
{kind=link}
| Author | Affiliation |
|---|---|
| Joseph E. Tonna, MD | Stanford/Kaiser Emergency Medicine, Stanford University, CA |
| Amy M. Balanoff, PhD | American Museum of Natural History |
| Matthew R. Lewin, MD, PhD | Institute for Exploration and Travel Health, California Academy of Sciences, San Francisco, CA |
| Namjilmaa Saandari, MD, MPH | National Public Health Service, Ulaanbaatar, Mongolia |
| Max Wintermark, MD | University of Virginia, Department of Radiology, Neuroradiology Division |
ABSTRACT
In preparing a case report on Brown-Séquard syndrome for publication, we made the incidental finding that the inexpensive, commercially available three-dimensional (3D) rendering software we were using could produce high quality 3D spinal cord reconstructions from any series of two-dimensional (2D) computed tomography (CT) images. This finding raises the possibility that spinal cord imaging capabilities can be expanded where bundled 2D multi-planar reformats and 3D reconstruction software for CT are not available and in situations where magnetic resonance imaging (MRI) is either not available or appropriate (e.g. metallic implants). Given the worldwide burden of trauma and considering the limited availability of MRI and advanced generation CT scanners, we propose an alternative, potentially useful approach to imaging spinal cord that might be useful in areas where technical capabilities and support are limited.
INTRODUCTION
While many modern computed tomography (CT) scanners contain software that can automatically produce two-dimensional (2D) multi-planar reformats (MPR) and three-dimensional (3D) reconstructions, this technology is not available in much of the developing world. Additionally, magnetic resonance imaging (MRI), which has become the mainstay of spinal cord imaging, is also difficult to obtain in many places. Commercially available 3D reconstruction technology commonly used in paleontology and engineering research can be used to perform 3D reconstructions from any contiguous series of 2D images. Worldwide, there is a large number of single and quadruple slice CT scanners and scanners otherwise unable to perform 2D MPR reformats or automatic 3D reconstructions. The ability to create 3D reconstructions from standard 2D CT images on a standard laptop may expand the useful life and use of those CT scanners. Having an MRI or CT capable of MPR reformats or 3D reconstructions is not a prerequisite to having neurosurgical capabilities but is often desired for planning surgery; as such, this software could additionally decrease the barriers to operative intervention and possibly extend the usefulness of early generation CT scanners lacking advanced software bundles for multi-planar reconstruction.
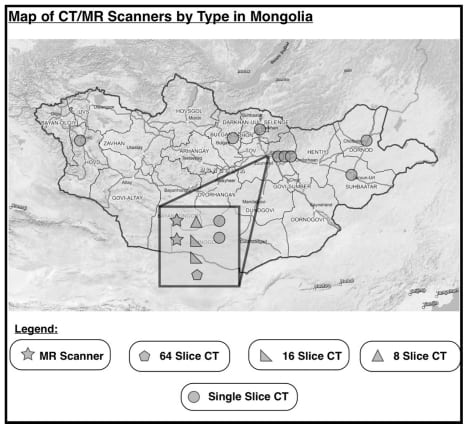
In a developing country, such as Mongolia, advanced generation CT scanners and neurosurgical support are scarce. Mongolia is about 1.7 million square kilometers—about three times the size of Texas with a population of 2.8 million people, 1.3 million of whom live in its largest city, Ulaanbaatar. This central Asian country has only 14 CT scanners and two MRI units. Of the 14 CT scanners, six are in the capitol city (Ulaanbaatar) and five of the six can write to compact discs (CD). Only one of the six CT scanners outside of Ulaanbaatar can write to CD. The two MRIs are also located in Ulaanbaatar. As of this writing, there are six neurosurgeons in Mongolia performing trauma-related operations on the brain and spine. The distribution of CT and MRI scanners there is shown in figure 1. Herein, we comment on the workup of a patient suspected to have Brown-Séquard syndrome to illustrate a potential strategy for imaging patients where MRI is either not available or not appropriate and/or where advanced generation CT imaging is not available.
