cerebral edema, accounting for loss of consciousness, memory impairment, disorientation and headache. However, the brain’s auto regulatory mechanisms compensate for this mechanical and physiologic stress and protect against massive swelling. This is thought to be accomplished by acutely limiting cerebral blood flow, which leads to accumulation of lactate and intracellular acidosis.15 After the initial phase, a state of altered cerebral metabolism occurs and may last ten days,16 involving decreased protein synthesis and reduced oxidative capacity.11Extensive experimental research suggests that the loss of consciousness after head injuries, the development of secondary brain damage, and the enhanced vulnerability of the brain after an initial insult can be explained largely by characteristic ionic fluxes, acute metabolic changes, and cerebral blood flow alterations that occur immediately after cerebral concussions. Extracellular potassium concentration can increase massively in the brain after concussion, followed by hypermetabolism lasting up to ten days. This makes the brain more vulnerable and susceptible to death after a second sub-lethal insult of even less intensity.11 Fisher and Vaca17 hence conclude that when the patient sustains a “second impact,” the brain loses its ability to auto regulate intracranial and cerebral perfusion pressures. In severe cases, this may lead to cerebral edema followed by brain herniation. Death has been reported to occur in a matter of two to five minutes, usually without time to stabilize or transport an athlete from the playing field to the ED. This demise can occur far more rapidly than that of an epidural hematoma.18 Bruce et al.19point our that brain swelling in minor head trauma is more significant in small children than in adults. The term “malignant brain edema” has been used to describe this phenomenon. More research in this area is necessary to determine if and when malignant brain edema and SIS are related, or even if they occur by the same process.
Clinical Workup Following Head Trauma
Airway, breathing, and circulation must be assessed and treated following any head trauma seen in the ED or in the prehospital setting. Even in the absence of hard signs suggesting cervical spine or spinal cord injury, such as posterior midline pain or tenderness, paresthesias, extremity weakness or depressed consciousness, injury should be assumed and immobilization and radiography routine. A thorough history is imperative and must be taken from the patient, if conversant, or from a witness. Important information includes mechanism of injury, loss of consciousness, previous concussions, seizure history, transient weakness or paresthesias, difficulty walking, bladder or bowel incontinence, and alcohol or drug use. A thorough general physical exam should be performed with special attention to the neurological exam.
Diagnostic Imaging
If there is suspicion of a serious structural brain injury, immediate computed tomography (CT) of the head is needed.20 CT is usually easier to obtain and more sensitive than magnetic resonance imaging (MRI) to detect acute intracranial bleeding and identify surgically reversible injury.21 The CT scan should be reviewed for intraparenchymal, extra-axial, intraventricular or subarachnoid bleeding, diffuse cerebral swelling manifested by loss of the grey-white junction, and midline shift. In case of an anatomic abnormality, a neurosurgeon should be consulted.
Treatment
As stated above, true SIS involves brain herniation and death within minutes. Therefore, the odds of seeing acute SIS in the ED are unlikely. If suspected, the patient should be immediately stabilized with special emphasis on airway management, and neurosurgery consulted. Cantu22 also recommends rapid intubation and mannitol to minimize morbidity. This has not been tested and is based on expert opinion. The use of mannitol in the treatment of intracranial pressure (ICP) shows a small beneficial effect. However, there are insufficient data on the effectiveness of prehospital administration of mannitol.23 In the management of increased ICP the intubated patient should maintain normocapnic at about 30 mm Hg.24 The recent literature suggests that hypertonic saline is evolving as a real alternative to mannitol or may be used in otherwise refractory intracranial hypertension. Safety data on hypertonic saline in the treatment of intracranial hypertension are very limited, and the efficacy and duration of ICP-lowering are difficult to predict.25
Prevention
Any athlete who still shows signs of concussion should not be allowed to return to play. Such signs include fatigue, headache, disorientation, nausea, vomiting, feeling “in a fog” or “slowed down,” as well as other differences from a patient’s baseline.18 If there are any doubts about the severity of injury, the patient or athlete should not be allowed to resume play.
