
{kind=link}
| Author | Affiliation |
|---|---|
| Erica Chiu Liang, MD | Standord/Kaiser Emergency Medicine Residency Program |
| Jennifer Rossi, MD | Standord/Kaiser Emergency Medicine Residency Program |
| Laleh Gharahbaghian, MD | Stanford University School of Medicine, Palo Alto, CA |
A 61-year-old man presented to the emergency department (ED) with gradual onset shortness of breath exacerbated by lying flat three weeks after undergoing minimally invasive three-vessel coronary artery bypass grafting (CABG). Due to a history of lower extremity deep venous thrombosis, he was taking warfarin, which was held pre-operatively and restarted on post-operative day three along with clopidogrel and aspirin. Prothrombin time was not checked prior to discharge. His vital signs in the ED were notable for an oxygen saturation of 84% on room air improving to 93% with supplemental oxygen. Laboratory testing was remarkable for an international normalization ratio of 24.3, and electrocardiogram showed lateral T wave inversions in V5–V6 but was otherwise unremarkable. A bedside echocardiogram was performed (Figure).
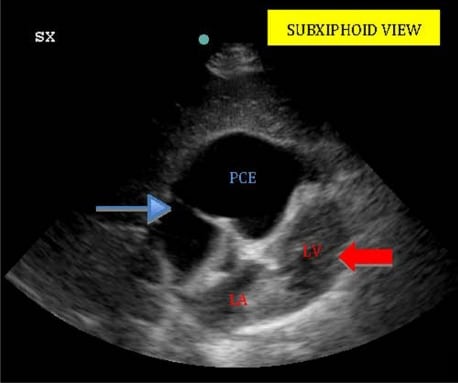
Pericardial effusion is a known complication of cardiac surgery found in up to 85% of patients by postoperative day two and usually begins in the posterior pericardial space in a supine patient.1Persistent pericardial effusion after post-operative day 15 is less common but is associated with a higher incidence of cardiac tamponade, especially in patients receiving anticoagulation therapy.2Minimally-invasive CABG, first described in the 1990s, involves access to the heart via a small anterior thoracotomy incision; however, pericardial effusion and cardiac tamponade are still known complications.3,4 Our patient had a loculated anterior pericardial effusion causing obliteration of the right atrium with diastolic collapse of the right ventricle causing heart failure and his initial complaint of shortness of breath. As shown in the image, the loculations prevented fluid from surrounding the entire heart. His coagulopathy was reversed with 6 units of FFP and 10 units of subcutaneous Vitamin K. Cardiology was immediately consulted, and the patient was taken for emergent echocardiographically-guided pericardiocentesis.
A pigtail catheter was placed in the pericardial space with 500 mL of bloody fluid return. The patient did well post-procedure and was discharged on post-procedure day five.
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted: March 8, 2010; Revision received May 5, 2010; Accepted September 13, 2010.
Reprints available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Laleh Gharahbaghian, MD, Stanford University School of Medicine, 701 Welch Rd., Suite C, Palo Alto, CA 94305
Email: Lalehg@stanford.edu
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Weitzman LB, Tinker WP, Kronzon I, et al. The incidence and natural history of pericardial effusion after cardiac surgery — an echocardiographic study. Circulation. 1984;69:506. [PubMed]
2. Meurin P, Weber H, Renaud N, et al. Evolution of the postoperative pericardial effusion after day 15: the problem of the late tamponade. Chest. 2004;125:2182. [PubMed]
3. Hirose H, Amano A, Takahashi A, et al. Delayed cardiac tamponade after minimally invasive direct coronary artery bypass. Eur J Cardiothorac Surg. 1999;16:487–8. [PubMed]
4. Lazzara RR, Hanlon T, McLellan BA, et al. Cardiac tamponade following minimally invasive direct coronary artery bypass. Chest. 1997;112:1112–4. [PubMed]
{kind=link}