METHODS
Three dimensional reconstructions were created by importing 2D CT scans (in this case, Digital Imaging and Communications in Medicine images, 1.25mm in thickness) into the image rendering program VGStudio Max 1.2.1 (http://www.volumegraphics.com). This software is one of several commercially available volumetric rendering programs that make feasible digital manipulation of CT data (Appendix A).1 We manually grouped components of the CT scan slices, based on density and removed or made transparent undesired regions. Desired isodense regions were digitally highlighted and linked over multiple images, producing a 3D structure. This allows for manual selection and highlighting of desired image densities (tissues), thus achieving clinical discrimination of the spinal cord, spinal fluid, thecal sac and other tissues from each other and from bone. Interestingly, images can be formatted into movies, allowing the viewer to observe the 3D scans from any perspective (see web version of this manuscript and at http://www.escholarship.org/uc/uciem_westjem). Amy Balanoff, the person performing the reconstructions for this paper, is a paleontologist with no medical training and was not privy to the diagnoses of the patients we examined for publication of what was originally intended to be a series of case reports. Dr. Wintermark, a neuroradiologist, reviewed the original CT images as well as the reconstructions during the production of this manuscript. The map of Mongolia (Figure 1) was provided courtesy of Dr. Saandari (MONMAP Engineering Services Co., Ulaanbaatar, Mongolia; www.monmap.mn). Data regarding the distribution and availability of advanced cross-sectional imaging as well as neurosurgical services in Mongolia were provided by Drs. N. Saandari and T. Ganzorigt of the Mongolian Public Health Service and Achtan Elite Hospital, Ulaanbaatar, Mongolia. The CT scanner in use to image the patients shown in this report was a GE Lightspeed 16 slice CT scanner (General Electric Healthcare, Waukesha, WI).
Illustrative Case
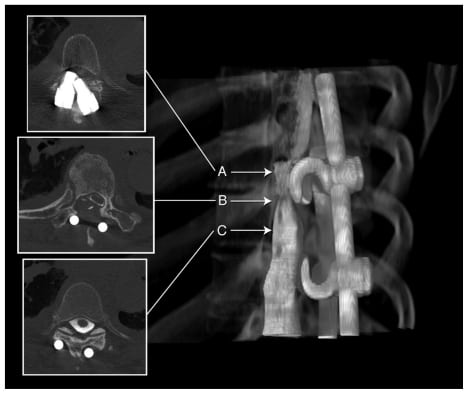
A 63-year-old woman with bilateral Harrington rods for severe, congenital scoliosis was in a Pilates class when she felt a “pop” in her back and developed the progressive onset of lower extremity weakness over two days. Upon presentation to a university emergency department in the United States (U.S.), she complained of worsening right leg weakness to the point that she was unable to walk. On exam, she was found to have right lower extremity weakness of large and small muscle groups in flexion and extension and ipsilateral sensory deficits to light touch and proprioception in a spinal distribution pattern, with contralateral sensory dimunation to pain and temperature at approximately the same spinal level—pathognomonic for Brown-Séquard type spinal cord hemisection or compression. The Harrington rods were MRI incompatible, so a CT myelogram was performed, with which a diagnosis of hemi-compression of the spinal cord was radiologically confirmed (Figure 2, A–C insets). She was taken to the operating room where the Harrington rods were removed from the spinal canal. The patient had nearly full recovery of motor and sensory function since the cord was compressed, not severed. In Figure 2 (main frame), we constructed the 2D CT images using the described technique. The resultant images enabled direct 3D visualization the impingement of the Harrington rods on the spinal canal, thecal sac and cord.
DISCUSSION
Worldwide there is a large number of early generation single and quadruple slice CT scanners and scanners otherwise unable to perform 2D MPR reformats or automatic 3D reconstructions. These reconstructions not only aid in the diagnosis of the acute spinal cord injury, but have become a common part of the neurosurgical pre-operative workup. The ability to create 3D reconstructions from standard 2D CT images on a standard laptop may expand the useful life and use of a large number of CT scanners. Having an MRI or CT capable of MPR reformats or 3D reconstructions is not a prerequisite to having neurosurgical capabilities, but is often desired for planning surgery; as such, this software could additionally decrease the barriers to operative intervention.