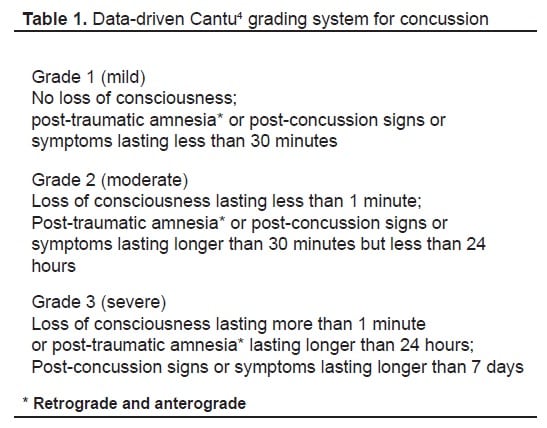
The difficulty lies in deciding the appropriate return to play when the athlete is completely asymptomatic. Parents, teachers and the coach must observe the athlete closely. High school athletes and those with scholarship possibilities, especially, will try to convince parents and coaches that they feel fine, in order to resume play. There are differences of opinion as to when it is appropriate for a post-concussive patient to resume play. Cantu18 suggests a grading system to rate the severity of concussions, ranging from Grade 1 through Grade 3 (Table 1). Three widely referenced clinical guidelines advise on the timing and level of participation after a first concussion.3,4,5 Unfortunately, none are evidence based, and their recommendations differ widely. Some even discuss a stepwise approach to return to play. The EP should focus on the initial stabilization, imaging and the exclusion of a life-threatening or surgically-treatable lesion. The EP should also ensure appropriate outpatient follow up by a neurosurgeon or a sports physician who has expertise with concussive symptoms. Although information on SIS is present in the medical literature, its description in 1984 may leave some non-specialists unaware of the potential danger. Currently the guidelines suggested by the American Academy of Neurology26 listed in Table 2 are the most widely disseminated and used.

The most sensible approach to prevention is to prevent the first concussion. For soccer, Kangaroo Soccer Headgear, similar to that used in martial arts, is primarily intended to provide protection for children and youth players. Coverage extends around the head, including the ears. The headgear is intended to protect against player-to-player impacts.27 These headgear models did provide measurable benefit during head-to-head impacts, but not necessarily with ball impact. Experts advise wearing a helmet during high-impact contact sports and preventing or mitigating especially head-to-head contact.
CONCLUSION
More meaningful research is needed to investigate SIS. In light of its rarity, research should focus on observational study of the incidence of primary concussion in similar systems that do and do not employ head protection. Research should be aimed at unifying an algorithm for the work up and treatment of concussions and potential predisposition for SIS, as well as developing guidelines for return to play. At this point, given the limited information on this topic, the prevention of high impacts during sport is the goal for young athletes. When in doubt after a severe concussion, the athletes should not resume play. “When in doubt, sit them out.”11
Appendix
Testing Guidelines for the Management of Sport-Related Concussion.24 Testing includes:
|
Footnotes
Supervising Section Editor: Mark I. Langdorf, MD, MHPE
Submission history: Submitted October 06, 2008; Revision Received September 11, 2008; Accepted September 12, 2008
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Tareg Bey, MD, FACEP. Department of Emergency Medicine, UC Irvine Medical Center, 101 The City Drive, Rte 128, Orange, CA 92868
Email: tbey@uci.edu
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Saunders R, Harbaugh R. The second impact in catastrophic contact-sports head trauma. JAMA. 1984;252:538–539. [PubMed]
2. Cantu RC. Second impact syndrome. Clin Sports Med. 1998;17:37–44. [PubMed]
3. Boden BP, Tacchetti RL, Cantu RC, Knowles SB, Mueller FO. Catastrophic head injuries in high school and college football players. Am J Sports Med. 2007;35:1075–1081.[PubMed]
4. Cifu D, Steinmetz BD, Drake DF. Repetitive head injury syndrome. [Accessed August 29, 2008];eMedicine. 2008 March 24; Available at:http://www.emedicine.com/sports/TOPIC113.HTM.
