
{kind=link}
| Author | Affiliation |
|---|---|
| Nirav Shastri, MD | University of Missouri–Kansas City, Children’s Mercy Hospital and Clinics, Overland Park, Kansas |
| Lauren Olson, MD | University of Missouri–Kansas City, Children’s Mercy Hospital and Clinics, Overland Park, Kansas |
| Milton Fowler, MD | University of Missouri–Kansas City, Children’s Mercy Hospital and Clinics, Overland Park, Kansas |
ABSTRACT
We present a pediatric case report of foot pain due to Kohler’s disease.
A 4-year-old girl presented with intermittent right foot pain for 1 week. Pain had worsened the previous day after playing outside, and she was now refusing to bear weight on the right foot. On examination, she had pain and tenderness over her right dorsomedial midfoot with no local skin changes. She walked with an antalgic gait with weight bearing on the lateral side of the foot. Her right foot radiograph showed a collapsed, flat, and radiodense navicular bone (Figure).
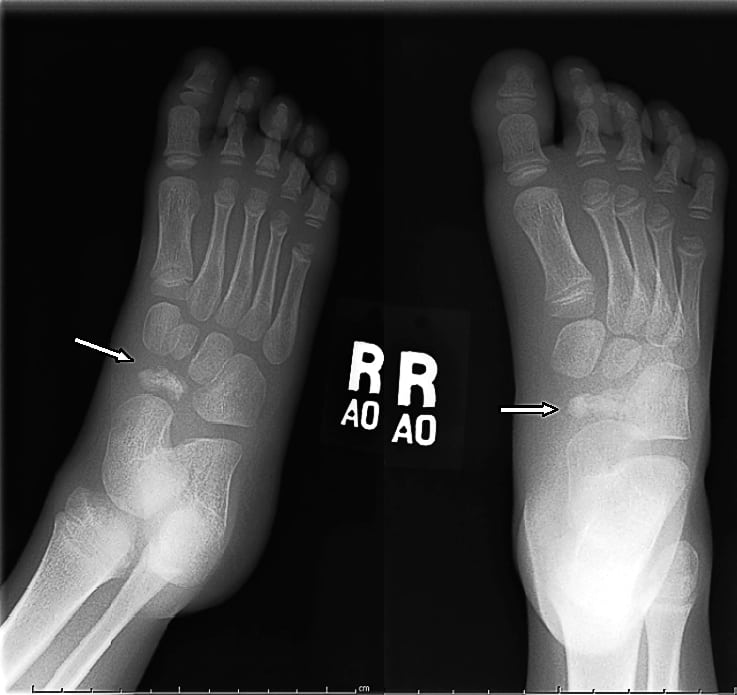
Kohler’s disease is a rare, self-limiting, avascular necrosis of the navicular bone, first described in 1908. It is usually unilateral and most often affects boys. Its usual onset is between 4 to 5 years of age but can present as early as 2 years of age. Girls with this condition are often younger than boys, probably owing to earlier onset of ossification.1,2 The pathophysiology of this condition is best explained by a mechanical cause associated with a delayed ossification. Navicular is the last tarsal bone to ossify and can get compressed between the already ossified talus and cuneiforms when the child becomes heavier. This in turn compresses the navicular bone’s perichondral ring of blood vessels, producing ischemia of the central spongy bone and avascular necrosis. The prognosis remains excellent owing to this radial arrangement of blood supply.1 Radiologic findings show patchy areas of navicular with sclerosis and rarefaction with loss of normal trabecular pattern. Sometimes the navicular may appear collapsed or may be normal in shape with a uniform increase in density with minimal fragmentation. Treatment includes pain control and using soft arch supports or medial heel wedge. Patients with worse symptoms may benefit from a short leg walking cast for 4 to 6 weeks. Symptoms in untreated patients last longer than in treated patients (15 months vs 3 months).2,3 Patients with persistent pain should be examined for other conditions such as talar coalition. Radiographic findings may be normal 6 to 18 months after onset and almost all patients eventually recover excellent function. The type of treatment does not alter the radiographic course of the disease or the final result.3
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted December 23, 2010; Revision received January 5, 2011; Accepted January 10, 2011
Reprints available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2011.1.6691
Address for Correspondence: Nirav Shastri, MD
University of Missouri–Kansas City, Children’s Mercy Hospital and Clinics, 5808 W 110th St, Overland Park, KS 66211
E-mail: nshastri@cmh.edu
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding, sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Vargas B. Kohler disease. 2010. http://emedicine.medscape.com/article/1234753-overvieweMedicine Web site. Available at: Accessed December 10.
2. Borges JL, Guille JT, Bowen JR. Kohler’s bone disease of the tarsal navicular. J Pediatr Orthop.1995;15:596–598. [PubMed]
3. Ippolito E. Ricciardi Pollini TP, Falez F. Kohler’s disease of the tarsal navicular: long-term follow-up of 12 cases. J Pediatr Orthop. 1984;4:416–417. [PubMed]
{kind=link}