As approximately one-fourth of patients have persistent spinal cord compression after osseous spinal realignment,3 it is sometimes important that providers achieve adequate visualization of non-osseous tissues (e.g. of thecal or spinal cord compression), especially when neurological deficits exist or persist in the setting of trauma or disease. While our reformats were post-hoc and thus did not affect management, our manual reformat could digitally remove the bony structures and highlight the desired regions, thus enabling visualization of the non-osseous structures (thecal sac, spinal canal).
The ability to use low-cost Internet-available software to process any 2D CT images of acute spinal cord injury into 3D reformats (rather than relying on MPR software bundled CT, multi detector CT or MRI) has broad implications worldwide for the evaluation and treatment of trauma victims and those with suspected acute spinal cord compression from other causes (eg tumor, epidural abscess or hematoma) where multi-detector CT (MDCT) scanners with bundled automatic 3D reconstruction software are not available, let alone where MRI is unavailable. In the described case, the CT scan was obtained with myelography contrast. We have subsequently performed 3D reconstructions from 2D CT images without contrast, with promising results (example shown in Appendix B).
Potentially increasing the available imaging modalities for acute spinal cord injury could be significant considering the burden of disease and healthcare costs associated with this injury type. The World Health Organization estimates that road traffic accidents, a leading cause of spinal cord trauma, will rise to third on the global burden of disease ranking by 2030.4,5 As estimated by the National Spinal Cord Injury Statistical Center in 2009, average yearly expenses as a result of spinal cord injury (not including lost wages, productivity and fringe benefits) vary from $236,109 to $801,161 in the first year with lifetime costs between $500,000 and $3 million dollars.5 Thus, any ability to increase the definitive characterization of acute spinal trauma and expedite its management by enhanced visualization may help decrease the healthcare and financial burden from acute spinal cord injury. Importantly, the American College of Radiology (ACR) does not list trauma as a contraindication for CT-myelography. In fact, there are no absolute contraindications to the procedure listed by the ACR, including major trauma.2
Three dimensional images and movies may be better for surgeons planning operative approach, especially if they are available on mobile computers such as laptops. Such 3D images may reduce inter-observer variability and may give results that are more objective compared to 2D CT images. Not all patients are suitable for MRI. Many have metal implants, some are on ventilators, and others may be claustrophobic. CT additionally enables the neurological or orthopedic surgeon to obtain high quality bone images, which may be of equal priority. CT scanners are available worldwide, whereas MR technology is largely limited to the developed world and, even then, largely in urban and wealthier suburban areas. We note with interest that myelography is not even mentioned in the latest editions of some leading textbooks of emergency medicine and may have been prematurely eliminated from consideration by the authors and editors updating these texts,6 Though most U.S. emergency medicine training programs and most U.S. emergency physicians work in technologically supportive settings with respect to imaging and the ability to transfer patients to higher levels of care, most of the world does not have this luxury. As we described earlier, in a developing country such as Mongolia, there is a dearth of advanced cross-sectional imaging and neurosurgical support—that which exists being concentrated in the capital city. Furthermore, emergency physicians should be familiar with their imaging options in the event a patient is not suitable for one modality or another or those modalities are suddenly not available.
LIMITATIONS
To our knowledge, this is the first report suggesting this combination of image acquisition and processing. Our method has not been validated in a clinical trial alone or in comparison to other advanced cross-sectional imaging techniques, such as MRI or MPR, or compared to clinical examination alone. The current processing time for these images was about three hours and was performed manually by a single individual (AM Balanoff) not medically trained but very familiar with the software program used. Compared to the time it takes to obtain an MRI technician, radiologist and complete a scan, these times are close. Based on the adequacy of the reconstructions for lesion visualization in a subsequent case (Appendix B), where the 2D CT images were without myelography contrast, it is suspected that the myelography procedure is not necessary for adequate spinal canal visualization after reconstruction. Even so, CT-myelography is actually a rather rapid procedure, involving only setup of a standard lumbar puncture, followed by injection of the contrast material (~2 minutes), transport to CT scanner and performance of the scan (~5 to 10 minutes). During reconstruction, the time required to perform digital isolations is variable. Density contrasts between bone and soft tissue are important variables in determining the degree of processing difficulty. Additionally, the digital processing software is rapidly advancing in an inverse relationship with processing time. Some patients may not be appropriate for CT-myelography, if this is desired, but it should be noted that there are no absolute contraindications to the technique and it can be performed very quickly (spinal puncture + image acquisition). As with any other invasive procedure, it is necessary to have expertise in this technique.2 Further research and development will be required to realize or confirm the use of this technique in the appropriate clinical settings.