5. Ropper A, Gorson H. Concussion. N Engl J Med. 2007;356:166–172. [PubMed]
6. Cantu RC. Post traumatic (retrograde/anterograde) amnesia; pathophysiology and implications in grading and safe return to play. J Athl Train. 2001;36:244–248.[PMC free article] [PubMed]
7. McCrory P. Does second impact syndrome exist? . Clin J Sport Med. 2001;11:144–149.[PubMed]
8. Mori T, Katayama Y, Kawamata T. Acute hemispheric swelling associated with thin subdural hematomas: pathophysiology of repetitive head injury in sports. Acta Neurochir [Suppl] 2006;96:40–43.
9. Centers for Disease Control (CDC) Nonfatal traumatic brain injuries from sports and recreation activities – United States, 2001–2005. MMWR. 2007;56:733–737. [PubMed]
10. Centers for Disease Control (CDC) Sports-related recurrent brain injuries- United States. MMWR. 1997;46:224–227. [PubMed]
11. Maroon J, Lovell MR, Norwig J, et al. Cerebral concussion in athletes: evaluation and neuropsychological testing. Neurosurgery. 2000;47:659–669. [PubMed]
12. McCrory P, Johnson K, Meeuwisse W, et al. Summary and agreement statement of the Second International Conference on concussion in sport, Prague 2004. Clin J Sport Med.2005;15:48–55. [PubMed]
13. Jordan BD, Zimmermann RD. Computed tomography and magnetic resonance imaging comparisons in boxers. JAMA. 1990;263:1670–1674. [PubMed]
14. Kraus MF, Susmaras T, Caughlin BP, Walker CJ, Sweeney JA, Little DM. White matter integrity and cognition in chronic traumatic brain injury: a diffusion tensor imaging study. Brain. 2007;130:2508–2519. [PubMed]
15. DeSalles AA, Kontos HA, Ward JD, Marmarou A, Becker DP. Brain tissue pH in severely head-injured patients: A report of three cases. Neurosurgery. 1987;20:297–301.[PubMed]
16. Kawamata T, Katayama Y, Hovda D, Yoshino A, Becker D. Administration of excitatory amino acid antagonists via microdialysis attenuates the increase in glucose utilization seen following concussive brain injury. J Cereb Blood Flow Metab. 1992;12:12–24. [PubMed]
17. Fischer J, Vaca F. Sport-related concussions in the emergency department. Top Emerg Med. 2004;26:260–266.
18. Cantu RC. Recurrent athletic head injury: risks and when to retire. Clin Sports Med.2003;22:593–603. [PubMed]
19. Bruce DA, Alavi A, Bilaniuk L, Dolinskas C, Obrist W, Uzzell B. Diffuse cerebral swelling following head injuries in children: the syndrome of “malignant brain edema” J Neurosurg. 1981;54:170–178. [PubMed]
20. McCrory P, Berkovic S, Cordner S. Deaths due to brain injury among footballers in Victoria, from 1968 to 1998. Med J Aust. 2000;172:217–220. [PubMed]
21. Doezema D, King J, Tandberg D, et al. Magnetic resonance imaging in minor head injury. Ann Emerg Med. 1991;20:1281–1285. [PubMed]
22. Scheid R, Walther K, Guthke T, Preul C, von Cramon DY. Cognitive sequelae of diffuse axonal injury. Arch Neurol. 2006;63:418–424. [PubMed]
23. Wakai A, Roberts I, Schierhout G. Mannitol for acute traumatic brain injury.Cochrane Database of Systematic Reviews. 1998;(Issue 1) Art. No.: CD001049.
24. Neurotrauma. Intracranial pressure. [Accessed May 8, 2008]. Available at:http://www.trauma.org/archive/neuro/icpcontrol.html.
25. Himmelseher S. Hypertonic saline solutions for treatment of intracranial hypertension. Curr Opin Anaesthesiol. 2007;20:414–426. [PubMed]
26. American Academy of Neurology. Practice parameter: the management of concussion in sports (summary statement) – report of the Quality Standards Subcommittee.Neurology. 1997;48:581–585. [PubMed]
27. Withnall C, Shewchenko N, Wonnacott M, Dovrak J. Effectiveness of headgear in football. Brit J Sports Med. 2005;39(Suppl1):i40–i48. [PMC free article] [PubMed]