CONCLUSION
The finding that high-resolution, 3D CT images of spinal cord could be obtained by applying technology and algorithms already used in engineering and paleontology to 2D CT images and processed on a standard laptop computer raises the possibility of extending the useful life and use of a large number of CT scanners worldwide, including single slice and non-MDCT scanners, and specifically those without 2D MPR reformat and 3D reconstruction capabilities. While availability of MRI or CT scanners capable of MPR reformats or 3D reconstructions is not a prerequisite to having neurosurgical capabilities, 2D MPR and 3D reconstructions have become a not uncommon part of the preoperative workup. Considering MDCTs with two or more channels can routinely produce 1.25mm slices, these software programs should be able to produce reconstructions with reasonably high accuracy, extending the use and versatility of older generation CT scanners.
Footnotes
Supervising Section Editor: Seric S. Cusick, MD
Submission history: Submitted January 1, 2010; Revision Received April 26, 2010; Accepted August 23, 2010
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Matthew R. Lewin, MD, PhD, Institute for Exploration and Travel Health, California Academy of Sciences, 55 Concourse Drive, Golden Gate Park, San Francisco, CA 94121
Email: mlewin@calacademy.org
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Stanford University National Biocomputation Center. 3D reconstruction software. [Accessed Mar 20, 2010]. Available at: http://biocomp.stanford.edu/3dreconstruction/software/index.html.
2. Practice guideline for the performance of myelography and cisternography. Am College of Radiology. 2008. [Accessed Dec 31, 2009]. Available at:http://www.acr.org/SecondaryMainMenuCategories/quality_safety/guidelines/dx/head-neck/myelography.aspx.
3. Allen RL, Perot PL, Gudeman SK. Evaluation of acute nonpenetrating cervical spinal cord injuries with CT metrizamide myelography. J of Neurosurgery. 1985;10;63(4):510–20.
4. World Health Organization. The global burden of disease: 2004 update. [Accessed Dec 31, 2009]. Available at:http://www.who.int/healthinfo/global_burden_disease/2004_report_update/en/index.html.
5. National Spinal Cord Injury Statistical Center. Spinal cord injury facts and figures at a glance.Birminham, AL: 2009. [Accessed Dec 30, 2009]. Available at: www.uab.edu/NSCISC.
6. Tintinalli J, Kelen GD, Stapczynski JS, et al. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 6th ed . The McGraw-Hill Companies, Inc.; 2004.
Appendix A: 3D Reconstruction Software
From Stanford University Biocomputation Center
3-D-E
Windows-based contour editor and visualizer from Data Cell Ltd. (Platforms: PC; Cost: ~$1500)
3DVIEWNIX
3DVIEWNIX is a transportable, very inexpensive software system developed by the Medical Image Processing Group, Department of Radiology, University of Pennsylvania, Philadelphia. It has state-of-the-art capabilities for visualizing, manipulating, and analyzing multidimensional, multimodality image information. It is designed to run on Unix machines under X-windows. (Platforms: SGI, Sun, PC; Cost: unknown)
Amira
Interactive segmentation and visualisation package for biomedical images. (Platforms: SGI, Sun, Windows; Cost: $$$$)
Analyze
Provides an environment for the interactive visualisation and manipulation of 2-D, 3-D and 4-D biomedical images. An integrated set of tools is provided to allow data to be interrogated in both two and three dimensions. (Platforms: SGI, Sun, HP, DEC; Cost: $$$)
AutoDeblur
AutoDeblur performs blind deconvolution for 3d data. (Platforms: SGI; Cost: unknown)
AVS
AVS – commercial visualization package from Advanced Visual Systems, Inc. (Platforms: SGI, Sun, HP, DEC; Cost: unknown)
Oncor
Biomedical image measurement and analysis system. (Platforms: Mac, PC; Cost: $$)
Bioquant
3D reconstruction and quantitative histochemistry system. (Platforms: PC; Cost: unknown)
BOB (GVLware)
The Army High Performance Computing Research Center (AHP-CRC) has been developing a set of tools to work with large time dependent 2D and 3D data sets. (Platforms: SGI; Cost: free)
C_Images 3D
3D Image analysis package by Foster-Findlay Associates (UK). (Platforms: PC (DOS, Windows), Unix (IBM, Sun, SGI); Cost: unknown)
CELLscan
A system for high-resolution 3D fluorescence microscopy. Provides image acquisition, deconvolution, and analysis capabilities. (Platforms:PC; Cost: Unknown)
CT
CT programs by Malcolm Slaney. (Platforms: Many; Cost: free)
Deltavision
Image acquisition and deconvolution software for 5-dimensional microscopy. (Platforms: SGI; Cost: unknown)
Dicer
Slicer/Dicer is a volumetric visual data analysis package. (Platforms: Mac; Cost: $)
DIP Station
Macintosh-based reconstruction package. (Platforms: Mac; Cost: unknown)
Dr. Razz
CT/MR display and analysis program for Macintosh color computers. (Platforms: Mac; Cost: free)
EM3D
Electron microscopy reconstruction software package from Stanford. (Platforms: Win, UNix; Cost: free)
EutecticSSRS
Low-end 3D reconstruction, mapping, and analysis system. Contour-based using a digitizing tablet. (Platforms: PC; Cost: $24–28k (NTS), $8–10k (NTSV))
FAST
It is a software environment for visualizing and analyzing Computational Fluid Dynamics data. (Platforms: SGI; Cost: free)
HVEM 3D
PC-based serial section reconstruction program for microscopy created by Kinnamon/Young at UColorado. (Platforms: PC; Cost: unknown)
IAP
Imaging Applications Platform is a commercial package for medical and scientific visualization. (Platforms: Most workstations; Cost: $$)
IBM Data Explorer
IBM Data Explorer. (Platforms: IBM, SGI, Sun, HP, DG; Cost: unknown)
IDL
IDL (Interactive Data Language) is a package for the interactive reduction, analysis, and visualization of scientific data and images. (Platforms: IBM, SGI, Sun, HP, DEC, PC, Mac; Cost: $$)
Image Pro
Image Pro from Media Cybernetics ($2,999). (Platforms: PC (Win3.1, NT, 95); Cost: $$$)
ImageSpace
Software environment for confocal imaging. (Platforms: SGI; Cost: unknown)
Image Volumes
Interactive image processing, contour editing, 3D reconstruction for confocal, EM, X-ray tomography, and MRI. (Platforms: SGI; Cost: unknown)
Imagist
Imagist2 from Princeton Gamma Tech- integrated microscope and analysis systems. (Platforms: Sun; Cost: unknown)
IMOD
Image modeling package used for EM tomography and serial section reconstruction. (Platforms: unknown; Cost: unknown)
IRAF
IRAF (Image Reduction and Analysis Facility). (Platforms: unknown; Cost: unknown)
KBVision
Software environment for creating image understanding applications. (Platforms: Sun, IBM, DEC, SGI; Cost: $$)
Khoros
Very large, general image processing toolkit. (Platforms: Sun, SGI, IBM, DEC, HP; Cost: free)
MacCubeView
Designed to display a texture map image of three-dimensional (3-D) data. (Platforms: Mac; Cost: shareware)
MacPhase
2D data analysis and visualization application for the Macintosh. (Platforms: Mac; Cost: unknown)
MacStereology
MacStereology is package designed to make measurements of images and to make 3-D reconstructions. (Platforms: Mac; Cost: unknown)
MCID
Image analysis and quantification mainly for fluorescence imaging. (Platforms: PC; Cost: unknown)
MEDx
Medical image visualization and analysis program for MRI, CT, PET, and SPECT. (Platforms: SGI; Cost: unknown)
MetaMorph
Integrated microscope image capture, enhancement, reconstruction, and visualization system. (Platforms: PC; Cost: unknown)
MicroMorph
MicroMorph is the software aid in learning the mathematical morphology techniques of image analysis. (Platforms: PC; Cost: Varies)
MicroVision II
MicroVision II can be used for for visualising point-sampled data volumes. produced by 3D scanning devices such as MRI, PET, CT-scanners and confocal microscopes. (Platforms: PC; Cost: unknown)
MicroVoxel
MicroVoxel is a 3D imaging package that imports data from Bio-Rad MRC-600 files, TIFF files, or raw 8-bit data. (Platforms: PC; Cost: unknown)
Montage
Montage is one of the first complete serial-section reconstruction packages and was produced at the University of Pennsylvania. (Platforms: Sun, SGI, IBM, PC; Cost: free)
Mvox
Mvox is a general purpose tool for visualization and manipulation of a wide range of 2-4D grey level/colour images and 3D surface graphics. (Platforms: SGI, HP, IBM; Cost: $$)
NCSA Tool Suite (DataSlice, Viewit, Tiller)
3D Visualization tools from the NCSA. (Platforms: Sun, SGI, DEC, IBM, Cray, Mac; Cost: free)
Neuro_Echo, Neuro_SPGR, Neuro_Lobe
Neuro_Echo aids analysis of double-echo MR brain scans from the GE Signa imager. The program uses axial scans to segment the brain scans into gray matter, white matter and CSF. (Platforms: Sun; Cost: unknown)
Neurolucida
Interactive image analysis software for neuron tracing and anatomical mapping. (Platforms: PC; Cost: unknown)
NIH Image
NIH Image has painting and image manipulation tools, a macro language, tools for measuring areas, distances and angles, and for counting things. (Platforms: Mac; Cost: free)
Nuages
This is Bernhard Geiger’s (INRIA) reconstruction package. (Platforms: Sun, SGI, DEC; Cost: free)
OLPARS
On-Line Pattern Analysis and Recognition System from the PAR Government Systems Corporation. (Platforms: Sun, DEC; Cost: unknown)
Pixar
High-end visualization and rendering for movies, but also for the medical community. (Platforms: SGI; Cost: $$$)
Pixcell
Pixcell from Sandia Labs. (Platforms: Sun; Cost: free)
PV-Wave
PV-WAVE from Visual Numerics. (Platforms: unknown; Cost: unknown)
RMN
A Nuclear Magnetic Resonance (NMR) data processing program for the Macintosh. (Platforms: Mac; Cost: unknown)
Reconstruction Of Serial Sections (ROSS)
Serial-section based reconstruction and visualization system for microscopy. (Platforms: SGI; Cost: free)
SciAn
Florida State University scientific visualization package. (Platforms: SGI, IBM; Cost: free)
Semper6
General image Processing and acquisition system. (Platforms: PC, DEC, Sun; Cost: unknown)
SGI Explorer
SGI Iris Explorer. (Platforms: SGI, Cray, DEC, HP, IBM, Sun; Cost: unknown)
Sunview
Sunview – available from SunSoft. (Platforms: Sun; Cost: unknown)
SunVision
Sun Visualization software, providing SunIPLib (Image Processing), SunVoxel (volume rendering), SunART (high-quality rendering), SunGV (interactive 3D graphics). (Platforms: Sun; Cost: unknown)
Synu
UCSD reconstruction/visualization program. (Platforms: SGI; Cost: free)
The Explorer
Macintosh-based package from UCLA. (Platforms: Mac; Cost: free)
TIM
Tomographic Imaging- PC Software for 3D image processing of pixel planes. (Platforms: PC; Cost: unknown)
Theraview
No information available. (Platforms: unknown; Cost: unknown)
V
Public-domain software package for magnetic resonance imaging and spectroscopy data. (Platforms: Unix; Cost: free)
Vida
Commercial volumetric display and analysis tool for Unix. (Platforms: Sun, HP, SGI; Cost: $$$)
View
SGI-based program from UNC. (Platforms: SGI; Cost: unknown)
Vis5D
Visualization program for time-varying multi-variate 3-D gridded data. (Platforms: SGI, IBM, Sun, HP, DEC; Cost: unknown)
VisAD
Visualization program for interactively steering and visualizing scientific computation. (Platforms: SGI; Cost: unknown)
VolPack
VolPack is a portable software library for volume rendering. (Platforms: SGI, Sun, HP, DEC; Cost: unknown)
VolVis
Volume Visualization package from SUNY. (Platforms: SGI, Sun, HP; Cost: unknown)
Vox-L
MR and CT visualizer. (Platforms: unknown; Cost: unknown)
Voxblast
Voxel-based 3d volume rendering system developed by Randall Frank at the University of Iowa Image Analysis Facility. (Platforms: SGI, Sun, DEC, HP, IBM, Mac, PC; Cost: unknown)
VoxelBox
3D Volume renderer for Windows. (Platforms: PC; Cost: $)
VoxelMan 3D
Interactive atlas of skull and brain. (Platforms: unknown; Cost: unknown)
VoxelView
VoxelView software from Vital images for 3D reconstruction of images. (Platforms: SGI, Mac; Cost: unknown)
Voxtool
Voxtool from General Electric. (Platforms: PC, Unix; Cost: unknown)
VROOM
VROOM (Vol. Rendering by Object Oriented Meth.). C++ Library. (Platforms: unknown; Cost: unknown)
Wavefront
Wavefront Data Visualizer. (Platforms: SGI, Sun, IBM, HP, DEC; Cost: unknown)
WHIP
General purpose image processing software from GW Hannaway & Associates. (Platforms: SGI; Cost: unknown)
XCOSM
X-Windows interface to Computational Optical Sectioning Microscopy. (Platforms: SGI, DEC, Sun; Cost: Free)
Zmode
Software/hardware that can convert a series of parallel MRI/CT scan images to a 3D reconstructive model in a CAD system. (Platforms: unknown; Cost: unknown)
Appendix B: Use of described technique in two dimensional computed tomography images without contrast
CASE
A 90 year-old female fell from standing. Her family helped her into bed because she complained of feeling weak. She was transported by emergency medical services to a university emergency department where paramedics reported she was “unhelpful” getting from the bed to the gurney. On exam she was found to have complete sensory loss and motor weakness below her neck. Non-Contrast computed tomography (CT) demonstrated possible step off fracture of cervical four and five (C4/C5), with bony fragments in the spinal canal, which radiologically correlated with her clinical signs and symptoms
Post hoc, two dimensional CT images were manipulated using the described technique to produce three dimensional (3D) reconstructions (Appendix B). These reconstructions provided remarkable visualization of the spinal canal. Not only is the vertebral step off at C4/C5 seen in 3D space, but by virtually recreating and highlighting the spinal canal, the location and extent of the acute spinal lesion are easily seen.
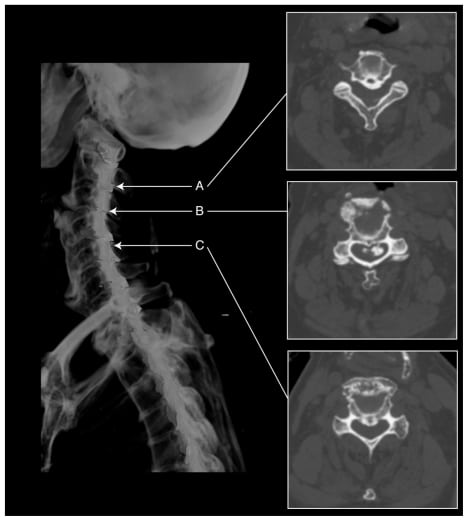
Two dimensional (2D) non-contrast computed tomography (CT) rendered in three dimensional (3D) using the identical data set. Physical examination of the patient confirmed paralysis from the neck, down. 3D rendering of the 2D images correctly identified division of the spinal cord that was not seen on the initial CT and only confirmed by magnetic resonance imaging the next day. A and C demonstrate normal spinal canal and thecal sac alignment. Subluxation of the vertebrae and spinal cord transection at cervical are demonstrated in B.
{kind=link}